
Abstract
Three organizations in Clark County, WA, partnered together to implement a pilot program to expand access to personal caregiving services in the homeless crisis response system. The aim of this study is to describe staff and clients’ experiences of the program and its impact on clients’ daily living activities, health and wellbeing, and housing stability. Using a qualitative descriptive design, semi-structured, in-depth interviews were conducted with 12 clients and 5 pilot staff, representing 4 housing service providers. Interviews were analyzed descriptively to examine staff and clients’ perspectives and experiences with the personal care services pilot program. Caregivers helped clients establish routines, find companionship, and connect to health and social services both logistically and socioemotionally, supporting clients’ stabilization and reducing barriers to healthcare. Hiring and retaining caregivers remained difficult due to the challenging nature of the work. Staff interviews highlight the need for additional supports to better retain caregivers. Findings from the evaluation have important implications for addressing the needs of individuals exiting homelessness and suggest that personal caregivers can play an important role in supporting the stabilization process. However, employing strategies such as training and increasing wages and benefits that support the needs of the caregiving workforce is essential to sustain this type of service delivery model.
Personal caregiving supports can help older adults and people with disabilities successfully achieve daily living activities, prevent further disability, and decrease reliance on institutional care.
Interviews with clients and staff implementing the caregiving pilot program help demonstrate how expansion of personal care services into the homeless crises response system helps clients establish more stability in their day-to-day lives, and positively contributes to their physical health, mental well-being, and housing stability.
Our results support increased integration of personal caregiving services into the homeless crises response system while also highlighting the need for strategies aimed at increasing economic incentives, improving training processes, and acknowledging the key role of caregivers among staff teams to more fully support caregivers in their work.
As the experience of homelessness becomes more prevalent across the globe, identifying effective strategies to support exits from homeless becomes ever more urgent.1,2 For many people exiting homelessness can be a complex process, that may be further exacerbated by increased levels of disability and morbidity that frequently accompany the experience of homelessness. 3 The social and economic challenges faced by people with experiences of homelessness such as poverty, trauma, social exclusion, and inadequate nutrition contribute to poor health and disability.4,5 As such, individuals transitioning into housing from homelessness may require additional supports to complete activities of daily living (ADLs) (e.g., food preparation, bathing, dressing, toileting, walking, etc.) as well as more instrumental activities of daily life (IADLs) (e.g., transportation to pharmacies and other appointments).6 -8 This is increasingly true as the number of older adults experiencing homelessness grows.9 -11
Caregiving supports can help individuals successfully achieve daily living activities, prevent further disability, and decrease reliance on institution care. 12 Yet, the caregiving needs of people with experiences of homelessness often go unmet. A recent study of adults ages 50 and older with experiences of homelessness found that more than 80% had a caregiving need but fewer than 20% of those with a need received assistance. 13 Moreover, experiences of homelessness can impede people’s access to needed caregiving assistance. For example, facets of the homeless experiences, such as social network disruptions, trauma, and behavioral health disorders, can limit access to informal caregiving (i.e., unpaid assistance from family and friends). 14
There are also barriers to integrating formal caregiver services into some types of housing that support people with experiences of homelessness. Through its Home and Community Based Services program, Medicaid offers a range of assistance to qualified persons with disabilities and chronic conditions to enable them to accomplish ADLs and IADLs. 15 Historically, these types of programs have been provided to elderly and disabled individuals who need additional assistance to remain in their own homes and communities rather than moving to an institutional setting such as a nursing home. 15 To-date however, integrating caregiving services into housing settings such as shelters or permanent supportive housing sites has been limited. This is due in part because the federal rules for demonstrating benefit eligibility for formal caregiving services are complex. 16 Moreover, administering the qualification assessment in these housing contexts can be difficult due to the Medicaid payment structure for caregiving services (caregivers are not incentivized for caring for individuals with more complex needs) and the eligibility process (individuals need to demonstrate a need for services, this can be challenge for people with experiences of homelessness who may have limited social support networks to provide needed assistance). 16
Recognizing this gap in caregiving services, Council for the Homeless, a non-profit organization that works to prevent and end homelessness in Clark County, Washington, partnered with the Vancouver Housing Authority and CDM Caregiving Services to pilot a program that expanded access to caregiving services by connecting individuals transitioning into housing with a caregiver aide. The pilot program prioritized senior clients and clients with complex medical needs. The purpose of this study is to understand the experience of staff and clients participating in the pilot program as well as its impacts on clients’ day-to-day living activities, health, and housing.
