
Abstract
Workforce shortage and the increasing burden of rheumatic and musculoskeletal diseases lead to extreme time constraints in rheumatology outpatient care. Digital services promise to facilitate care by relieving employees and unleash new capacities. This study aims to explore the perspectives of early adopter health care professionals (HCP) on digital transformation in outpatient rheumatology. In-depth qualitative interviews were conducted with rheumatology nurses and physicians in 3 German rheumatology outpatient clinics, each characterized by an advanced level of digital adaption. Qualitative data were subsequently analyzed using deductive-inductive qualitative content analysis. Interviews with 11 rheumatology nurses and 5 rheumatologists were completed. Three key themes emerged from the qualitative analysis: (i) Digital transformation of care; (ii) impact of digital transformation on health care delivery; and (iii) perceived drivers of successful digitalization. The interviews revealed that digital technologies are widely used throughout the complete patient pathway. Digitalization enables more continuity and flexibility in rheumatology care. Patient information can be electronically obtained in a standardized manner prior to planned visits, enabling an informed consultation and more time for in-depth patient discussion. Although digitalization restructures work, it can also increase the current workload. Improved accessibility for patient calls leads to more work for HCP. Important drivers of successful digital technology implementation are low-threshold and interoperable services, a medical team that is interested and educated in eHealth, and comprehensive patient information and onboarding. Digital transformation is increasingly redefining rheumatology care. While accelerating communication and workflows, improved service accessibility leads to more work for HCP.
Keywords
The growing need for rheumatology care faces a shortage of specialized professionals. eHealth is one of the solutions for ensuring adequate rheumatological care in the future, especially in the outpatient sector. Despite advancements, there is a lack of insights into HCPs’ views on digital transformation in outpatient rheumatology and the factors influencing it.
There is still a lack of organisational research on the successful implementation of digital health. Our study is the first to investigate the digitalization dynamics in rheumatology outpatient clinics.
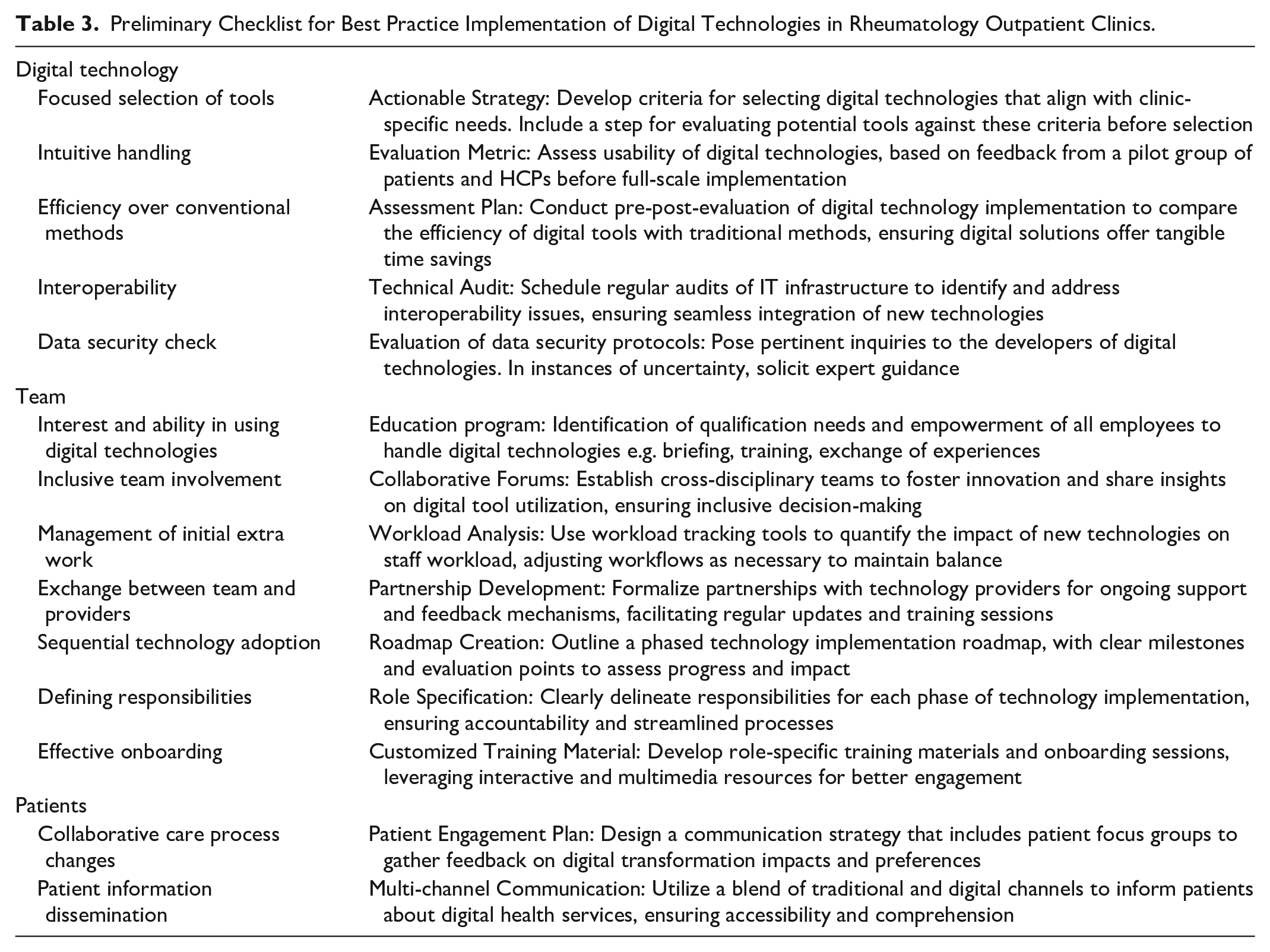
Implementation of digital technology requires focused tool selection, intuitive usage, speed improvement over conventional methods, interoperability, and data security. Teams need interest and training in digital technologies, inclusive involvement and structured responsibilities. Patient collaboration involves clear communication about care changes, addressing concerns, and using multiple media for information dissemination.
