
Abstract
Regular exercise and community engagement may slow the rate of function loss for people with dementia. However, the evidence is uncertain regarding the cost-effectiveness and social return on investment (SROI) of home exercise with community referral for people with dementia. This study aimed to compare the social value generated from the in-person PrAISED program delivered before March 2020 with a blended PrAISED program delivered after March 2020. SROI methodology compared in-person and blended delivery formats of a home exercise program. Stakeholders were identified, a logic model was developed, outcomes were evidenced and valued, costs were calculated, and SROI ratios were estimated. Five relevant and material outcomes were identified: 3 outcomes for patient participants (fear of falling, health-related quality of life, and social connection); 1 outcome for carer participants (carer strain), and 1 outcome for the National Health Service (NHS) (health service resource use). Data were collected at baseline and at 12-month follow-up. The in-person PrAISED program generated SROI ratios ranging from £0.58 to £2.33 for every £1 invested. In-person PrAISED patient participants gained social value from improved health-related quality of life, social connection, and less fear of falling. In-person PrAISED carer participants acquired social value from less carer strain. The NHS gained benefit from less health care service resource use. However, the blended PrAISED program generated lower SROI ratios ranging from a negative ratio to £0.08:£1. Compared with the blended program, the PrAISED in-person program generated higher SROI ratios for people with early dementia. An in-person PrAISED intervention with community referral is likely to provide better value for money than a blended one with limited community referral, despite the greater costs of the former.
Promoting regular exercise and engaging in community activities may slow the rate of functional loss for people with dementia. However, the cost-effectiveness of exercise programs for people with dementia is conflicting.
The in-person PrAISED program generated higher social value ratios than blended delivery. Patient participants gained social value from improved health-related quality of life, social connection, and less fear of falling. Carer participants acquired social value from less carer strain. The NHS gained benefit from less health care service resource use.
In-person delivery of home exercise with community referral for people with early dementia is likely to provide better value for money than a blended delivery with limited community referral.
Introduction
Dementia is a complex and progressive syndrome causing cognitive impairment and restricted daily function.1,2 It affects the mental, physical and financial wellbeing of people living with dementia and their families. 1 In 2019, the global cost of dementia was $1.3 trillion and is expected to rise to $1.7 trillion by 2030. 2
Preventing or delaying the onset of dementia by 2 years can have significant economic and societal benefits. 3 For people with dementia, the ability to perform daily activities deteriorates as the disease progresses. 4 For people with dementia and their carers, maintaining independence is a priority. 5 Promoting regular exercise and engaging in community activities may slow the rate of functional loss.6 -8 However, the cost-effectiveness of professionally supervised regular exercise for people with dementia is conflicting. One study indicated that a structured exercise program over 12 months was not able to maintain cognitive function for people with dementia, and therefore was not cost-effective. 9 Another study found that exercise therapy for people with dementia was not cost-effective in terms of quality-adjusted life year (QALY) gains, but potentially cost-effective when improvements in behavioral and psychological symptoms were considered. 10 A home-based exercise program for people with dementia in Finland reported reductions in hospital admissions and overall costs 6 and another study demonstrated that 10 home-based sessions of community occupational therapy for people with dementia and their carers could be cost-effective. 11
PrAISED (promoting activity, independence, and stability in early dementia) was a multi-center, pragmatic, randomized controlled trial (RCT), which was conducted between October 2018 and September 2022.12,13 Patient participants were recruited from 5 locations in England and were randomized to a control group (usual care) or an intervention group (PrAISED). The intervention was a specifically designed rehabilitation program that provided a home-based exercise program along with promoting access to community activities for people with early dementia.14,15 It was a complex intervention consisting of balance and strength building exercises, dual-task and functional activities training, and gait re-education. The PrAISED program included home visits from a multidisciplinary team (MDT) of physiotherapists (PTs), occupational therapists (OTs) and rehabilitation support workers (RSWs) who encouraged patients to engage in 180 min of physical activity per week. Patient participants in the PrAISED group were offered up to 50 therapy sessions over 12 months while those in the usual care group received an assessment modeled on usual falls prevention care which consisted of an initial visit and up to 2 further visits. 12
From October 2018 to February 2020, 61 patient participants completed the in-person PrAISED program prior to the COVID-19 pandemic. Due to pandemic restrictions between March 2020 and September 2022, 144 patient participants completed a blended PrAISED program which consisted of a combination of in-person visits, telephone calls, and video conferencing with MDT members. For blended program patient participants, referral to and uptake of community activities was significantly reduced due to pandemic restrictions.