Methods
This study used a qualitative descriptive design to assess the impacts and experiences of individual engaged in the pilot program. Data for the study come from in-depth interviews conducted with clients, housing staff members, and caregiving staff members engaged in the caregiving pilot program at 4 housing sites collected between July and November 2021. The Providence Health and Services Institutional Review Board (#2021000402) approved all study protocols. Participants provided verbal informed consent prior to enrollment in the study. Providence Health and Services Institutional Review Board determined the study to be minimal risk and waived the requirement for written consent.
Recruitment and Data Collection
Staff recruitment
Council for the Homeless personnel provided a list of housing supervisors at 5 participating housing sites in the pilot program as well as caregiver supervisors. CDM Caregiving Services provided a list of caregivers staffing the pilot program. We prioritized outreach to supervisors from the 2 types of housing sites involved (i.e., supportive housing and shelter settings), caregiver supervisors, and caregivers. A member of the research team contacted participants via email to determine interest and schedule interviews. Supervisors were considered non-responsive after 2 outreach attempts and caregivers after 3 attempts.
Trained members of the research team (SR, a female PhD research scientist; KM, a female Master’s-level research associate) conducted interviews with housing and caregiving staff over a video conferencing application. Using a semi-structured interview guide, interviews focused on understanding staff perspectives regarding pilot program implementation, caregiver day-to-day experiences, and how the program had impacted clients. No staff participants refused to participate or dropped out during the study. Interviews lasted approximately 60 min. No one else besides the research team and staff participants were present during the interviews. Notes and observations from the interview were compiled by the interviewer after each interview was completed. No repeat interviews were conducted.
Client recruitment
To be eligible to participate in an interview, clients had to be 18 years of age or older, speak English proficiently enough to give informed consent and participate in the interview, and have received caregiving services through the pilot program. Using convenience sampling approach, housing supervisors at 3 sites, 2 permanent supportive housing sites and 1 shelter site, provided study information and flyers to eligible clients and offered a private, quiet space with a telephone for interviews.
Members of the study team (SR, KM) held a total of 24 drop-in interview hours across 6 different days when clients could call an interviewer via telephone and participate in the interview at their convenience and discretion. Drop-in hours were offered until data saturation was reached. The decision to use drop-in hours to conduct the interviews was made in collaboration with housing staff supervisors. This population is often very challenging to reach and engage in research, and the drop-in interview format provided increased flexibility and access for clients to participant in this study. Prior to beginning the interview, the study team confirmed that each participant met the eligibility criteria and confirmed participation consent verbally. During study planning housing staff suggested that verbal consent was more appropriate for the population as individuals in these settings had limited access to the resources needed to provide written consent in a remote environment. No client participants refused to participate or dropped out during the study. Interviews followed a semi-structured interview guide that centered on clients’ relationship with caregivers and the impact participation in the pilot program has had on their daily living activities, health and well-being, and housing status. Interviews lasted between 20 and 45 min. A housing case manager was present during 2 interviews to support the study participant during the interview. All other interviews were completed with just the research team and study participant present. Notes and observations from the interview were compiled by the interviewer after each interview was completed. No repeat interviews were conducted. Participants received a $60 grocery store gift card as compensation for their time and expertise.
Analysis
Data were analyzed using a qualitative descriptive approach which stays close to the data and is less interpretive than approaches like grounded theory, or phenomenology. 17 This allowed us to focus on the individuals’ lived experiences of the program and supported pattern identification within and across interviews. Each interview was audio recorded and transcribed verbatim. The research team then reviewed the transcripts for accuracy.