Introduction
The number of people suffering from rheumatoid and musculoskeletal diseases (RMDs) is increasing. 1 Concurrently, there are not enough specialized health care professionals (HCP) available to address the high demand for rheumatology care. 2 A recent systematic review shows an increase in the prevalence of inflammatory rheumatic diseases in Germany, with an estimated prevalence of IRD in Germany to be 2.2%-3.0%, which corresponds to approximately 1.5 to 2.1 million affected individuals. 3 In contrast, as of 2021, Germany had a total of 682 rheumatologists available in outpatient care, resulting in a ratio of fewer than one rheumatologist per 100,000 adults. This figure falls significantly short of the minimum threshold needed for adequate care, which is estimated at 1350 per 100,000 adults. The German Society of Rheumatology suggests that to ensure sufficient medical care, the ideal ratio should be approximately 2100 per 100,000 adults. 4
eHealth represents a viable solution to relieve the strained state of rheumatology care.5,6 Particularly in outpatient care, eHealth approaches could contribute to enabling close follow-up while saving human resources.7,8 Digital services, such as telehealth,9,10 mHealth,11,12 specifically digital health applications (DiGA) 13 or app-based ePRO monitoring, 8 and wearables 14 are valuable measures that can support classic therapeutic options. 15 Furthermore, assistive digital systems like voice assistants, 16 systems for obtaining medical anamnesis, 17 and questionnaire-based need-driven appointment management 18 support organizational processes in medical practices, which in turn might be connected in relieving rheumatology workforce 6 (Figure 1).

eHealth in rheumatology care.
The potential of eHealth has been recognized at both the national health policy level and in the professional associations in Germany: In 2019, the Digital Health Act was passed with the goal of additionally boosting digital transformation in healthcare. 19 In 2020, the German Society of Rheumatology (DGRh) launched their position paper of the commission on digital rheumatology of the German Society of Rheumatology. 20 In addition, eHealth received further impetus from Covid-19 and the urge to reduce infections through less face-to-face contact2 -23 that also resulted in European recommendations for remote care in rheumatology. 24 Despite advancements, the perspectives of healthcare professionals (HCPs) on digital transformation and its effects within rheumatology outpatient clinics remain largely unexplored. Moreover, understanding the organizational and structural factors driving digitalization in these settings is still an area in need of research, both nationally and internationally. Particularly, HCPs in clinics that have already embraced a high level of digital adaptation are well-positioned to provide insights on this matter.
