
Abstract
A series of 3 direct-type earthquakes with magnitude ≥6 occurred in the Kumamoto Prefecture, located in the western area of Japan, between April 14 and 16, 2016. Children with food allergies (FA) had difficulty procuring allergen-free meals during this period due to the infrastructure shutdown. We investigated the status of children with FA during the 2016 Kumamoto Earthquake and their behavioral changes after the disaster. We conducted a survey of the parents of 59 children with FA (median: 4 years and 1 month old) who were clinically followed up at our institution. They were questioned about their behavior change to allergen removal and using allergen-free foods during the disaster. Forty-seven (79.7%) children with FA were evacuated immediately after the earthquake and returned to their homes after the restoration of lifelines. Most stayed in their cars, while a few took shelter at public evacuation sites. Thirty-eight children (64.4%) had difficulty obtaining allergen-free food, and 29 children with FA (49.2%) did not have a stockpile at home. Thirty-three children with FA (55.9%) consumed allergen-free foods acquired primarily through relief supplies. Forty-seven guardians (79.7%) insisted that stockpiling allergy-friendly foods at home should be a part of future disaster planning. Stockpiles of allergen-free food were not sufficient in most households. Awareness of self-stockpiling allergen-free foods, reassessing public stockpiling, and establishing a system to provide information regarding relief supplies to evacuees outside evacuation centers are important for disaster planning in children with FA.
Children are vulnerable to disasters such as big earthquakes.
Children with food allergies have difficulty avoiding allergen foods at the evacuation site.
This information in our study became a lesson during a big earthquake.
Our study suggests that allergen-free foods should be stockpiled in public institutions and at homes.
Introduction
Large-scale natural disasters make securing food more difficult than regular times due to suspending logistics and lifelines. 1 It has been reported that lifestyle changes during and after large-scale earthquakes result in significant stress on the body and negatively influence an individual’s overall health.2 -4
Children with food allergies (FA) may be at risk of lowering their intake threshold due to changes in physical conditions and environments, 5 such as living in public evacuation sites. Moreover, it becomes difficult for them to acquire allergen-free foods. 6 Therefore, they must take sufficient precautionary measures and use social support systems during a disaster. 7
A series of 3 direct-type earthquakes with magnitude ≥6 occurred in the Kumamoto Prefecture, located in the western area of Japan, between April 14 and 16, 2016, followed by >4400 after earthquake. 8 This disastrous event resulted in enormous damage to the area centered around Mashiki town, which experienced an earthquake recorded maximum magnitude of 7.3 on the Seismic Intensity Scale of Japan Meteorological Agency (Supplementary Data 1). Since this disaster occurred at night, comparatively less fire damage was evident. Unlike the Great East Japan Earthquake, there were no tsunamis, and this catastrophe was purely an earthquake disaster. 9 Since several residents of Kumamoto Prefecture had difficulty cooking in their own homes post-earthquake due to the destruction of lifelines such as electricity, gas, and water supply, 8 children with FA had more difficulty than usual in terms of safe food intake. 10 Additionally, since some food rations, such as eggs, milk, and wheat, distributed at evacuation centers contained their causative allergens, children and their caregivers were concerned about accidental ingestion. Moreover, some hospitals with emergency departments were also damaged by the earthquake.
There is a paucity of data regarding the status of children with FA during such large-scale disasters.6,9,10 In this study, we investigated the impact of the 2016 Kumamoto Earthquake on children with FA and their guardians to determine precautions that should be taken by children with FAs and their parents in the event of future major disasters.
Methods
Study Participants and Design
We enrolled parents of children with FA aged 0 to 15 years who regularly visited the Department of Pediatrics at the National Hospital Organization, Kumamoto Medical Center, between March 21, 2017, and August 31, 2017. All these participants were residents of the Kumamoto prefecture as of April 16, 2016, and had IgE-dependent FA. The study did not include children living in the southern part of the prefecture (Kuma and Ashikita areas), which was not affected by the 2016 Kumamoto Earthquake. The study objectives and design were explained to the legal guardians of these children, and they were requested to participate in this survey. The participants were not compensated for their time. Subsequently, we asked the guardians to complete the questionnaires (Supplementary Data 2). We developed this questionnaire based on Japanese reports regarding the Great East Japan Earthquake in Japan.9,11 The validity and/or reliability testing was not performed on the questionnaire.