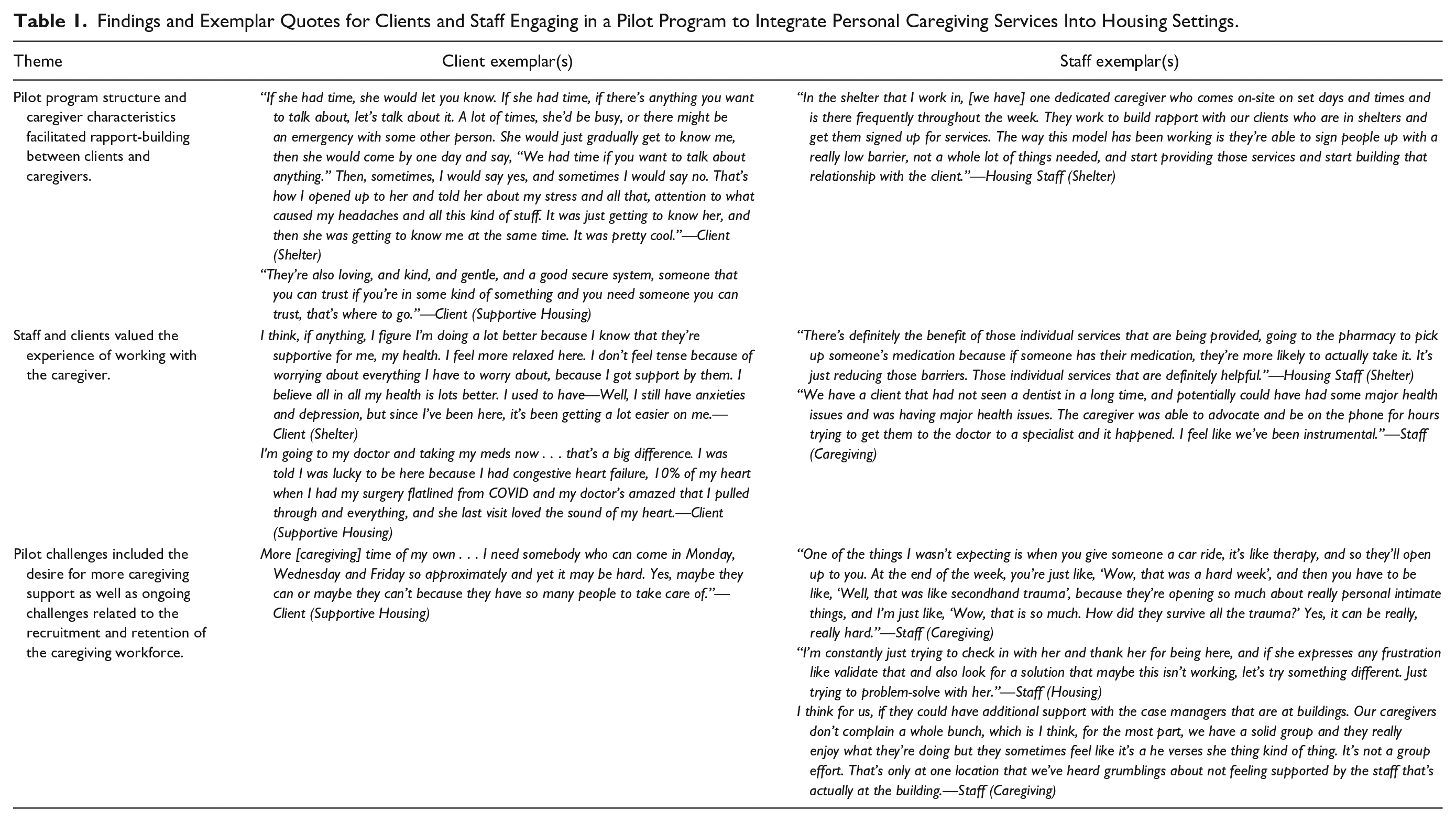
Separate codebooks were developed for the staff and client interviews. Each initial codebook was developed from the interview guide and revised iteratively as emergent codes were identified. To help maintain methodological and analytical rigor, 2 members of the research team (SR, KM) independently coded the transcripts. After each round of coding, the coding team met to discuss codes until consensus was reach. Six of the interviews were double coded to ensure consistency and reliability. The research team reviewed the content of each code to develop a set of central themes. Main themes and subthemes were identified through discussion between the coder team and not finalized until the research team reached consensus. Illustrative quotes are presented in the results section to support the themes and subthemes. In addition, verbatim quotes are provided in Table 1 to further validate findings. All analyses were completed in Atlas.ti version 9.0. 18
Findings and Exemplar Quotes for Clients and Staff Engaging in a Pilot Program to Integrate Personal Caregiving Services Into Housing Settings.