Providing a home-based exercise program for people with dementia is a complex intervention. Recent guidelines from the Medical Research Council (MRC) suggest using a broad framework for economic evaluation to capture wide and diverse outcomes for complex interventions. In addition to cost-effectiveness analysis (CEA), the MRC recommends cost-consequence analysis (CCA), and cost-benefit analysis (CBA). 16 Social return on investment (SROI), a type of social CBA, is becoming more commonly used to evaluate complex interventions.16,17 SROI quantifies and values multiple outcomes to achieve a broader perspective than traditional CEA, which tends to focus on only 1 outcome (ie, QALY).18,19 SROI is a pragmatic form of social CBA, which is recommended in His Majesty’s (HM) Treasury Green Book in the United Kingdom (UK) to assess interventions that impact social welfare.17,20 The framework for SROI is described in the Cabinet Office “A Guide to Social Return on Investment.” 21 SROI identifies and quantifies outcomes that are relevant to stakeholders and then determines financial proxies for these outcomes, which often do not have market values. This enables SROI ratios to be presented in monetary units (£). SROI adopts an individual approach to measuring the social value of outcomes rather than averaging across an entire intervention arm.18,22 SROI can help inform decision-making by monetizing and reporting the social value generated by a health or social care intervention.
There are few published SROI studies of interventions to improve the health and wellbeing of people with dementia. Previous studies include the impact of peer support groups, 23 art activities, 24 and home exercise and community referral. 25 Our study intended to build upon the PrAISED feasibility study (n = 60) of home exercise and community referral for people with early dementia. 25 The findings of this study indicated that the PrAISED intervention could generate positive SROI ratios ranging from £3.46 to £5.94 for every £1 invested. 25 We hypothesized that the main trial PrAISED intervention (n = 365) would generate similar ratios. However, the impact of the COVID-19 pandemic rendered it impossible to conduct the PrAISED program in-person, necessitating a change in the mode of delivery. Therefore, the objective of this SROI analysis is to compare the social value generated from the in-person PrAISED program delivered before March 2020 with a blended PrAISED program delivered after March 2020.
Methods
The study design for the PrAISED multi-center RCT has been previously reported, covering details such as the randomization method, sample size calculation, participant selection criteria, informed consent, and content of baseline and follow-up questionnaires. 12
A CONSORT flow diagram outlining the flow of participants through the trial is shown in Figure 1. A CONSORT checklist reporting on the trial design, analysis and interpretation is presented in Supplemental File 1. 26

Adapted CONSORT 2010 flow diagram outlining the flow of participants through the trial.
In this evaluation, a range of SROI ratios were generated using quantitative data collected during the PrAISED trial. SROI methodology contains the following steps: identifying stakeholders, developing a logic model, evidencing outcomes, valuing outcomes, calculating costs, and estimating the SROI ratio. This analysis was conducted in alignment with the 21-item SROI Quality Assessment Framework Tool 27 (Supplemental File 2).
Key stakeholders were the people and organizations most affected by the PrAISED program: patient participants, informal carer participants and the National Health Service (NHS). It was expected that patient participants would benefit from home exercise and community referral; carer participants would benefit from additional support provided by MDT home visits, and the NHS would benefit from less frequent health service use from PrAISED patient participants.
Comparing the In-Person and Blended Programmes
Patient participants in the in-person and blended PrAISED program were offered up to 50 therapy sessions over 12 months. PrAISED was designed as an individually tailored in-person program comprising of physical exercises, functional activities, and inclusion in community life. However, following the guidance on strict social distancing and remaining at home during the COVID-19 pandemic, PrAISED in-person visits were discontinued after 17 March 2020. Therefore, a blended PrAISED program was delivered which included telephone calls, videoconferencing and in-person visits when possible.
Logic Model
The logic model of the PrAISED intervention illustrates how the intervention intended to improve quality of life, lessen fear of falling, increase social connection, reduce carer strain and decrease health service resource use (Figure 2).

Logic model of the PrAISED intervention.
