
Abstract
Intimate partner violence (IPV) is globally endemic and a gross violation of human rights, in addition to abuse of intimacy by some men against their female intimate partners. Based on literature review, attitudinal, socio-demographic, and experiential attributes of 15 to 49 year old ever partnered women in the heterosexual relationships were identified. This study used the anonymized 2020-21Cambodia Demographic and Health Survey (CDHS) data to compute the IPV prevalence and its correlates, in addition to computing the changes in IPV prevalence at the urban, rural, and at the national levels using data from the 2014 CDHS. Identified attitudinal, socio-demographic, and experiential attributes were used in the bivariate and multivariable analysis. Simple and multiple logistic regression models were used for computing the bivariate and multivariate associations with IPV; additionally, trend analysis was done to compute changes in IPV prevalence between the 2 surveys. Lifetime prevalence of IPV was 20.70%, while the most common subtype was emotional IPV at 18.70%. Ten out of 12 correlates studied were found to be statistically significantly associated with IPV in the bivariate analysis. These were added in the multivariable model and 7 were found to be statistically significantly associated with IPV. Which included educational attainment of women and their intimate partners, number of living children, women’s IPV acceptance, male partner’s alcohol use, knowledge of physical beating of mother by one’s father, and controlling behavior exercised by partner. During the intervening period between the 2 CDHSs, IPV and its subtypes were decreased in both urban and rural areas, as well as nationally. IPV decrease between the 2 DHSs and lower IPV rates in 2021-22 augur well for the health and human rights of Cambodian women. However, the ultimate target of eliminating IPV against women, will require measures that ensure economic and gender empowerment, and gender equality.
The prevalence and correlates of the intimate partner violence (IPV) in Cambodia are available only for the year 2014, using the 2014 Cambodia Demographic and Health Survey. While no trends analysis has been reported that determines statistical significance of IPV at either the national or urban/rural residency status.
The prevalence and correlates of the intimate partner violence (IPV) in Cambodia were computed using the most recent Cambodia Demographic and Health Survey conducted in 2021-22 and trend analysis for various types of IPV was done using the 2014 Cambodia Demographic and Health Survey.
Crafting optimal policy and practice response in combating intimate partner violence is contingent upon better understanding of the intimate partner violence burden and its correlates. Additionally, trend analysis disaggregated by the urban/rural residency status, has implications for better appreciation of stakes that drive IPV in Cambodia and globally.
Please mark ethical/consent statements from main document
In the subsection “Study area and data source” of the “Methods” section, following statement is highlighted/marked please:
“The ethical approval for the CDHS2021-22 was granted by the Cambodian National Institute of Statistics and the Ministry of Health, in addition to the ICF Institutional Review Board. While the approval for the conduct of secondary analysis of fully anonymized CDHS14 and CDHS 2021-22 surveys and spatial data was granted to the author by the Measure DHS using online request form.”