Results
Five staff engaged in the caregiver pilot program participated in an interview. Two staff members worked in the housing sector as staff supervisors (1 supportive housing site, 1 shelter site). Three staff worked at the caregiving staffing organization: 2 served in a supervisory role and 1 worked in the pilot as a caregiver.
In total 12 clients completed an interview. Four of the interviewees lived at a supportive housing site. Eight of the interviewees were currently staying at a housing shelter.
Altogether, interviews with clients and staff implementing the pilot program demonstrate how the expansion of personal care services into housing settings like permanent supportive housing and shelters, helped clients establish more stability in their day-to-day lives. The structure of the program allowed for more consistent engagement between caregivers and clients which facilitated rapport-building. At the same time, the characteristics of the caregivers themselves further encouraged client engagement. With this foundation of trust, caregivers served as a bridge supporting clients’ connection to other service providers both logistically and socioemotionally, and positively contributed to their physical health, mental well-being, and housing security. Yet, several challenges persist in the pilot, especially staffing and the need for additional training for caregivers tailored to the population. Additional exemplar quotes are provided in Table 1.
Theme 1: Pilot Program Structure and Caregiver Characteristics Facilitated Rapport-Building Between Clients and Caregivers
Program structure
For clients, the convenience and ease of access to caregiving services greatly contributed to their participation in the program. Caregivers worked with clients at regular intervals, ranging from daily to twice a week, depending on caregivers’ schedules and clients’ needs. Clients described how caregivers would check in daily to see if they needed help or had questions.
I’m very shy talking to people. [Pilot caregivers] . . . gave me time to get used to it. I’ve always done things on my own, try to, but I realized I needed the help and I asked for it, and ever since they’ve been helping me pretty good.—Client (Shelter)
The fact that caregivers initiated many of these interactions alleviated some stress for clients and helped draw in clients who were initially hesitant to work with caregivers. Staff noted that having a consistent caregiver at a housing location helped to establish trusting relationships with clients, Initially, as you can imagine with this population, there’s a lot of trust issues and a lot of concerns about potentially being stolen from, et cetera. Much of what our caregivers did early on was simply be there and chat with somebody who came by and offer services, whether it be going to get a food box at the food bank or maybe going to pick up medications, that kind of thing, and slowly develop relationships with some of the residents there. Then next thing we know they’re signing up to provide to get help. Now my caregivers have very little downtime, they’re pretty much running from the minute they get there all the way up until the time they leave, staying busy, and continuing to develop relationships with the folks who are living in these shelters.—Staff (Housing)
Staff also identified that a challenge of having an on-site caregiver was that the day-to-day needs of clients fluctuated, leaving caregivers very busy some days and not very busy other days.