Outcomes
Five relevant and material outcomes were identified from the logic model: improved health-related quality of life, increased social connection, less fear of falling, decreased carer strain, and reduced health service resource use. Four of these outcomes were measured and valued using baseline and follow-up questionnaires: fear of falling (Falls Efficacy Scale-International; FES-I), 28 health-related quality of life (EQ5D-5L), 29 carer strain (Carer Strain Index; CSI), 30 and health service resource use (adapted Client Service Receipt Inventory (CSRI) 31 (Table 1). Social connection was measured and valued using an adapted community activities questionnaire (CAQ) at follow-up (Supplemental File 5). Three of the outcome measures FES-I, EQ5D-5L, and CSI were validated scales frequently used in studies involving persons with dementia.
Quantity of Relevant Outcomes Measures for In-person and Blended programs.
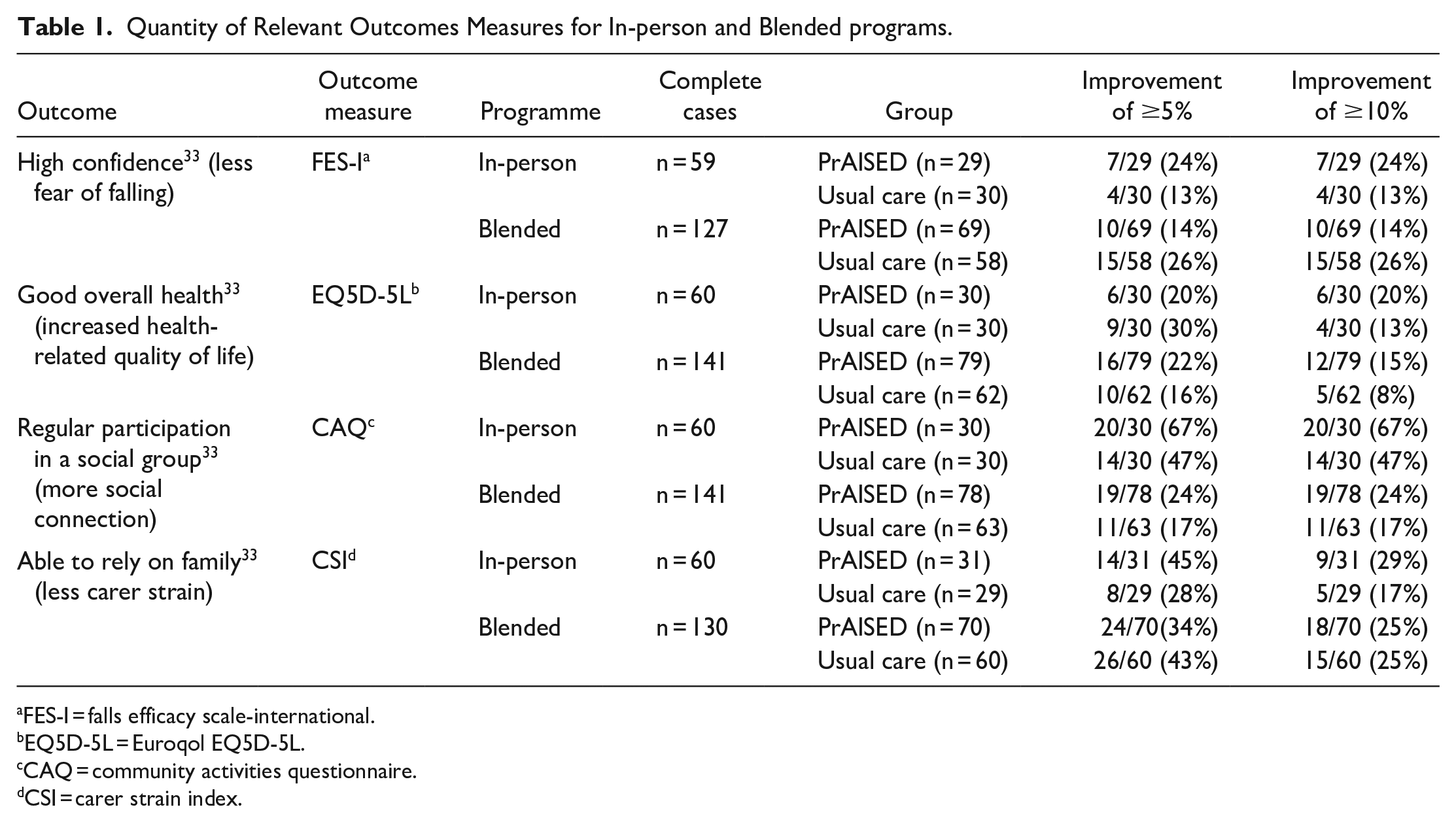
FES-I = falls efficacy scale-international.