Introduction
Intimate partner violence (IPV) is a global public health and human rights concern that impacts a broad array of domains, including physical and mental health, economic security, and child welfare. IPV can be emotional, physical, and/or sexual in nature and is specified as “any behavior within an intimate relationship that causes physical, psychological, or sexual harm to those in the relationship.” 1 The United Nations Sustainable Development Goal (SDG) number 5 entails achieving gender equality and empowerment of all women; while goal 5.2 specifically refers to IPV and envisages to “Eliminate all forms of violence against all women and girls in the public and private spheres, including trafficking and sexual and other types of exploitation.” 2 The lofty SDGs were formulated by the United Nations General Assembly in 2015 and were called “Transforming our world: the 2030 Agenda for Sustainable Development” with most of the goals to be achieved by 2030. 3
However biased gender social norms are globally endemic today. The United Nations Development Program’s “Gender Social Norms Index” (GSNI) calculates various biases against women including “physical integrity”; which is a proxy for IPV. The 2023 GSNI report, based on data until 2022 shows that 85% of global denizens exhibit gender biases irrespective of regions, income levels and cultures. With 9 out of 10 people—men and women—hold biased opinions against women. While over a quarter deemed beating of wife by her husband as junstifiable. 4 Lifetime prevalence estimate in 2018, of physical and/or sexual IPV for ever-married/partnered women aged 15 to 49 in the WHO Western Pacific Region—which Cambodia is part of—is reported as 20%, in contrast with the global estimate of 27%. 5
The Demographic and Health Surveys (DHS) Program in collaboration with countries conducts DHSs to collect data on various population, health, and nutrition indices. These surveys have been conducted in over 90 countries, including Western Pacific countries. 6 DHS data have been extensively used to study IPV and its correlates. Several studies have identified age of women and her male intimate partner, urban/rural residency status, women, and her intimate partner’s educational attainment, women’s employment status, alcohol use and controlling behavior on the part of intimate partner, income status of the household, acceptance of IPV by women, participation in decision-making on important issues, and knowledge of one’s mother having ever been beaten by one’s father to be associated with IPV.7 -25 Consistent and strong associations between IPV and knowledge of one’s mother even having been beaten by father, alcohol use and controlling behavior demonstrated by intimate partner have been consistently associated with IPV in women. While the age of women and her intimate partner, urban/rural residency status, employment status of women, household wealth status, and acceptance of IPV by women have been shown to be lacking consistency. As reported associations are either bidirectional or having no associations with IPV. However, in general rural residency status, low educational attainment, low household wealth status have been associated with higher proportions of IPV in women.
Several recent meta analyses have also been done that echo these findings. A study based on 36 prospective/longitudinal studies reported unplanned pregnancy and low parental educational attainment (less than high school) as IPV risk factors, while being married and of older age as shielding against IPV. 26 Using data from 44 DHSs, a meta-analysis of 29 Sub-Saharan countries reported higher levels of low educational attainment in women being associated with higher IPV levels. 27 While higher prevalence of IPV was reported in infertile women in a meta-analysis using 25 studies from low- and middle-income countries. 28 Association of rural residency, poor living conditions, and women’s low educational attainment with IPV was reported by another meta-analysis based on DHSs conducted in 25 sub-Saharan African countries. 29
The Kingdom of Cambodia is a southeast Asian country with a population of about 16 million based on the “Cambodia Socio-Economic Survey 2019–20.” 30 There is a dearth of studies on IPV and its correlates from Cambodia. A recent study using DHS data from 7 countries including Cambodia for the years 2000, 2006, and 2014 provided results of IPV trend at the national level for physical and sexual IPV and reported increased sexual violence and decreasing physical violence in Cambodia 31 ; however, statistical significance was not computed. A study based on secondary analysis of United Nations Multi-Country Study on Men and Violence (UNMCS) and Nabilan Study databases, including Cambodia, reported the independent associations of alcohol drinking and lower gender-equitable attitudes with perpetration of IPV by men against women. 32 Another study from 4 countries, including Cambodia, analyzed the past-year prevalence of male-perpetrated IPV and its risk factors using the data from the United Nations Multi-Country Study on Men and Violence in Asia and the Pacific, underscored the importance of 4 correlates that included poverty, childhood trauma, male partner’s substance use, infidelity, and unemployment, in addition to women’s restricted control in relationship and her quarreling. 33
There have been 5 DHS surveys conducted in Cambodia that is, 2000, 2005, 2010, 2014, with 2021-22 being the most recent survey. For many countries, including Cambodia, DHSs are the only surveys that provide nationally and sub-nationally representative indices on IPV. The Cambodia DHS conducted in 2014 reported lifetime prevalence of IPV as a composite measure of emotional, physical, and/or sexual to be 28.7%. 6 In many developing countries, including Cambodia, the only nationally and sub-nationally representative metrics on IPV are provided by the Demographic and Health Surveys (DHS). This study aimed to address the current state of IPV in Cambodia, its structural and cultural contexts in which it occurs; based on secondary analysis of the fully anonymized most recent DHS cross-sectional and representative survey conducted in 2021-22. Additionally linear trend analysis of having ever experienced either emotional, physical, sexual, and the composite variable of all 3 types of IPV, was computed using the Cambodia 2021-22 DHS with the 2014 DHS.