Questionnaires aimed at collecting data regarding children’s age, sex, area of residence, concomitant allergic diseases, evacuation status, and availability of medical care were administered to the guardians. The sex and age of the parents were not examined. In the context of FA, we enquired about the causative food allergens and examined the ingestion status for each allergen. We investigated the ingestion status of allergenic foods among children with FA to hen’s egg, cow’s milk, or wheat and compared it before and after disasters. These are the most common allergens in Japanese children, 12 and those with allergies to these foods often spontaneously remit with age. During this disaster, some children stopped eating foods that they could achieve clinical tolerance before the disaster for fear of allergic reactions during evacuation; such cases as children with FAs were considered in this study. Moreover, some of the study participants with FA were affected by multiple food items. When the same patient had 2 different FAs, such as allergy to hen’s egg and wheat, it was calculated as 2 cases because we considered that the difficulty of elimination diets depended on the allergen. We also asked about FA responses during the disaster.
Infrastructure recovery by evacuation sites and the relationship between food antigens and disaster problems were compared using the Fishers’ exact test. Statistical significance was set at P < .05. All statistical analyses were conducted using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria).
Ethics Approval and Consent to Participate
This study was conducted in accordance with the tenets of the Declaration of Helsinki of the World Medical Association. The study was approved by the National Hospital Organization Kumamoto Medical Organization Ethics Committee (Approval number 705) on March 13, 2017. Written informed consent was obtained from the participants or their legal guardians before the commencement of the study. For this study, the raw data were first extracted, and patients’ identities, including names, patient IDs, and other personal information, were de-identified.
Results
Characteristics of the Study Participants
Fifty-nine children who completed the questionnaire were included in this study. Of the 423 patients who visited the allergy outpatient during the survey period, 300 lived in the affected area. Of these, 287 were eligible for the survey, excluding 13 infants who had not yet been born at the time of the disaster, of which only 20.6% (59/287) were included. Table 1 presents the characteristics of the children with FA included in this study. In all, 30 (50.8%) boys and 23 (39.0%) girls with FA formed our study population. Sex data for 6 children were missing. The median age of children included in this study was 4 years (interquartile range: 2-7 years). Twenty-eight (47.5%) children developed atopic dermatitis, and 11 (18.6%) presented with bronchial asthma. Three (5.1%) children resided in the area which was hit by an earthquake of magnitude 7 (Mashiki town); 42 (71.2%) in areas with 6 upper magnitudes, including the eastern regions of Kumamoto City, Ozu-town, Koshi-city, Uto-city, Uki-city, and Kashima-town; and 13 (22.0%) in areas with 6 lower magnitudes, including the central regions of Kumamoto-city, Mifune-town, Yatsushiro-city, Kikuyo-town, Tamana-city, and Takamori-town (Supplementary Data 1).
Characteristics of the Study Participants.

Fifty-nine participants had affected a cumulative total of 165 cases of FAs, including 24 cases who achieved clinical tolerance. In all, 45 (76.2%, 45/59) children were allergic to hen’s egg, 36 (61.0%, 36/59) to cow’s milk, 24 (40.7%, 24/59) to wheat, 6 (10.2%, 6/59) to soy, 8 (13.6%, 8/59) to fish, 19 to peanuts (32.2%, 19/59), 16 (27.1%, 16/59) to shellfish, and 5 (8.5%, 5/59) to vegetable or fruits (Table 2). Twenty children (33.9%, 20/59) had 1 allergy, 18 (30.5%, 18/59) had 2 allergies, and 21 (35.6%, 21/59) had 3 or more allergies.
Food Items Causing Allergies in 59 Children.

Status of Children With FA During the 2016 Kumamoto Earthquake
Figure 1 shows the evacuation sites for children with FA during the 2016 Kumamoto Earthquake. Forty-seven (79.7%, 47/59) children were evacuated from their houses within a week of the occurrence of the main earthquake, with 25 of these children staying in their cars. Thirteen children were evacuated to public sites (N = 3) or their cars (N = 10) from their homes only at night. The number of families evacuated only at night was 13 (22%), 7 (12%), and 3 (5%) cases within 1 week, 2 to 3 weeks, and 4 weeks after the disaster, respectively (Data not shown). Children gradually returned to their homes a week after the main earthquake. Four weeks after the main earthquake, only 14 (23.7%, 14/59) children remained at the public shelter (N = 2) or relatives/friends’ houses (N = 12). Eight (13.6%, 8/59) families never moved to the evacuation sites since they were concerned about exacerbating their child's allergic disease.