Caregiver characteristics
In addition to facets of the program structure supporting caregivers in building trust with clients, various characteristics of the caregivers also facilitated their work with clients. Clients described caregivers as approachable, calming, always being willing to listen and help, and having genuine concern for their wellbeing. Clients also cited caregivers’ patience, reliability, and consistency in following up as factors that helped them connect. As one client described, She’s got a really laid-back attitude. She’s really down to earth and she’s upfront with everything, she doesn’t pull no punches. She’s straight up with everything. “If you don’t do this, this is going to happen. If you don’t do this, this is going to happen.” I like that about her.—Client (Supportive Housing)
Staff described caregivers as friendly with positive attitudes, honest and straightforward, proactive, and perceptive of the clients’ needs. One staff member talked about an encounter 1 caregiver had with a client using substances and how the caregiver’s personal qualities eased the situation, I think it’s part of her personality. Things don’t phase her, but I know that that’s not everybody and that I worked with other caregivers who are not that way. Luckily, she walks in and she’s like, “Oh, cool. Okay. Yes. Well, I’ll just come back, you come get me when you need me.” I’m like, she just really chill about it, and I was like that’s awesome. That’s great. Because if you would have shown fear or maybe anger, I could see someone getting really upset and being like, “You’re going to tattle on me?,” or escalate a little bit.—Staff (Housing)
Theme 2: Staff and Clients Valued the Experience of Working With the Caregiver and Felt it Had a Positive Impact on Housing Clients’ Day-to-Day Lives and Wellbeing
Caregivers helped clients to establish more regular routines in their daily lives, which contributed to their overall health and well-being. Similarly, staff talked about how caregivers supported clients in building the necessary skills for an independent, housed life.
Activities of daily living
Clients and staff described how caregivers assisted with activities of daily living such as cleaning, meal preparation, dressing, bathing, and grooming, as well as assisting with making appointments and arranging transportation. Clients highlighted transportation to various locations like the grocery store, pharmacy, medical or dental appointments, or public transit stops as a key component of their work with their caregiver. One client described his work with the caregiver accordingly, Just helping me stay on top of things, like my laundry or stuff like that. She helps a lot. Grocery shopping, keeping my house clean. It’s so much nicer having her clean the house. It really is.—Client (Supportive Housing)
Staff also described examples of times when caregivers supported clients with some system navigation such as securing a social security card or a driver’s license. One staff member explained, As you talk to people, there has been a lot of success stories and the caregivers that work this program care about these individuals so much and will navigate whatever systems and be on the phone and try to get them into doctor’s appointments or advocate for them or get into social security. Get their driver’s license. They’ve done so much.—Staff (Caregiving)
While some clients talked about not necessarily needing this type of support from the caregivers, they also described feeling like they could ask for this type of help if the need arose. From the staff perspective, this type of support from caregivers was especially helpful for clients whose personal care needs extended beyond the scope of regular housing site staff, as having trained caregivers onsite helped alleviate these additional responsibilities. As 1 staff member described, When we have a client who needs assistance with the ADLs, that’s something that shelter staff are not trained or equipped to handle really. In the past, sometimes that has fallen on staff and that can be difficult, difficult because we may be asking them to do things that they’re really not trained to do which can be unsafe or just outside of their role which is hard for someone. It also just detracts from their ability to do the rest of their job.—Staff (Housing)
Health
Clients talked about how caregivers supported them in establishing more regular habits with things like eating and going to medical/dental care providers, which in turn contributed to improvements in physical well-being. From the staff perspective, getting clients connected with physical health services was a huge need at the onset of the program and has been one of the biggest benefits of the pilot program.
There’s definitely the benefit of those individual services that are being provided, going to the pharmacy to pick up someone’s medication because if someone has their medication, they’re more likely to actually take it. It’s just reducing those barriers. Those individual services that are definitely helpful.—Staff (Housing)
Clients highlighted prescription medication management as a primary support provided by the caregivers. This included picking up prescriptions at the pharmacy, organizing multiple medications, and reminders to take medications. For multiple clients, improving adherence to prescription medications led to feeling physically healthier. As one client described, I was hesitant at first because I’m not used to getting help, but I would probably talk to her just about every day. I had a bad problem of not taking my medications and staying on schedule because I was out in the tent world and then once I came here she really worked close with me and made sure that I took my medication on time and she made me more aware and its helped my health tremendously.—Client (Shelter)
A few clients also described how improvements in physical health from their work with the caregiver has led to improvements in mental health and vice versa. Only one resident felt that the pilot project had not had an effect on his/her physical health.