Methods
Study Area and Data Source
Cambodia 2014 (CDHS2014) and 2021-22 (CDHS2021-22) Demographic and Health Surveys data were used for secondary analysis in this study. The data collection phase for CDHS2021-22 lasted from September 15, 2021, to February 15, 2022. Implementation of the CDHS2021-22 was jointly done by the Cambodian National Institute of Statistics and the Ministry of Health, with technical assistance provided by ICF though DHS program. The Cambodia 2019 General Population Census (GPC) was used as a sampling frame for CDHS2021-22. GPC entails list of all Cambodian enumeration areas (EA) that constitute as census counting units. Two-stage sample design was used for the CDHS2021-22 to compute estimates at the national, urban, rural, and the 25 provinces levels. First stage entailed selection of 709 EAs or clusters (241 urban and 468 rural), while the second stage entailed selection of 30 households using systematic sampling from each cluster; resulting in the selection of 21 270 households cumulatively. Women aged 15 to 49 years old who were either permanent residents or had stayed in the selected household, the night prior to survey, were deemed eligible for the survey using the woman’s questionnaire. The woman’s questionnaire also included the “domestic violence” module with questions on IPV. However, only 1 eligible woman in each household was randomly selected for the administration of domestic violence module, as per recommendation of the World Health Organization’s guidelines for the ethical collection of domestic violence including intimate partner violence information. 34 The domestic violence module was administered only after ensuring privacy, in the absence of which, this module was not administered.
Cumulatively, 7502 women were selected for the administration of domestic violence, but 158 women could not be interviewed due to either lack of privacy, frequent interview interruptions, or inability to find women despite several attempts. Hence, the total number of women who answered the domestic violence module questions was 7344.
Until recently DHS surveys collected information on IPV from ever-married women only, who were defined as “women who are currently married or living with a man as if married and women who were formerly married or lived with a man as if married.” Hence, women who were never-married but have or had intimate partners were not asked IPV questions. However, this restrictive inclusion criteria has recently been revised to gauge the true burden of IPV by also including never-married women who at the time of survey reported having an intimate partner or have had one in the past. The CDHS2014 used the old restrictive inclusion criterion, while the CDHS2021-22 used the expanded criterion. Hence, for the CDHS2021-22, “women who have ever had a husband or other intimate partner” were included. The total number of women who met this new eligibility criteria for questions pertaining to IPV in CDHS2021-22 were 6204, out of the 7344 who were selected and interviewed for the domestic violence module. While for the CDHS2014 there were 3498 women who answered the IPV questions based on the old restrictive eligibility criterion of having ever been married. Results in terms of the lifetime IPV prevalence and its correlates are provided based on the expanded eligibility criteria used for CDHS2-21-22.
The ethical approval for the CDHS2021-22 was granted by the Cambodian National Institute of Statistics and the Ministry of Health, in addition to the ICF Institutional Review Board. While the approval for the conduct of secondary analysis of fully anonymized CDHS14 and CDHS 2021-22 surveys data was granted to the author by the Measure DHS using online request form. As anonymized data for secondary analysis was used, no ethical approval was required. Additionally, author has no conflicts of interest.
Questionnaires for both surveys and details pertaining to methodology, sampling design & weights generation, including non-response adjustments are published in the Cambodia DHS reports available for free download on the Measure website. Anonymized datafiles for both surveys were downloaded from the Measure website www.measuredhs.com.
Study Variables
DHSs in Cambodia, as conducted in other countries, used the standardized domestic violence module based on the modified version of the Conflict Tactics Scale for questions pertaining to IPV. This scale has been empirically shown to have good validity and reliability in community and clinical settings.35,36 IPV is inquired about using several questions pertaining to emotional, physical, and sexual violence perpetrated by the male intimate partner. Computation of outcome and explanatory variables is described below.