Evacuation site after the main earthquake (59 children).
Figure 2 shows the recovery rates of the lifelines. Recovery of electricity, gas, and water supply services was described by 53, 41, and 55 guardians, respectively. Electricity services were recovered in 42 (79.2 %. 42/53) homes within a week of the main earthquake. However, gas and water supply services were recovered only in 20 (48.8%, 20/41) and 22 (40.0%, 22/55) homes, respectively. It took 4 weeks to achieve 90% recovery of all the lifelines. We compared the evacuation sites of children 2 weeks after the earthquake with the restoration of infrastructures at that time. The gas restoration rate for the families who evacuated to a friend’s house was 35.0%, lower than for those who evacuated in their cars (62.5%, P = .231) or for those who did not evacuate (39.2%, P = 1.000) (Data not shown). The water restoration rate for families who evacuated to a friend’s house was 35.0%, also lower than for those who evacuated in their car (75.0%, P = .096) or for those who did not evacuate (60.7%, P = .142) (Data not shown). Therefore, the families whose infrastructure was not restored were more likely to evacuate to a friend’s house, which could provide electricity, gas, and water to serve safe foods for children.

Recovery rates of infrastructure after the main earthquake. (Electricity: N = 53, Gas: N = 41, Water: N = 55).
Measures Taken During the 2016 Kumamoto Earthquake
Concerning the routine medical visits during the 2016 Kumamoto Earthquake, 5.1% (3/59) of guardians could not visit the hospital due to impaired road status, defects in transportation measures, and unknown hospital status (Data not shown). However, they believed that their children should have visited the hospital. Subsequently, 6.8% (4/59) of patients visited a medical facility other than their family doctor and 27.1% (16/59) did not need medical care.
We investigated the ingestion status of allergenic foods among children with FA to hen’s egg, cow’s milk, and wheat (Figure 3). Out of the 59 study participants, 56 children (94.9%) had presented allergies to 3 major allergen foods, such as hen’s egg, cow’s milk, or/and wheat, or had histories of these allergies. Additionally, we observed a cumulative total of 105 FA cases of hen’s egg (n = 45), cow’s milk (n = 36), or wheat (n = 24) among the 56 children, with those having 1 to 3 allergies (Table 2). Of the 14 participants (hen’s egg allergy: 4 cases, cow’s milk allergy: 3 cases, and wheat allergy: 7 cases) who outgrew their FA and could routinely ingest allergen foods before the earthquake, 3 (hen’s egg allergy: 1, cow’s milk allergy: 1, and wheat allergy: 1) decreased the intake volume of allergen foods during the earthquake disaster (Figure 3). Of the 50 cases (hen’s egg allergy: 23, cow’s milk allergy: 17, and wheat allergy: 10) who could consume medium or low doses of allergen food but had not completely outgrown them, 27 (hen’s egg allergy: 13, cow’s milk allergy: 8, and wheat allergy: 6) did not eat the causative foods at all. In contrast, 9 (hen’s egg allergy: 5, cow’s milk allergy: 3, and wheat allergy: 1) intensified the restriction of these food items (Figure 3). Forty-one elimination cases (hen’s egg: 18 cases, cow’s milk 16 cases, wheat 7 cases) continued avoiding the intake of allergen foods before and after the earthquake. Guardians of these children restricted the intake of allergen foods due to various concerns, including anxiety about an allergy threshold reduction resulting from poor physical condition (40.7%, 24/59), emergency response in acute allergic reactions (37.3%, 22/59), concerns about symptom induction for food allergens (27.1%, 16/59), effect on family members caused by the development of allergic symptoms (13.6%, 8/59), effects of the shelter environment on the development of allergenic symptoms, with instances such as some of the children receiving sweets containing allergens from evacuees who were not family members while they were in the shelter (5.1%, 3/59), and anxiety about drug shortages (8.5%, 5/59) (Data not shown). Only one child with cow’s milk allergy visited a medical facility for accidental ingestion of dairy products.