EQ5D-5L = Euroqol EQ5D-5L.
CAQ = community activities questionnaire.
CSI = carer strain index.
FES-I measured whether home exercise could generate more confidence in patient participants performing activities of daily living and therefore reduce the risk of falls. Health-related quality of life as measured by the EQ5D is recommended by the National Institute for Health and Care Excellence (NICE) for conducting economic evaluations of complex public health interventions. 32 The CAQ measured the degree to which patients increased their engagement in community activities due to the PrAISED intervention. For carer participants, the CSI was a key outcome measure, assessing whether PrAISED lessened the burden of care on family members or carers. Finally, the CSRI form measured whether PrAISED resulted in reduced healthcare service use by patient participants in comparison with usual care (Table 1).
For 4 outcomes (FES-I, EQ5D-5L, CAQ, and CSI), financial proxies were assigned from the Social Value Bank (SVB). The SVB is a databank of methodologically consistent unit costs for outcome indicators. 33 It is based on “wellbeing valuation” and recommended in the HM Treasury Green Book as a robust method for financial appraisal and evaluation. 22 Monetized values from the SVB included £13 080 for high confidence (less fear of falling); £20 141 for good overall health (health-related quality of life); £1850 for regular attendance at a social group (social connection); and £6784 for being able to rely on family (less carer strain). 33 For 3 outcomes (FES-I, EQ5D-5L, and CSI), financial proxies were assigned using 2 cut-off points for participants who improved by ≥5% and by ≥10%. These 2 cut-off points allowed for calculation of a range of SROI ratios, enabling a sensitivity analysis. For CAQ, a financial proxy was assigned for those participants who participated in community activities at least once a month. 33
Health Service Resource Use
Outcomes for the NHS were assessed by measuring the health service resource use of patient participants during the previous 3 months before the baseline and 12-month follow-up. Cost data were obtained from NHS unit costs and Personal Social Services Research Unit 2020/202134,35 (Supplemental File 4). Health service resource use included contact with general practitioners (GPs), nurses, physiotherapists and other hospital services (Supplemental File 4). Health service resource use analysis compared PrAISED with usual care patient participants for both in-person and blended delivery formats.
Training and Delivery Costs
Total costs for the PrAISED intervention included the following categories: MDT training costs, MDT staffing and transport costs, instructional materials, and exercise equipment for patient participants. Total costs per patient participant were calculated for both in-person and blended formats.
SROI Ratios
After outcomes and costs were monetized, SROI ratios were calculated by dividing the social value per participant by the cost per participant. Intervention participants were compared with usual care participants for both the in-person and blended formats. In most SROI evaluations, deadweight, attribution, displacement, and drop-off are considered. 18 However, our study design was an RCT, and therefore it was unnecessary to calculate these factors. Discounting was also unnecessary because all costs and outcomes were measured within 12-months of the baseline assessment.
Results
Of the 365 trial participants, 75 (21%) did not provide 12-month follow-up outcome data and an additional 85 (23%) did not provide cost data. Complete cost data (at both baseline and follow-up) was obtained from 205 (56%) participants. Of these, 61 (30%) participants completed the in-person program, and 144 (70%) participants completed a blended program. For blended PrAISED participants, approximately 69% of sessions were received in-person and 31% were experienced by telephone or videoconference.
Baseline characteristics were similar between in-person and blended patient participants. The mean age was 81 and 79 years for in-person and blended programs, respectively. Most patient participants in both programs were male, married, and white ethnic (Supplemental File 2).
In-Person Programme
SROI results for the in-person program showed that when compared with usual care, a higher proportion of in-person PrAISED patient participants reported improvements of ≥5% in fear of falling and social connection, and in-person PrAISED carer participants reported improvements of ≥5% in carer strain (Table 1). Social value was also higher for in-person PrAISED patient and carer participants when compared with usual care at both the 5% and 10% cut-off points (Table 2).