Outcome variable
The composite dichotomous variable intimate partner violence (IPV) was computed as affirmative if the respondent reported having ever (lifetime) experienced any type of either emotional, physical, and/or sexual violence perpetrated by her male intimate partner. Emotional IPV was deemed positive if the respondent reported that her male intimate partner had either ever humiliated her, threatened to harm her, insulted her, or made her feel bad. Physical IPV was based on respondent’s affirmative responses to either having been ever pushed, shaken, thrown something at, slapped, arm twisted or hair pulled, punched with fist or something that could hurt, kicked, dragged, strangled, burned, or threated with a knife, gun, or any weapon by her male intimate partner. While sexual violence was computed as present if respondent had ever been either physically forced into unwanted sex, unwanted sexual acts, or to perform unwanted sexual acts. Questions pertaining to IPV were used from the “Conflict Tactics Scale.”
Explanatory variables
In this study 12 explanatory variables were used for computing association with IPV. These include women’s age, occupation, and educational attainment; her partner’s educational attainment and alcohol use; household’s wealth in terms of quantiles; urban/rural residential status; and number of living children. Women’s decision making ability in the milieu of intimate relationship was determined in terms of either her healthcare seeking, large household purchases, or visits to family or friends; affirmative answer to any of the 3 attributes in terms of decision being made either by the woman alone or jointly with her husband/partner were deemed as respondent being able to partake in decision making. Acceptance of IPV was considered acceptable if respondent gave affirmative reply to either wife beating justified if wife goes out without telling her husband, neglects children, argues with husband, refuses sex with husband, or burns food. Having knowledge of one’s father having ever beaten respondent’s mother. Finally, controlling behavior exhibited by intimate partner was deemed present if respondent gave affirmative answer to either her husband or intimate partner having ever gotten jealous or angry if she talked to other men, wrongly accused her of being unfaithful, doesn’t permit her to meet her female friends, tries to limit her contact with her family, or insists on knowing where she is all the times. With the exception of age of women and her intimate partner, wealth, and the number of living children, all other explanatory variables were coded as dichotomous (yes/no). Age was coded in 5-year intervals, occupation coded into 3 groups, number of living children into 4 groups, while wealth was coded in 5 groups (quantiles); category details for all variables are provided in the Table 1.
Counts and Proportions of Study Variables—Cambodia Demographic and Health Survey 2021-22.

Questions on “Husband/partner’s education” and questions pertaining to “Decision making” were asked from only those women who were either currently married or currently living with a male intimate partner.
For the CDHS2021-22, the intimate partner was defined as “[H]usband includes a partner with whom a woman is living as if married. Husband/intimate partner refers to the current husband for currently married women; the most recent husband for divorced, separated, or widowed women; the current intimate partner for never-married women who currently have an intimate partner; and the most recent intimate partner for never-married women who do not currently have an intimate partner but had one in the past.”
Data Analysis
STATA version 18 (Texas, USA) was used for the analysis, while accounting for complex survey design; hypothesis testing was 2-tailed with P-value of less than 5 deemed as statistically significant (P < .05). The 2 Cambodian DHS datasets were downloaded in STATA file format from the DHS website, upon approval of access request.
Unweighted counts along with number of missing records, weighted percentages reported as proportions were computed for all explanatory and outcome variables without imputing missing values. For each explanatory variable, binary simple logistic regression models were created to determine the association of binary outcome of the IPV variable. All statistically significant explanatory variables in the binary models were included in the final multiple logistic regression mode. Odds ratios along with their 95% confidence intervals and statistical significance were computed and reported. Lastly, linear trend analysis was conducted separately for the 3 types as well as cumulatively, for the IPV percentages at the national and based on urban/rural residency status between CDHS2014 and CDHS 2021-22 surveys. The 2 survey datafiles were appended, a new dichotomous variable “year” was created representing each survey and used as dependent variable with explanatory variable as IPV type in the logistic regression model.