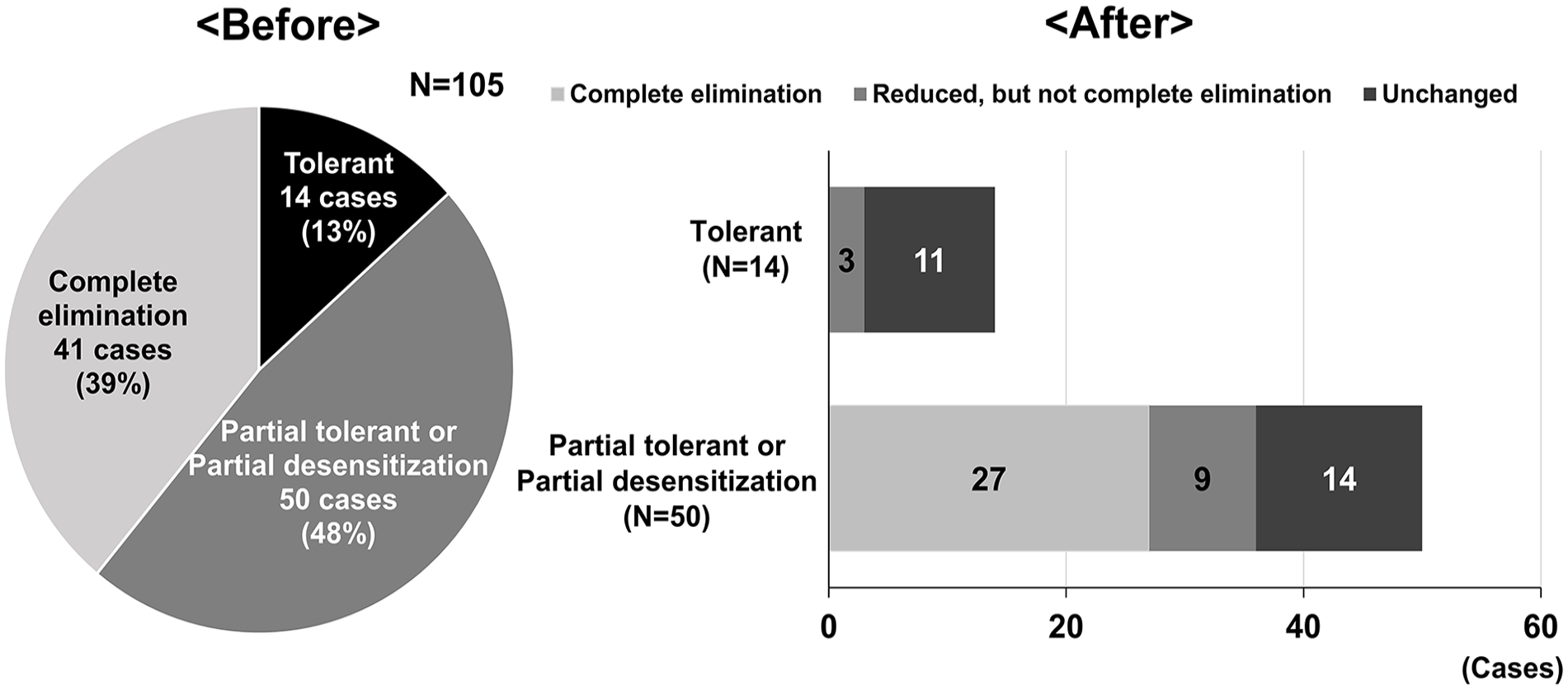
Left: consumption status of allergen foods before the main earthquake (105 cases in 59 children). Right: consumption of allergen food after the main earthquake (64 cases that had achieved clinical tolerance or partial desensitization to the causative foods).
Thirty-eight (64.4%, 38/59) guardians considered procurement of allergen-free food as the essential of disaster (Figure 4). More parents answered this problem in the cases with multiple food allergies (30/39) than those with 1 food allergen (8/20) (P = .006). Limited to hen egg, milk, and wheat allergies, more cases with 2 or more of these allergies (25/30) pointed out food procurement as a problem than those with 1 or fewer (13/29) (P = .001, Data not shown). The more food allergens a child had, the more difficult it was for them to avoid food allergens. Thirty-three (55.9%, 33/59) guardians used allergen-free foods for their children with FA during the disaster. Twelve (20.3%, 12/59) guardians could not use allergen-free food but wanted to use it, while 14 (23.7%, 14/59) did not need it. Of the 33 children who used allergen-free food, 23 (69.7%, 23/33) received social support supplies from the government or charitable organizations for allergen-free foods (Data not shown). Twenty-two children (66.7%, 22/33) received support from friends and acquaintances, 18 purchased them themselves, and only 5 (15.2%, 5/33) lived through the disaster period using stockpiled allergen-free foods. Twenty-nine (49.2%, 29/59) guardians had not stockpiled allergen-free foods (Figure 5).