Additionally, clients and staff identified the mental health benefits of the companionship caregivers provided. As one staff member explained, I . . . have some people who want to be checked on. They want to be heard. That’s the one thing I really enjoy about [the Caregiver] . . . she just stops by just like, “How are you doing?” She ends up telling them about her grocery trip and her taking her kid to 4-H. I think they just like that, not feeling so alone, which is great. With 46 people, I’m from one unit to the next, just in a circle. It’s nice to have another caring face to come in and check with them.—Staff (Housing)
For clients, the caregivers acted as a trusted individual to talk to about things going on in their lives. Having this outlet for their day-to-day stressors and tensions was helpful and contributed to reports of improved mood; reduced depression, anxiety, and stress; as well as a more positive outlook for the future. One resident talked about how the positive socioemotional support provided through the caregiver has helped him to maintain his sobriety.
I think the most positive I got from [the caregivers] is that they see me staying sober, and they look forward seeing out how I'm staying away from the drugs because this place down here is drug-infested, They give me a lot of compliments . . . also is hard to believe seeing how I could stay sober down here and off of drugs when it’s so available. Just their support, it really strengthened me a lot.—Client (Shelter)
Housing
While some staff and clients felt that caregivers had not specifically contributed to their housing situation, others described how caregivers have been able to help clients avoid negative exits from housings and supported overall housing stability. Clients included examples of caregivers helping them to avoid fights with other clients, improve attitude, keep their residence clean, and facilitate difficult roommate situations (e.g., roommate with body lice).
She kept me from getting in a fight. I got in an argument with another resident, and she said, “Calm down and walk with me to walk it off.” She stopped me a couple of times that I probably would have lost my housing.—Client (Supportive Housing)
One staff member talked about how the caregiver at her site has been critical in supporting residents’ successful transition from shelter into permanent housing: I can think of a couple of clients that we’ve recently had in shelter who may, and I can’t say for sure, I think definitely could have ended up in negative exits where we had to exit someone either to the hospital or just to a place not meant for habitation so a car or outside because they weren’t able to successfully live in shelter. They weren’t able to meet our guidelines, they weren’t able to meet their basic needs, whatever that might be and I think that having caregiving services has allowed some of those people to remain in shelter for long enough to move into housing.—Staff (Housing)
Theme 3: Pilot Challenges Centered on the Recruitment and Retention of the Caregiving Workforce
Clients and staff drew attention to the fact that the demand for caregiving services outweighed the current availability of pilot caregivers. One client discussed his desire to have greater caregiver availability, I wish it was run seven days a week . . . I don’t whether it’s because they’re just shorthanded or whether it has anything to do with the COVID thing or what. Usually, it’s on Saturdays. Saturday there’s nobody here, and there’s nothing you can do about it. If have to get something done, you have to do [it] yourself . . .—Client (Shelter)
While the demand for services in the pilot program was high, filling open caregiving positions was an ongoing challenge. One staff member described the staffing challenge, I know the staffing levels are down, so there’s a lot of need and there’s not a lot of people to fill the job . . . I only have one caregiver who’s rotating in this on-call position. She’s between multiple buildings and she also has permanent clients. She’s multitasking. I feel like there’s a lot of people who could use more support here, but there just aren’t the people . . .—Staff (Housing)
Staff also described one potential barrier to recruitment and retention of pilot caregivers being the challenges of providing services in these settings. The needs of clients greatly differed from the typical caregiving clientele, noting fewer physical needs, and more trauma and behavioral health concerns. One staff member talked about the differences between usual caregiving clients and clients engaged in the pilot, This is so fundamentally different because we’re working with a number of folks who are not really physically disabled, but they’ve been on the streets so long that they don’t know how to do some of the common things that you and I do. Learning, only to do laundry again, learning to shop, learning to cook, or relearning from maybe when they were kids and delving up some of those memories. What we’re looking toward is establishing not only consistent housing for the client but also, a consistent lifestyle that fits in with that housing.—Staff (Caregiving)
While caregivers did receive some formal training as part of the pilot program, most staff felt that additional specialized training would be highly beneficial to caregivers engaged in the pilot. Suggested topics for such trainings included understanding houselessness, trauma-informed care, crisis intervention and de-escalation techniques, and harm reduction strategies. One housing staff described the need, I think it would probably be beneficial to have some sort of an introduction to supportive housing and introduction to homelessness and the process of how they’ve [the clients] gotten to where they’re at. Maybe some understanding of trauma-informed care. I haven’t experienced it with [the pilot program], but caregivers in the past not understanding the idea of housing someone prior to solving all their other problems.—Staff (Housing)
Payment structures and policies present challenges for job satisfaction and retention among current caregivers. While caregivers in the pilot program were compensated at a higher wage than other caregivers, their work is challenging and emotionally demanding. To help reduce burnout, staff interviewees noted that both housing and caregiving supervisors strive to offer pilot caregivers flexibility in taking time off and working to ensure that caregivers feel supported, validated in their frustrations and concerns, and aided in problem solving.