Results
Cumulatively, 6204 women were asked questions about the intimate partner violence. Emotional IPV was reported by 1247 (18.70%) women, physical IPV was reported by 582 (8.73%), and sexual IPV was reported by 169 (2.61%) women. While 1372 (20.70%) women reported having ever experienced emotional, physical, and/or sexual IPV. Regarding prevalence of combinations of various IPV types: physical, sexual, and emotional IPV that is, all 3 types were reported by 100 (1.45%), physical and sexual IPV by 101 (1.48%), physical and emotional IPV by 485 (7.19%), and emotional and sexual IPV by 140 (2.11%) women. While 650 (9.85%) women reported physical and/or sexual IPV.
Table 1 displays findings in terms of unweighted number and weighted proportions expressed as percentages, for the IPV, its subtypes, and all 12 explanatory variables used in the analysis; number of missing records is also specified. The questions pertaining to “Husband/partner’s education” and “Decision making” were only asked from women who were either currently married or currently living with a partner currently married women, as such there were 564 women who did not answer this question. Lifetime prevalence of having ever experienced any 1 or more of the 3 types of IPV was 20.70% (95% CI: 19.25-22.23). Emotional IPV was the most common type of reported IPV (18.70%—95% CI: 17.36-20.11); followed by physical IPV (8.73%—95%CI: 7.73-9.84); while sexual IPV was the least common IPV (2.61%—95% CI: 2.11-3.22).
Each of the 3 types of IPV variables were composite indicators, hence within each IPV type, the most common emotional IPV was “ever being insulted or made to feel bad” by intimate partner (16.13%—95% CI: 14.85-17.51). Most commonly reported physical IPV was “ever been pushed, shook or had something thrown” by the intimate partner (6.33%—95% CI: 5.48-7.32). While for sexual IPV, the most commonly reported type was “ever been physically forced into unwanted sex” by the intimate partner (2.35—95% CI: 1.87-2.95).