Our study aims to explore the perspectives of early-adopter HCPs regarding digital transformation in outpatient rheumatology care, focusing on nurses and physicians within this specialty. Specifically, we aim to address the following questions:
How do HCPs experience digital transformation in the context of outpatient rheumatology care?
What are HCPs’ perceptions of digitalization’s impact on the delivery of outpatient rheumatology care and their work routines?
Which drivers of digitalization are identifiable within outpatient rheumatology practices?
Method
To explore the early adopters’ experiences of digital transformation in outpatient rheumatology care, we conducted qualitative interviews with rheumatology nurses and physicians. The study commenced with the identification of rheumatology outpatient clinics throughout Germany, noted for their high level of digital adaption, through a literature review that encompassed journal articles and conference presentations of the last 5 years. Clinics located in the northern (Immunologikum Hamburg, Rheumatologie and Klinische Immunologie, Hamburg), central (Rheumatologische Schwerpunktpraxis, Osnabrück), and southern parts (MVZ für Rheumatologie Dr. Martin Welcker GmbH, Planegg) of Germany were chosen for their participation. The principal investigator (FM), who is an experienced researcher in the field of digital rheumatology, contacted the directors of the outpatient clinics and invited them to participate in the study. The directors provided their consents to support the study. Interview participants were selected using homogeneous sampling to permit a logical generalization and comparability between the 3 rheumatology outpatient clinics. 25 The inclusion criterion comprised (1) employment as a HCP in a rheumatology outpatient clinic; (2) using digital services or assistive systems on a daily basis for more than 3 months; (3) willingness to participate in an interview. Candidates not meeting these specifications were excluded from participation. Since the present study is focused on a very homogeneous study population and the objectives are narrowly defined, the sample size was set a priori at a minimum of 15 participants. We chose to conduct 15 interviews as this number has proven to be adequate in previous studies to reach theoretical saturation in the exploration of digital approaches.8,26 The participants were financially compensated for their participation in the study and received a sum of €50 by bank transfer after the interview was completed. Semi structured interviews were conducted by 2 experienced health services researchers (SM, FM) using an open-ended interview guide that was developed to elicit rheumatology nurses’ and physicians’ perspectives on digital transformation in rheumatology outpatient clinics. A preliminary interview guide was drafted by a multiprofessional team including the following domains: Rheumatology, Psychology and Public Health. To ensure relevance and clarity of the questions, we conducted a pilot test of the interview guide with 4 participants from rheumatology outpatient clinics. The pilot interviews were not included in the analysis. After the pilot phase the interview guide was refined. For instance, questions that were misunderstood were eliminated and groups of questions were rearranged to maintain the flow of the conversation. The final interview guide included the following 3 main topics:
Utilization of digital health services and assistive systems in rheumatology outpatient clinics
Changes in outpatient rheumatology and in general health care delivery
Drivers for successful implementation of digital services in rheumatology outpatient clinics
Additional sociodemographic data was collected, including gender, age, profession and professional experience (for detailed information please see Supplemental Material 1). Prior to commencing the interviews, the 2 interviewers underwent training in a preparatory workshop. To minimize the risk of infection of Covid-19, the interviews were carried out by telephone. All study participants received a study information pack and provided their written informed consent prior to voluntary participation. Data collection was continued until the target number of 15 interviews was achieved. Consistent with the planned number of interviews, no substantial new findings emerged and saturation of content was reached. 27 The interviews were audio-recorded and transcribed verbatim. Qualitative analysis of the interviews was performed iteratively by SM, FM and KB based on Kuckartz’s structured qualitative content analysis 28 using MAXQDA software (Verbi GmbH). In the course of data cleaning, only the statements that referred to the interviewer’s initial questions were taken into account. Text passages that did not refer directly to the questions were not included in the coding process. Relevant text passages were coded, organized, deepened and systematized by using MAXQDA. The analysis began with a screening and familiarization with the interview data, where upon the interview texts were coded (SM, FM, KB). Main categories and subcategories were formed from the codes. Until a common understanding of all the emerging categories was achieved, consensus discussions were held continuously in the research group. Categories were developed based on the research questions and merged into a coding tree. At this stage, data collection had already been completed. Two experienced researchers (SM, FM) independently applied the developed category system to the entire data to ensure traceability. For the presentation of the results, representative quotes of the transcripts were selected, translated forward-backward into English by KB, proficient in both languages, and included into the manuscript, while long quotes were visually set off from the main text.