I’ve talked to multiple caregivers in the program about it is that mental health issues are huge with our caregivers and they can get burnt out. Our union has great mental health programs, and I’ve referred two of them to those. I don’t know if they’ve tapped into. One of them did not, they chose not to but I think I’ve talked to a lot of them about how have you thought about going back to regular home care because it is a hard environment to work in and you are emotionally invested and when you don’t have success. They have lots of success, but when you don’t have success, it can be disheartening for some of them.—Staff (Caregiving)
Caregiving and housing supervisors described efforts to be readily accessible and facilitating clear channels of communication with other housing staff around role expectations. Even so, staff also identified times when it was challenging to determine whether housing staff or caregiving staff should support a specific client need. As one staff member explained, I think caregivers knowing to say no is okay. Not only to the client, though, but to the staff because you walk into a room and sometimes it’s a hoarder room . . . why isn’t it okay for caregiver to say, “Hey, no” and when a staff member is like, “Hey, can you help blah and blah with their room?”—Staff (Caregiving)
Discussion
The evaluation of this pilot program provided an opportunity to explore the value of integrating personal care services into housing settings from the perspective of clients as well as housing and caregiving staff. Interviews with these groups highlight the positive impact that caregivers had on clients while also emphasizing the need for additional infrastructure to support this workforce.
Altogether, interviews revealed that having caregiving services available in housing settings removed barriers to accessing personal care supports and alleviated anxiety for clients reacclimating to housing. The caregivers in the pilot provided key instrumental supports for things like transportation, connection to health care services, and medication adherence which are frequently cited as unmet needs among recently housed populations.19,20 The assistance with the daily living activities provided by caregivers, in turn, contributed to clients’ overall sense of health and well-being, and highlights the benefit of making this type of assistance more available in housing settings. As older adults both constitute a growing proportion of people with experiences of homelessness and have unmet needs in terms of achieving ADLs and IADLs,6,13 these results suggest that the integration of caregivers into housing settings may fill an important gap in services.
Findings from this evaluation also suggest that working with the pilot caregivers helped many clients re-learn to trust other care providers, which helped clients to feel safe, supported, and not alone in facing their needs. Previous evaluation work has identified the importance of going beyond basic needs by working to rebuild emotional ties that can facilitate the re-integration process for people with experiences of homelessness. 21 Overcoming the social isolation and marginalization experienced during periods of homelessness requires focused effort, and programs like the pilot assessed here may offer promising strategies for promoting connectedness among people with experiences of homelessness.22,23
The consistency of the caregivers' presence at the housing site and their genuine care and concern for clients' needs played an important role in clients feeling comfortable developing relationships with caregivers at their own pace. This enabled clients to view caregivers as a reliable source of support. In this way, caregivers act as a bridge supporting the client in a process of stabilization. A mixed methods evaluation of a similar personal caregiving pilot program in Washington state found that participation positively contributed to successful transitions into housing. 16 Similarly, prior research has shown that housing environments that employ flexible and respectful approaches to care, take time to build trust and personal relationships, and engage clients in meaningful ways contribute positively to housing stability.24,25 Moreover, social support, like the support provided by the caregivers in the pilot, has been identified as a key contributor to well-being above and beyond housing instability for individuals who have experienced periods of homelessness. 26
Finally, interviews with pilot staff revealed both the essential role of the caregivers in the success of the pilot program along with the ongoing challenges of recruiting, training, and retaining this important workforce. Maintaining a robust paraprofessional workforce, like personal caregivers, is a systemic issue with high rates of turnover and persistent understaffing across care settings.12,27 While many paraprofessionals find their work rewarding, challenges such as low pay, lack of benefits, heavy workloads, unsafe working conditions, inadequate training, and limited opportunities for advancement contribute to high rates of burnout and turnover in this workforce.12,28 Findings from this research also have potential implications for extending the use of theoretical frameworks like the occupational stress model 29 into alternative settings such as the homeless crises response systems and may also underscore the usefulness of these models as guides for informing future programmatic efforts.