Valuing Outcomes for In-person and Blended program.

Blended Programme
SROI results for the blended program indicated that when compared with usual care, a lower proportion of blended PrAISED patient participants reported improvements of ≥5% in fear of falling and a lower proportion of blended PrAISED carer participants reported improvements of ≥5% in carer strain (Table 1). Social value was also lower for blended PrAISED patient participants and only slightly higher for blended PrAISED carer participants when compared with usual care at both the 5% and 10% cut-off points (Table 2).
Training and Delivery Costs
The NHS was responsible for training and delivery costs of the 12-month PrAISED program. Overall, 61 therapists were trained to deliver the PrAISED program to 183 patient participants. In-person training costs averaged £184 per patient participant compared to £139 per patient participant for online training (Supplemental File 3).
The difference in delivery costs between PrAISED and usual care was £1504 per participant for the in-person program (Supplemental File 3), and £1105 per participant for the blended program. Total costs for the in-person program were higher than blended program by £444 per participant (Supplemental File 3).
Health Service Resource Use
For the in-person program, health service resource use was £11.71 less per PrAISED patient participant in comparison with usual care, mostly due to PrAISED patient participants reporting a 20% reduction in outpatient visits during the 12-month intervention (Supplemental File 4). For the blended program, health service resource use was £23.36 more per PrAISED patient participant in comparison with usual care, partly due to an 8% increase in outpatient visits by PrAISED patient participants during the 12-month intervention (Supplemental File 4).
SROI Ratios
SROI ratios comparing the in-person program with usual care ranged from £0.58:£1 to £2.33:£1. In contrast, SROI ratios for the blended program ranged from a negative ratio to £0.08:£1 (Table 3).
SROI Ratios.

Discussion
PrAISED was designed as an in-person exercise rehabilitation program delivered in the homes of people with early dementia. Due to lockdown and social distancing restrictions during the COVID-19 pandemic, the intervention had to be adapted to a blended program. A substantial difference was found in SROI ratios between the pre-pandemic in-person delivery and the blended delivery during the pandemic. The in-person program SROI ratios ranged from £0.58 to £2.33 for every £1 invested, while the SROI ratios for the blended program ranged from a negative ratio to £0.08: £1.
In-Person Programme
The range of SROI ratios for the in-person PrAISED program was lower than the SROI ratios from the in-person PrAISED feasibility trial, which ranged from £3.46 to £5.94 for every £1 invested. 25 Possible explanations for differences in results include variations in the population recruited, expertise of the clinicians delivering the program, the small sample sizes, and different thresholds for assigning social values.
The variation in the population recruited refers to a higher proportion of feasibility study participants enrolling from the Join Dementia Research (JDR) service. These participants tended to have higher motivation and engaged more fully with the PrAISED program which resulted in higher outcomes. The feasibility trial had a higher proportion of MDT members who were therapists within NHS Mental Health Services for Older People (MHSOP). These therapists had more training and experience in working with people with dementia, which may have also led to higher outcomes.
Differences in SROI ratios between the feasibility study and our study may have also been due to using different thresholds for assigning social value. In the feasibility trial, SVB financial proxies were assigned to participants who either “stayed the same” or “improved” between baseline and follow-up. However, one of the main principles in social value accounting is to “only include what is material” and social value guidance states that “materiality is essentially a matter of professional judgment.” 36
Blended Programme
The lower SROI ratios for the blended program may have been due to restrictions on the in-person delivery during the pandemic, and the inability to refer patients to community activities. During the pandemic, community activities became unavailable or unattractive to older people with early dementia who may have considered themselves at high risk of COVID-19. Regular engagement with community groups is significantly associated with slower cognitive decline for people with dementia and lower risk of developing dementia.8,37 Telephone and video conference delivery made it more difficult for the MDT to develop therapeutic relationships with participants and to help participants advance toward goals that required their physical presence. 38 Patient participants often engaged more deeply with PrAISED exercises when MDT members were physically present.38,39 Patients reported that in-person therapy visits were experienced as an opportunity for meaningful human interaction. The social element of in-person visits were an important factor for achieving positive outcomes. 39 These results are consistent with a recent study which found that in-person interventions for people with dementia may be more effective than internet-based interventions for reducing anxiety and improving activities of daily living. 40
Comparison With Other Studies
Previous research on the cost-effectiveness of in-person supervised exercise for people with dementia is uncertain. A 2008 study (n = 135) found that 10 home-based sessions of community occupational therapy for people with dementia and their carers could be cost-effective. 11 However, a 2019 study (n = 494) found that a structured exercise program over 12 months was ineffective in maintaining cognitive function for people with dementia and thus was not cost-effective. 9 Our study indicated that an in-person home-based exercise program coupled with access to community activities for people with early dementia could generate positive SROI ratios.