Results
Participant Characteristics
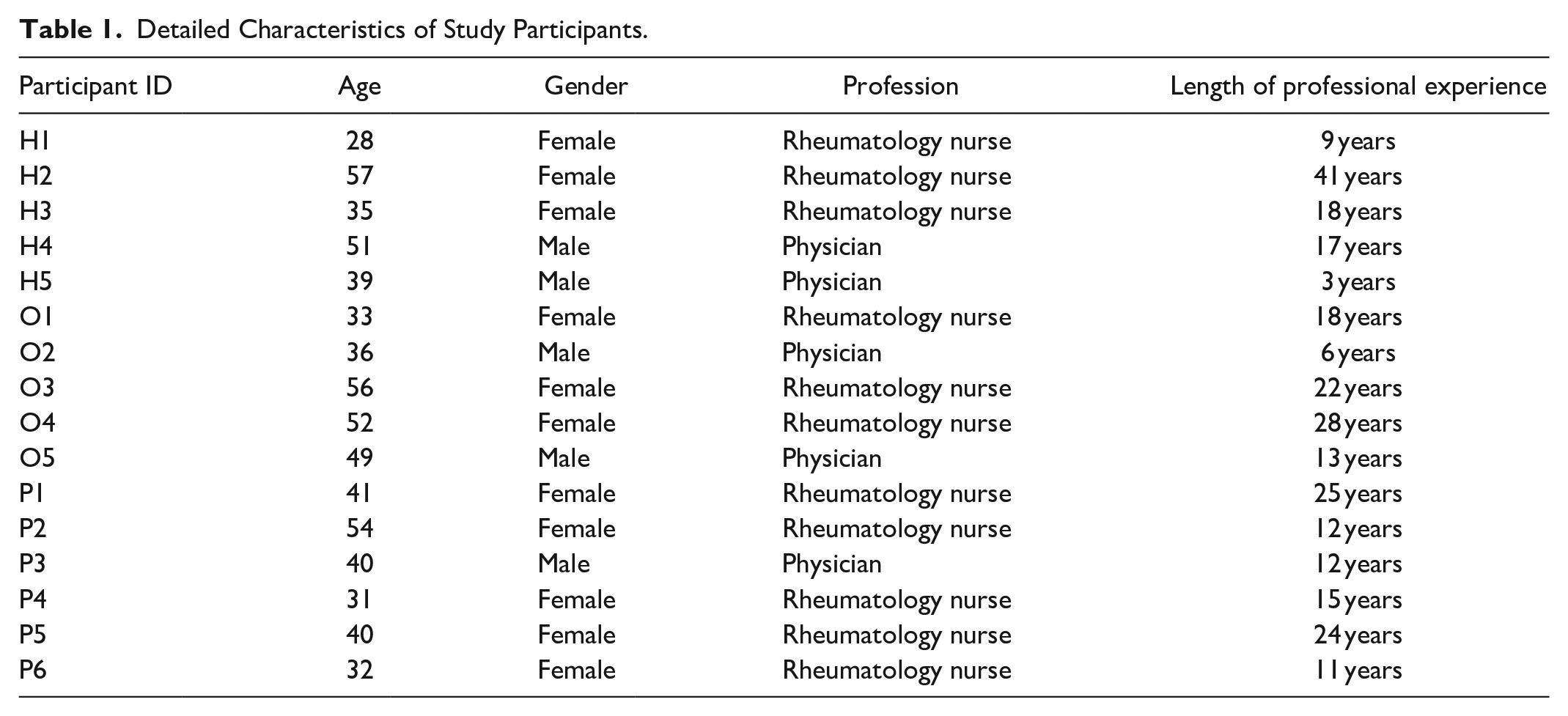
In January and February 2022, we conducted qualitative interviews with 11 rheumatology nurses and 5 rheumatologists, see Table 1. Mean age of interviewed nurses and physicians was 40 (range: 28-57) and 43 (range: 36-51) years, respectively. All of the interviewed rheumatology nurses were female (11/11; 100%) and all physicians were male (5/5; 100%). Interviews lasted an average of 46 (39-55) minutes.