While the staffing challenges identified by interviewees are not unique to the pilot program, staff identified several opportunities to better equip caregivers to work in these types of housing environments. Offering a well-developed training program could help to hone the skills of the caregiver workforce as well as reduce potential risk of injury.30,31 Alongside training, increased wages and benefits could also help to improve recruitment and retention. 12 Additionally, continuing to cultivate workplace environments that elevate and center the perspective of caregivers in the design and implementation of these types of programs would serve to ensure caregivers are recognized as key members of the staff. Together these strategies would serve to grow and maintain a more robust caregiving as well as ensure the provision of high-quality personal care. 12
Limitations
Study findings are limited by several factors. The interview guide was not pilot tested with the study participants prior to data collection. In addition, staff interviewees may not capture the full range of perspectives for all staff engaged in the pilot program, especially caregivers as we did not achieve data saturation among this group of staff. Similarly, client interviewees consisted of a small convenience sample of individuals engaged in the pilot program at 3 of the 5 pilot sites. The results presented here may not fully represent the experiences of clients at other sites in the pilot. Moreover, we relied on housing staff to help identity and recruit eligible clients. Staff selection may have been biased toward clients they work with most frequently or toward clients who have had a good experience in the pilot and thus, again, limits the study’s ability to speak to the diversity of experiences. There is also potential for social desirability bias in clients’ responses around the services they receive from caregivers, especially because all clients were still receiving personal care services. The use of an external evaluation team to conduct interviews may have helped to mitigate this bias. Finally, because many of the factors shaping the program may be unique to the United States context (e.g., Medicaid funding restrictions) it may be difficult to extrapolate the findings of this work to other counties especially in diverse settings with distinct culture and socioeconomic contexts. Even so, this work highlights the importance of care work in supporting the reintegration of individuals with experience of homelessness as well as a call to action to recognize the essentialness of care work in promoting human well-being.
Conclusion
Interviews with clients and staff implementing the caregiving pilot program demonstrate how the expansion of personal care services into the homeless crises response system helps clients establish more stability in their day-to-day lives, and positively contributes to their physical health, mental well-being, and housing stability. Even so, the demand for caregiving services outpaced the pilot’s ability to onboard new staff. Strategies aimed at increasing economic incentives, improving training processes, as well as highlighting the key role of caregivers among staff teams may help to address concerns around caregiver recruitment and retention.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank the Southwest Washington Accountable Community of Health for funding this work. We would also like to acknowledge the support and insight from the program staff at Council for the Homeless and the Vancouver Housing Authority, as well as thank the housing supervisor staff for their help connecting us with potential interviewees. Finally, we would like to thank the research staff who helped with this study including Jennifer Rountree for their project support.
Author Contributions
The author contributions were as follows: All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Katherine Marsi, and Sarah Roth. The first draft of the manuscript was written by Katherine Marsi and Sarah Roth and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Southwest Washington Accountable Community of Health.
Ethics Statement
The protocol for this study was approved by the Providence Institutional Review Board (IRB #2021000402). Participants provided verbal informed consent prior to enrollment in the study.