Issues faced by children with food allergies (59 children) (A guardian could give multiple answers).

The status of stockpiles at home.
Awareness of Precautionary Measures to be Taken During Disasters After the 2016 Kumamoto Earthquake
We investigated the awareness of precautionary measures to be taken during disasters after the 2016 Kumamoto Earthquake. Forty-seven (79.7%, 47/59) parents of children with FA contemplated the need to store allergen-free foods in their homes, 45 (76.3%, 45/59) considered the need to store allergen-free foods in public institutions, and 44 (74.6%, 44/59) considered the need of information about where to obtain allergen-free food (Figure 6).

Disaster precautions for food allergy (A guardian could give multiple answers).
Discussion
We conducted a survey of children with food allergies and their guardians who were affected by the 2016 Kumamoto Earthquake using a questionnaire to learn from their experiences and take future measures for children with FAs in large-scale disasters.
It is challenging to obtain allergen-free foods during a disaster. In the survey about food and nutrition issues after the Kumamoto arthquake 6 and the Torrential Rain Disaster in Western Japan, 13 Tsuboyama et al reported that FA was a prolonged problem in the disaster area. This problem did not appear immediately after the severe damage occurred in the affected disaster areas. Their report suggested that considerations for FAs might have been impractical in these severely damaged regions because more immediate and pressing concerns have appeared. 6
All the children in this study experienced an earthquake of magnitude ≥5, and 70.3% of them had difficulties obtaining food that they could eat. Almost 80% of children with FA in this study were evacuated, and the restoration rate of gas and water was lower among those living in their cars and those who did not evacuate compared to those living with relatives/friends. Moreover, the number of evacuated children decreased with the recovery of lifelines. Therefore, it is suggested that the place where parents having children with FA were evacuated depends on the damage level of the lifeline.
Within a week after the Kumamoto Earthquake, the family vehicle was the most common evacuation site for children with FA. Only a few took refuge in public evacuation sites. Many people evacuated only at night for fear that their homes would collapse while they were sleeping. 8 Most of the study participants were infants (median 4 years old). Several families with infants refrained from evacuating because they were crying at night or due to difficulty in breastfeeding. 14 Children evacuated in their cars (12%, 3/25) were less likely to receive public assistance compared to those evacuated to shelters (25%, 2/8) (P = .078) (Data not shown). These results suggest that support (such as the supply of allergen foods for children with FA who took refuge outside the shelters) should be considered. Kumamoto prefecture also reported that many people took shelter in their cars and yards during the disaster and that there was a lack of relief supply support and information provision because it was impossible to fully grasp the actual situation of evacuees outside the evacuation shelters. 8 A week after the disaster, the main evacuation sites changed to the homes of relatives and acquaintances. Several guardians of children with FA insisted on the importance of catering to the needs of children with FA. Tsuboyama et al reported that cooking utensils and gas supplies were essential for improving meals at evacuation sites during the 2011 Great East Japan earthquake. 10 Therefore, it is likely that evacuation sites were changed to the homes of relatives and acquaintances because guardians could move with improved road conditions and needed an environment where they could cook using water or gas.
More than half of the guardians strengthened the removal of allergenic foods during the disaster period. This may have resulted from enhanced anxiety about anaphylaxis, which may be induced by deterioration in their physical condition under a stressful disaster environment. Only one child case of FA anaphylaxis was reported. This child, who was on an elimination diet (partial elimination) at the family’s discretion, was drinking only water but got tired of it and drank juice with milk protein exceeding the threshold level, resulting in hives and wheezing. However, the child recovered after the use of epinephrine. Accidental ingestion in children with FA was also reported after the 2011 Great East Japan Earthquake. 9 Managing children with FA in a disastrous environment, where it is difficult to obtain allergen-free food and medicines, is an arduous task. Therefore, the mental burden on the guardians is heavy.
Many guardians (64.4%, 38/59) responded that food procurement was an important concern when dealing with FA during a disaster. However, half of the households with children having FA (29/59) did not stockpile food at home. They understood that home stockpiling of allergen-free foods is the most important countermeasure for future disasters.