Detailed Characteristics of Study Participants.
Themes
The analysis followed 3 key themes: (i) Digital transformation of care; (ii) impact of digital transformation on health care delivery; and (iii) perceived drivers of successful digitalization.
Digital Transformation of Care
The interviews revealed that digital technologies are widely used in all stages of outpatient rheumatology care from scheduling the doctor’s appointment to follow-up care. Figure 2 illustrates which digital services and assistive systems are currently used in rheumatology outpatient clinics and in which stage rheumatology care they are utilized.

Digital health services and assistive systems utilized in rheumatology outpatient clinics per stage of the care process.
The perspectives of the interview partners were relatively homogeneous, revealing no discernible differences between rheumatologists and nurses in their evaluations of digital technology. However, variations emerged in the application of digital technologies, with nurses primarily utilizing these tools for administrative purposes, whereas doctors employed them for both patient care and administrative tasks.
Impact of Digital Transformation on Health Care Delivery
Impact of Digitalization on Outpatient Rheumatology Care Delivery
HCP reported that automated voice assistants (i.e., PraxisConcierge/https://praxisconcierge.de/) support appointment scheduling, as they ensure better accessibility and lead to optimized management through appointment reminders.
So, what’s going well is the reachability. We are virtually not NOT reachable, we are always reachable. We are just sometimes not personally available, it's sometimes only the automated voice assistant who can be reached. [H4-Physician; Position: 18-18]
Participants reported that communication within the team, but also with patients, has accelerated due to digital transformation of the clinic organization. In addition, less patient-relevant information is lost through the use of digital technologies. For example, all requests are noted by the automatic voice assistants. The person responsible for answering the request must then check the documentation software whether the individual request has been processed. This procedure ensures that no important information is lost.
Digitalization certainly leads to the fact that we save paper and also telephone calls, without any loss of information. [O2_Physician; Position: 46-46]
Participants reported that digital technologies facilitate efficient work. Efforts in everyday work are minimized and time can be saved. With the use of systems to assess the medical history (e.g., idana/https://idana.com/), for example, patient-relevant information can be compiled concisely and recorded quickly. Tasks can be prioritized as their relevance can be assessed better and faster. Last but not least, data can be accessed quickly and independently of the workplace, allowing new working models to be implemented.
There’s a lot, a lot of resources wasted in day-to-day practice with what I’ll call information displacement. What bothers me most is that the patient walks in the door and we don’t really have any information about him at that point. We don’t know, whether he is only coming for a blood sample, whether he just wants to get a prescription, whether he has an appointment, with whom he has an appointment, how is he at the moment, how has he been in the last few weeks? This is all banal information that can be collected prior to the appointment. The flow of information within the clinic, between the patient and the clinic, before the appointment, these are all things that certainly could have a huge increase in efficiency or potential to save time, to then be able to focus on the core task of being a doctor again, and of course reinvest that time in the patient. [O2_Physician; Position: 32-32]
Consultations can be better prepared as patient-relevant information is available to physicians before the patient enters the consultation. Physicians report that they have more time with patients through the use of digital tools (such as idana) because information that they would otherwise have asked for during the consultation are already available. This allows a more focused and patient-oriented consultation.
And it is important to note that it is a more valid data pool and basis for a therapy decision if you actually have the patient describe or write it. And then you also have to work with it. And this work is much more pleasant. We have more time for discussion during visits and we don’t have to spend so much time on data collection. [H4-Physician; Position: 34-34]
Long-term, digital tools can reduce the physician's documentation effort and lead to faster preparation of medical reports.