Strengths of This Study
To our knowledge, this SROI evaluation is the first study to compare the social value of in-person versus blended delivery of a home-based exercise program to people with dementia. The RCT design helped ensure that social value was not overestimated, and the societal perspective using multiple outcomes helped ensure that important benefits were not overlooked. In addition, the majority of outcomes were based on quantitative data collected from both patient and carer participants at baseline and follow-up. Finally, the social value sets used in this study were derived from wellbeing valuation, a robust method recommended for measuring and valuing social CBA. 20
Limitations of This Study
The main limitations were due to the COVID-19 pandemic, which could not have been anticipated. The sample sizes for the in-person and blended participants were unplanned and unequal. It was not possible to determine to what degree the change in the mode of delivery or the change in the social context during the pandemic explained the differences in SROI ratios between the in-person and blended phases.
Another limitation is that the SVB is limited to the UK context and does not have monetary proxies for every possible material outcome. Monetized values in this study were applied for outcomes closely associated with specific SVB values. 33 However, matching study outcomes with specific SVB values depends on researcher discretion, which could lead to potential bias in overestimating or underestimating social value. Furthermore, the generalizability of these findings is uncertain as future studies may use different outcome measures and monetary proxies. Nevertheless, the SROI results captured multiple outcomes of a complex intervention. These outcomes were relevant to stakeholders and presented in monetary units to inform decision-making.
Conclusion
Compared with blended delivery, the PrAISED in-person exercise program generated higher SROI ratios for people with early dementia. During the COVID-19 pandemic, a blended delivery of the exercise program and the curtailment of community activities may explain why there was a negative SROI ratio during this period. These findings suggest that in-person delivery with community referral is likely to provide better value for money than a blended delivery with limited community referral, despite the greater costs of the former. The findings also illustrate how the social context in which the intervention was implemented could significantly impact the value for money. However, future research should continue to explore the impact of lower- cost blended approaches for improving activities of daily living for people with dementia.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241246468 – Supplemental material for RCT-based Social Return on Investment (SROI) of a Home Exercise Program for People With Early Dementia Comparing In-Person and Blended Delivery Before and During the COVID-19 Pandemic
Supplemental material, sj-docx-1-inq-10.1177_00469580241246468 for RCT-based Social Return on Investment (SROI) of a Home Exercise Program for People With Early Dementia Comparing In-Person and Blended Delivery Before and During the COVID-19 Pandemic by Kodchawan Doungsong, Ned Hartfiel, John Gladman, Rowan Harwood and Rhiannon Tudor Edwards in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580241246468 – Supplemental material for RCT-based Social Return on Investment (SROI) of a Home Exercise Program for People With Early Dementia Comparing In-Person and Blended Delivery Before and During the COVID-19 Pandemic
Supplemental material, sj-docx-2-inq-10.1177_00469580241246468 for RCT-based Social Return on Investment (SROI) of a Home Exercise Program for People With Early Dementia Comparing In-Person and Blended Delivery Before and During the COVID-19 Pandemic by Kodchawan Doungsong, Ned Hartfiel, John Gladman, Rowan Harwood and Rhiannon Tudor Edwards in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Thanks to Dr Catherine Lawrence for reading support for RTE.
Contributions of Authors
RH, JG and RTE developed the study concept, acquired funding and contributed to the study design. KD and NH analyzed the data and drafted the manuscript. All authors contributed to reading and approving the final draft. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the NIHR Program Grants for Applied Health Research, award number RP-PG-0614-20007. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Ethical Approval
This study was approved by the Bradford-Leeds Research Ethics Committee (REC number 18/YH/0059, IRAS project identification 236099) and research governance departments in each organization.
Patient and Public Involvement
Every stage of the research cycle included patient and public involvement to ensure that the intervention was relevant and the research processes were acceptable to people with mild dementia and their carers.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.