Children with FA staying outside the evacuation sites had less chance to get some food compared to those residing in public evacuation sites. 14 Even in public shelters, some children could not get allergen-free foods. Private relief supplies and self-purposes provided allergy-friendly foods for the children. Since many children with FA did not evacuate to the public evacuation sites, the municipality had difficulty gauging the status of residents outside the public evacuation sites, such as residents staying in their cars, which made providing relief supplies and information more challenging. 8 Therefore, it may be important for the municipality to create a system that allows food allergy sufferers to send out an SOS or access information on relief supplies in an emergency by using social networking services.
Rice allergies in children have rarely been reported in Japan, 12 and rice can be consumed by most children. Therefore, increasing public food stockpiles, especially of rice, may be important. Bread, not rice, was often supplied at evacuation sites. Since many children with FA are allergic to hen’s eggs, cow’s milk, or wheat 12 allergies could not consume it. The Kumamoto municipalities regularly had stockpiled alpha rice, a pre-cooked and dehydrated rice. 15 However, children with FA preferentially could not receive alpha rice even in public services because alpha rice was supplied for people in the disaster area, and people without FA also ate it. 14 The municipal government should stockpile alpha rice sufficiently.
More parents faced problems with food procurement in cases with more than 1 food allergen. Practically, 31 (52.5%, 31/59) guardians indicated the importance of a definite diagnosis of the causative food allergen. Many partially tolerant children with FA who could eat small amounts of allergen foods reduced their intake volume during the earthquake. Children with FA and their guardians were more concerned about dealing with symptoms they may develop during the disaster. Moreover, an appropriate identification of FA is also needed because undiagnosed or unintroduced FAs are often suspected as real food allergens.
This study had a few limitations. Since this study included guardians residing in the area significantly impacted by the earthquake, emotional bias may have been involved. Moreover, since the survey using the questionnaire was anonymous, we could not compare the difficulty level of dealing with FA based on the severity of the allergy. However, this study contains important considerations that should be addressed in the future as a measure for children with FA during disasters.
Conclusion
Children with FA require immediate food assistance during large-scale disasters. During the hyperacute phase until recovery of lifelines and roads, allergen-free foods should be stockpiled in public institutions and at homes. In addition, since some families with children may take refuge outside public evacuation sites, municipalities should establish a system to provide information on relief supplies to them as a part of disaster countermeasures.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241248100 – Supplemental material for Disaster Preparedness for Children With Food Allergies During the 2016 Kumamoto Earthquake—Observational Study
Supplemental material, sj-docx-1-inq-10.1177_00469580241248100 for Disaster Preparedness for Children With Food Allergies During the 2016 Kumamoto Earthquake—Observational Study by Mariko Nagayoshi, Mika Ogata, Nami Hirai and Jun Kido in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-2-inq-10.1177_00469580241248100 – Supplemental material for Disaster Preparedness for Children With Food Allergies During the 2016 Kumamoto Earthquake—Observational Study
Supplemental material, sj-jpg-2-inq-10.1177_00469580241248100 for Disaster Preparedness for Children With Food Allergies During the 2016 Kumamoto Earthquake—Observational Study by Mariko Nagayoshi, Mika Ogata, Nami Hirai and Jun Kido in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to thank the members of the Japanese Society of Pediatric Allergy and Clinical Immunology for their valuable advice in preparing the questionnaire.
Author Contributions
MO and JK designed the study. MN, MO, NH, and JK contributed to data collection. MN, MO, NH, and JK checked and analyzed the data. MN, MO, and JK wrote the manuscript. MO and JK supervised the study. All authors read and approved the final manuscript for submission. All authors have agreed to be personally accountable for the author’s contributions and to ensure the accuracy or integrity of any part of the work.
Availability of Data and Materials
This dataset is available with the permission of the responsible author and the National Hospital Organization Kumamoto Medical Organization Ethics Committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the tenets of the Declaration of Helsinki of the World Medical Association. The study was approved by the National Hospital Organization Kumamoto Medical Organization Ethics Committee (Approval number 705) on March 13, 2017. Written informed consent was obtained from the participants or their legal guardians before the commencement of the study. For this study, the raw data were first extracted and patients’ identities, including names, patient IDs, and other personal information were de-identified.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.