At the same time, the participants report challenges that occur with the implementation of digital technologies. Digital services and assistive systems have to comply with data protection regulations, whose inspection is connected to additional work. In addition, organization of the data entering the system also requires work.
Furthermore, additional documentation is required during the initial implementation phase.
Situations where no action can be taken, for example, in the event of a system failure, are described as elusive.
Impact of Digitalization on Work Routines in Rheumatology Outpatient Clinics
HCP reported that the use of digital technologies has changed the way they communicate in their daily practice. Where the telephone was previously used, patients communicate more frequently via email.
Yes, it has changed completely. We also have a lot of patients with whom we often only communicate by e-mail, because they are difficult to reach by phone, either at work or because they are away on business or have appointments. [P4_Rheumatology nurse; Position: 66-66]
According to the HCP the use of digital technologies relieves or reduces the workload of rheumatology nurses in certain areas of activity.
And yes, of course, digitalization of fax-machines and e-mail or expansion of e-mail communication has simply led to us saving manpower and time, especially at the rheumatology nurse, medical assistant level. [O2_Physician; Position: 30-30]
However, the HCP state that digitalization shifts the daily routines of rheumatology nurses. For example, calls are no longer answered directly but via an automated phone assistant and can thus be answered by the rheumatology nurse at any time. Consequently, the workload becomes more structured, but according to the HCP, it is not decreasing.
On the other hand, you also feel that it’s extra work because, of course, a lot of requests weren’t even made to us in the past, because they [the patients] didn’t reach us. And now all [patients] reach us. And all the requests have to be processed. That’s why I think it’s a more structured extra work. [H4-Physician; Position: 28-28]
Due to the extra effort involved in introducing new digital services and systems, participants report that this is initially associated with an increased experience of stress.
Yes, I mean everything that is new means more stress in the short term. First of all, you have an increased stress level. Not because you have the feeling that you’ll get it right, but rather, does it all work? Do the processes work, do the interfaces work, and so on? [P3_Physician; Position: 72-72]
Digitalization might have an impact on patient physician communication. By gathering patient-relevant information before a visit via app or digital questionnaires (e.g., idana or Rhadar-RhePort/https://www.rheport.de/), there is more time for other topics in the consultation, which has an impact on care from the participants’ point of view.
If everything is recorded beforehand in this app or in the questionnaires, then the patients can simply discuss other things with us again. I think this gives us a little more time for personal exchange. If something is happening somewhere else or there is something on the patient’s mind that simply can’t be captured digitally in an app. [P1_Rheumatology nurse; Position: 46-46]
In addition, digitalization allows new working models and flexibility in rheumatology outpatient clinics. For example, it is possible for rheumatology nurses to work remote or from home.
I work a lot in home office [. . .]. And that's also a big point of digitalization. You have to try to organize rheumatology care in such a way that it can be done from several places. That creates so much flexibility. [O1_Rheumatology nurse; Position: 30-36]
Perceived Drivers of Successful Digitalization
The interviews with rheumatology nurses and physicians revealed specific drivers of digitalization in outpatient rheumatology care (Table 2).
Coding Tree: Requirements at Different Levels.

HCP described the principle “the simpler, the better” as a prerequisite for the successful implementation of digital technologies into medical practice. If the handling is simple and intuitive, there is a high probability that technologies will be used in everyday practice. The digital tools must be faster than the previous, conventional approach. Ideally, each technology is compatible with the practice software, allowing data to be easily transferred. Digital technologies have to be pre-tested and examined before implementation. Not all technologies may be suitable for all practices. Additional data protection examination should also be performed before implementing new digital tools.
Digital transformation of rheumatology outpatient clinics requires technical skills and even more importantly interest in the adoption of digital technologies. It is essential that not only the physicians, but also the rheumatology nurses are involved in the implementation process. According to the HCP, implementation periods succeed when team hierarchies are flat. Each implementation involves additional work for the team until the technology becomes routine. To support this process of routinization, technologies have to be implemented successively by defining sub goals and tracking achievements, and not in an ad hoc approach. For instance, only a predefined group of HCP should start using a new technology, with the rest of the team joining at a later date. It is particularly important that responsibilities are pre-defined at the beginning of the implementation.