Regarding the profile of respondents, about half of women (46.77%) were 35 or older; 42.52% had secondary or higher level of educational attainment, while half (50.06%) of their intimate partners also had similar educational attainment; 70.76% were engaged in some kind of work/job. Regarding the household wealth index, 64.14 women belonged to middle, richer, or richest group; 58.85% were living in rural areas; only 12.31% had no living children; participation in decision-making was reported by 95.35% women, while 59.27% believed that IPV was not justified or acceptable; overwhelming (82.39%) women reported use of alcohol by their intimate partner; only 14.82% reported knowing about their father having ever physically beaten their mother; finally, about a quarter (24.43%) reported controlling behavior exercised by their intimate partner.
Results of simple and multivariable logistic regression models, expressed as crude and adjusted odds ratios, their corresponding 95% confidence intervals, and statistical significance are shown in Table 2.
Crude Odds Ratios and Adjusted Odds Ratios for All Statistically Significant Associations Between Intimate Partner Violence and the Selected Variables – Cambodia Demographic and Health Survey 2021-22.
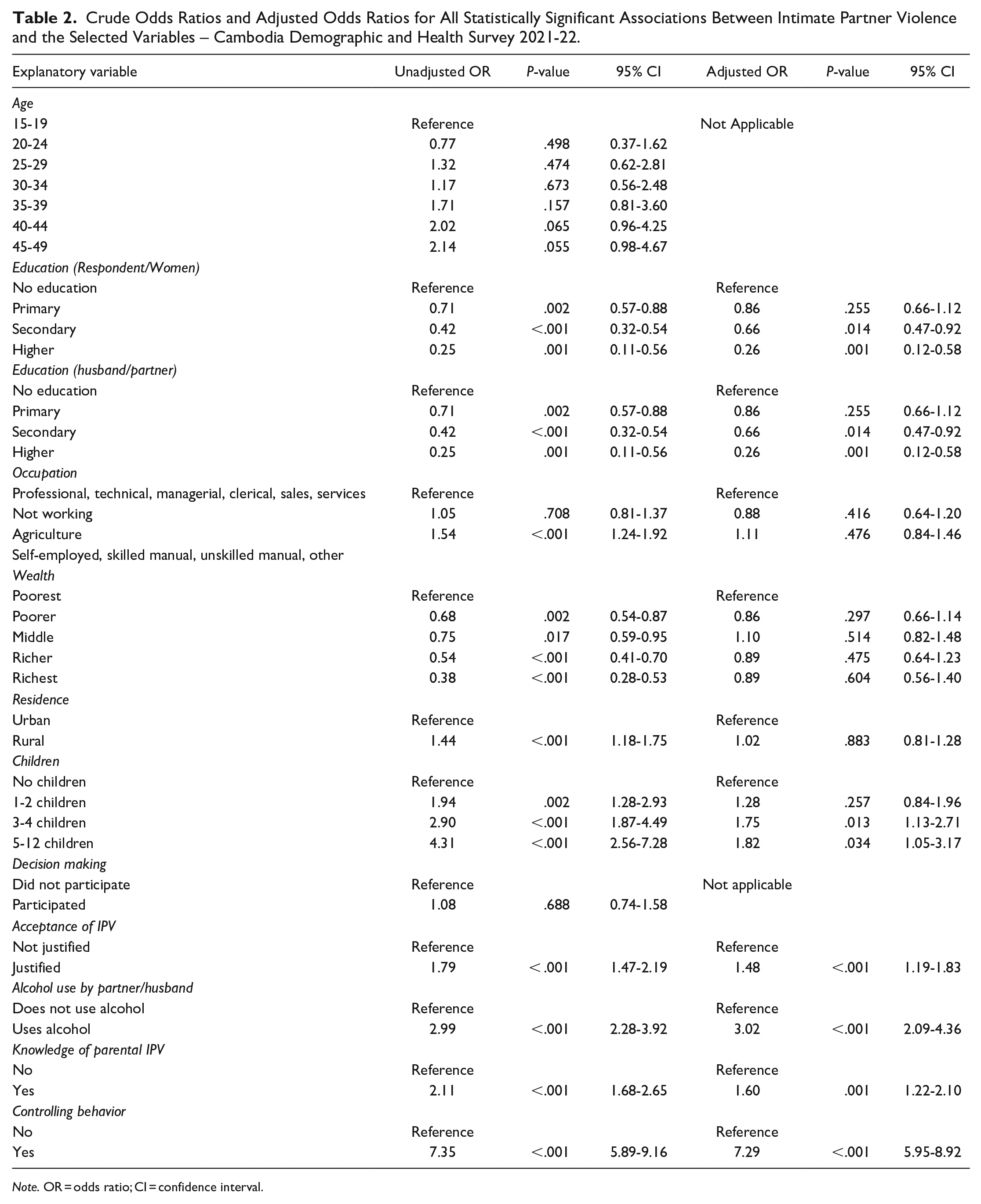
Note. OR = odds ratio; CI = confidence interval.
Twelve explanatory covariates were studied and based on the crude/unadjusted odds ratios and their statistical significance, only 2 explanatory variables that is, women’s age and her participation in decision-making were not statistically significantly associated with having ever experienced IPV. The remaining 10 covariates were added in the multivariable logistic regression model, which included women’s and her intimate partner’s educational attainment, wealth status, number of living children, women’s occupational status, acceptance of IPV, residential status (urban/rural), partner’s use of alcohol, knowing one’s father ever beat one’s mother, and controlling behavior displayed by intimate partner. In the final multivariable logistic regression model, save women’s occupational status, household wealth status, and residential status, all other 7 covariates were statistically significantly associated with having ever experienced IPV by women.