Patients need to be informed about the new technologies in the medical practice. This also includes purpose, advantages and possible risks and problems with technology use as well as a short introduction to the correct way to use the specific technology.
Discussion
In this qualitative study, we explored the perspectives of early-adopter HCPs regarding digital transformation in outpatient rheumatology care, focusing on nurses and physicians within this specialty. We found that eHealth is increasingly implemented in all phases of outpatient rheumatology care in the investigated clinics. According to the study participants, digitalization impacts rheumatology care primarily by accelerating communication with patients and appointment management. It promotes efficient workflows in the rheumatology outpatient clinics and allows access to crucial patient information in the medical consultation. Yet, HCP also describe challenges of digitalization in rheumatology care, which lay mainly in the implementation of new technologies, technology failure and data protection. The drivers for digitalization in outpatient rheumatology operate at different levels: on the part of the technologies themselves, on the part of the rheumatology care team, and on the part of the patients. Drawing from the insights of our qualitative analysis, we have developed a preliminary checklist aimed at guiding the best practice implementation of digital technologies in rheumatology outpatient settings (Table 3). This checklist aligns with established implementation frameworks, such as the Consolidated Framework for Implementation Research (CFIR). 29 Nonetheless, its applicability and refinement require further validation through empirical studies leveraging real-world data to ensure its efficacy and relevance in practical scenarios.
Preliminary Checklist for Best Practice Implementation of Digital Technologies in Rheumatology Outpatient Clinics.
Our results are in line with earlier research in rheumatology care and beyond: The interview data from the 3 clinics confirms that digital transformation actually contributes to effective allocation of scarce resources in outpatient rheumatology.4,30 The use of voice assistants can improve the accessibility of clinics. 30 Digitalization can contribute to the attractiveness of rheumatology as a profession through new working models in the outpatient clinics, flexibility, but also a high appreciation of the nurses when it comes to the use of technologies.4,30 At the same time, our results show that digitalization tends to structure workloads, without reducing it. The imbalance between increasing patient demand 1 and stagnating workforce 2 remains, which is why our results may dampen hopes for relief of the strained situation in rheumatology.4,6
Our qualitative results also align with the findings of Richter et al., 23 who found that the use of video consultations in rheumatology stagnated again after a brief peak following the outbreak of the Covid-19 pandemic. The participants of our study mentioned the use of video consultations only marginally. Apparently, they are not (anymore) part of rheumatology care delivery in the 3 clinics. Concurrently, our findings suggest that digitally-supported asynchronous and telemedicine-based outpatient follow-up concepts, as reported by De Thurah et al., 7 are not yet part of the standard care in the 3 clinics. This observation extends to digital educational interventions, currently being explored in the management of fibromyalgia care. 31 Lack of incentives in the medical reimbursement system could be key barriers. 8
As reported in previous quantitative studies,32,33 the participants emphasized the relevance of intrinsic motivation of HCP to try digital approaches as an important driver. In fact, the high level of digitization in the 3 clinics studied can be attributed to the high motivation of the directors and HCP. This also applies to patient education: Informing and training patients are time-intensive tasks and requirements to successfully implement technologies into outpatient care routines. However, with advancing digital transformation of healthcare delivery, we find that patient education in eHealth should not be the task of the medical clinics. For instance, in psychiatry care a curriculum for training digital navigators to support community-based digital literacy for patients and clinical-based integration for HCP has been established.34,35 Furthermore, developers can also contribute to the digital transformation by developing their technologies narrowly to the working routines in rheumatology outpatient clinics: Their services must fit easily and seamlessly into established workflows and existing IT. 36 Our study is the first to investigate the drivers of digitalization in rheumatology outpatient clinics. We closely aligned with the reality of care and the perspective of users/the user perspective. Organizational research on the successful implementation of digital health is still largely unexplored. Findings highlight the potential of digital technologies to make rheumatology care and healthcare as a whole more personalized and efficient, particularly in enhancing access to care. The study underscores the necessity for specialized digital technology training tailored to the unique roles of nurses and doctors. 32 For nurses, who primarily use digital tools for administrative tasks, and doctors, who leverage them for both patient care and administrative functions, such training can enhance job efficiency and satisfaction—both key aspects to counteract workforce shortage in rheumatology.1 -4