Results of the multivariable logistic regression model in Table 2 show that following statistically significant associations were found: compared with women with no education, those women who had either secondary (aOR: 0.66; 95% CI: 0.47-0.92) or higher (aOR: 0.26; 95% CI: 0.12-0.58) education were protected from IPV. Similarly, women whose intimate partners had secondary education (aOR: 0.57; 95% CI: 0.41-0.79) or higher (aOR:0.50; 95% CI: 0.25-0.97) were protected from IPV. Compared with women who had no living children, those who had 3 to 4 children (aOR: 1.75; 95% CI: 1.13-2.71) and those with 5 or more children (aOR: 1.82; 95% CI: 1.05-3.17) were more likely to have ever experienced IPV. Compared with women who believed that IPV was not justified or acceptable, those who did believe in IPV’s justification were more likely (aOR 1.48; 95% CI: 1.19-1.83) to report IPV. Compared with women, whose intimate partners did not use alcohol, those with alcohol using partners were more likely (aOR: 3.02; 95% CI: 2.09-4.36) to report IPV. Knowing about one’s mother having ever been beaten by one’s father was associated with higher (aOR: 1.60; 95% CI: 1.22-2.10) odds of having ever experienced IPV, compared with women who didn’t know. Finally, women whose intimate partners demonstrated controlling behavior were more likely (aOR: 7.29; 95% CI: 5.95-8.92) to report having ever experienced IPV compared to those whose intimate partner didn’t. The multivariable model focused on women who were either currently married or currently living with a male intimate partner. As questions about partner/husbands’ education and women’s decision-making involvement were only asked from women who were currently married/living with a man.
Results of linear trend analysis between the 2014 Cambodia DHS and the 2021-22 Cambodia DHS in terms of the 3 types and cumulative IPV prevalence between urban, rural, and at the national level are shown in Table 3. Statistically significant decreases were found in emotional IPV in rural areas as well as nationally; sexual IPV also decreased in a statistically significant manner in rural areas and at the national level. While for physical IPV, statistically significant decreases were found in all 3 levels that is, urban, rural, and national. Cumulative IPV that is, any IPV type ever experienced also decreased at the rural and national levels in a statistically significant manner.
Proportions and Trend Analyses of Emotional, Physical, Sexual, and Cumulative Intimate Partner Violence (IPV) by Urban/Rural Residency Status—Cambodia Demographic and Health Surveys (DHSs) 2014 and 2021-22.

Note. CI = confidence interval.
Discussion
Using data from the most recent representative cross-sectional Cambodia DHS (CDHS20-21), secondary analysis was conducted to study the lifetime prevalence of IPV and its correlates. Additionally, the changes and trends in the 3 IPV types as well as cumulative IPV prevalence were also computed using the CDHS2014. For ever partnered women aged 15 to 49 years in Cambodia, the lifetime prevalence of IPV was 20.70%. The prevalence of physical and/or sexual IPV was 9.85% in Cambodia, which is about half (20%) of what was reported for WHO’s Western Pacific Region, of which Cambodia is a member state. 5 While the global lifetime prevalence of physical and/or sexual IPV was reported as 27%. 5 Hence, Cambodia has much lower prevalence of physical and/or sexual IPV than in its neighbors, as well as compared to global estimates. Prevailing cultural norms and healthy attitudes entailing respect for women’s rights perhaps account for this divergence from the region and the world.
Amongst the 3 types of IPV, the least common type was sexual IPV (2.61%), while most common type was emotional IPV (18.70%); physical IPV was reported by 8.73% women. Some studies using DHS data have reported physical IPV as the most common among the 3 types.14,19,21 Perhaps men in some countries have the propensity to resort directly to physical IPV when dealing with their female intimate partners owing to real or imagined slights, threats, or attempting to keep her in her place. Or perhaps there is a continuum from emotional to physical IPV, and in some countries male intimate partners restrain themselves and do not escalate their emotional IPV to physical IPV. In any case, IPV is a behavioral phenomenon and can be unlearned. However, transition from primarily physical to primarily emotional IPV perpetrated by some men could be construed as an intermediate step before its elimination entirely. Preponderance of emotional IPV is by no means excusable, but an explanation is hypothesized for contrast with countries that report physical IPV as the most common type.
Survey respondents profile delineates about half of the women being 35 or older with slightly over 42% having secondary of higher education, and little over 70% having some job. Half of women reported their intimate partners educational attainment of at the secondary or higher levels. Household wealth was reported as belonging to middle, richer, or richest group by about 64% women. About 41% lived in the urban areas of the country, and almost 87% women had 1 or more living children.