We highly agree with Frisinger and Panagiotis on “the importance of listening to the voice of healthcare is valuable for understanding the conditions that need to be fulfilled when adopting new technology into a healthcare organization.” 37
From a methodological perspective, our research is consistent with Lincoln and Guba’s 4-dimension criteria to assess rigor of qualitative research. 38 To ensure credibility, factors such as the researcher’s genuine interest in the subject area, long engagement with the topic, immersion in the data and interviewing a wide range of people contributed to credibility. To ensure dependability, the authors discussed the coding and analyses throughout the research process and reached agreement on the final coding tree and themes, which enabled both data credibility and reliability. To enhance confirmability, the researcher consulted with several qualitative researchers and made a concerted effort to provide a comprehensive description of the study methodology. To increase transferability, a semi-structured interview guide was used and described in detail, which is also transferable to similar populations. In addition, a sufficiently detailed description of a phenomenon makes it possible to assess the extent to which the conclusions drawn are transferable to other times, settings, situations, and people.
However, limitations underlie our insights: Only HCP from 3 rheumatology outpatient clinics were included in this study using homogenous sampling. Simultaneously, the potential for selection bias is notably high. Additionally, there is a high potential of a bias towards social desirability, given that participants were aware their clinics had been recognized as early adopters. Moreover, pre-existing acquaintanceships between the principal investigator and the clinic directors might have influenced responses, leading to answers tailored to what participants presumed would align with the principal investigator’s interests. To mitigate these biases, researchers formulated neutral questions and actively encouraged respondents to articulate both positive and negative experiences. In this research, only perspectives by rheumatology nurses and rheumatologists were inquired. These might not be applied to other professional groups. In addition, patients were not interviewed at this time. Furthermore, our findings only apply to outpatient care. It is unclear whether the identified drivers of digitalization can also be transferred to inpatient rheumatology care.
These limitations directly translate into opportunities for further research: We are planning to extend the study to the inpatient setting of rheumatology care. Since hospitals are larger organizational units, we expect to observe other drivers of digital transformation here. Further, patients’ perspectives on ongoing digital transformation need to be continuously assessed. In addition, our qualitative results should be validated by quantitative data and our checklist for the successful implementation of digital technologies in rheumatology outpatient clinics needs to be critically appraised, extended and, most importantly, tested in practice. Furthermore, it is crucial to investigate to what extent digitalization affects the quality of rheumatology care, health care spending and whether it reduces diagnostic delay. 39
Conclusion
Digital transformation is advancing in outpatient rheumatology care, making eHealth ubiquitous from the perspectives of HCP. According to HCP it impacts rheumatology care by accelerating communication and workflows, while enabling access to patient information. Yet, workloads in rheumatology outpatient clinics may be accelerated and structured through digitalization, but not reduced.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241247021 – Supplemental material for “The Simpler, the Better.” A Qualitative Study on Digital Health Transformation in Early Adopter Rheumatology Outpatient Clinics
Supplemental material, sj-docx-1-inq-10.1177_00469580241247021 for “The Simpler, the Better.” A Qualitative Study on Digital Health Transformation in Early Adopter Rheumatology Outpatient Clinics by Susann May, Robert Darkow, Johannes Knitza, Katharina Boy, Julian Schwarz, Martin Heinze, Johannes Hornig, Peer Aries, Martin Welcker and Felix Muehlensiepen in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author’s Note
Johannes Knitza is also affiliated to Institute for Digital Medicine, University Hospital of Giessen and Marburg, Philipps University Marburg, Marburg, Germany.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was conducted in cooperation with RheumaDatenRhePort GbR (RHADAR) and uses data from a health care analysis commissioned by AbbVie Deutschland GmbH & Co. KG. This publication was funded by the Brandenburg Medical School Open Access Publication Fund supported by the German Research Association.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.