Age of women and her participation in decision-making were the only 2 covariates out of the 12 examined, that were not statistically significantly associated with the IPV in the bivariate analysis. The lack of statistically significant association of participation in decision-making is understandable in the context of CDHS2021-22, as this attribute was reported by an overwhelming proportion (about 95%) of women. Since it was almost universal and as such lacked any discerning power to explain IPV. Lack of women’s age association with IPV has been reported previously.14,21 However, empirical evidence is also split, as association of both younger and older aged women and IPV has been reported.8,19,22,26
Out of the 10 covariates added to the multivariable model, 3 were not found to be statistically significantly associated with IPV, and included women’s occupation, household wealth quintile, and rural/urban residency status. Regarding women’s occupational status, other studies have also reported no association,14,21 unemployment being protective, 16 and women with high income or being employed as associated with higher probability of IPV.7,16 Higher wealth quintile/household wealth has been fairly consistently reported to be associated with lower probability of IPV,7,8,10,14,24 and conversely lower wealth quintiles with higher probability of IPV 17 ; however, absence of association with IPV has also been reported. 21 Perhaps wealth-driven empowerment of women and enlightened values in families with means, account for this association. Multivariable model may have negated the association of wealth with IPV when other variables present in the model are more pronounced in discerning associations with IPV. While for residency status in terms of urban/rural residency, rural resident women have been reported to be more likely to experience IPV,10,27 while rural residency’s association with low IPV has also been reported, 20 in addition to lack of association between residency status and IPV.14,21 The lack of association of IPV with women’s occupation, household wealth quintile, and rural/urban residency status in this study, against the backdrop of opposing associations previously reported, suggest the complex nature of IPV and its covariates and lends further credence to the notion that “all epidemiology is local.” 37 Hence, reinforcing the imperative need for reliable nationally representative data and indices for effective prevention of IPV in each country.
The 7 covariates in the multivariable model, that were found to be statistically significantly associated with IPV included educational attainment of women and their intimate partners, number of living children, acceptance of IPV by women, alcohol use by intimate partner, knowledge of physical IPV perpetrated by father on the mother and controlling behavior shown by the intimate partner. The covariates that have almost consistently been shown to be associated with higher probability of IPV include alcohol use by intimate partner,8,9,11,16,18,20 -22 knowing about one’s father having ever beaten mother,8,14 -16,19 -23,25 controlling behavior exercised by the male intimate partner,8,14,20,38 and acceptance/justification of IPV on the part of women.19 -21 However, acceptance/justification of IPV was not found to be statistically significantly associated with IPV, 14 while the same study reported lack of association between alcohol use by intimate partner and IPV. However, in this study the use of alcohol by intimate partner was reported by less than 2% of women. Inebriation owing to alcohol use is known to impair judgment including compromising inhibitions; knowing about one’s father having ever beaten mother is an experience that could be construed as a learned behavior and a putative pathway for women to normalize and misguidedly accept it as a normal/acceptable part of marital/intimate relationships. Acceptance/justification of IPV is also a learned behavior with its attendant acceptance, like one’s father having ever beaten one’s mother. While controlling behavior by one’s intimate partner could be explained as a harbinger of IPV. The conclusions drawn from the multivariable model apply solely to women who were either currently married or currently living with a male intimate partner. However the persistence of IPV’s association across several studies between aforementioned covariates does offer a glimmer of hope for the IPV’s eventual eradication globally; as IPV is a behavioral phenomenon and as such entirely amenable to prevention, in addition to promoting gender equality. However, no country is expected to completely eliminate and prevent IPV by 2030—an ambitious SDG goal—or for anytime in the foreseeable future, a practice as old as perhaps recorded history.
The association of higher levels of education in both women and her intimate partner with lower levels of IPV found in this study aligns with previous studies that reported lower educational attainment in women and her male intimate partner being associated with higher IPV levels in women; conversely association of higher educational attainment in both sexes and lower IPV reporting by women.7,14,16,18,19,21,22,27 Education renders respect for gender equality, that contributes to a better and more inclusive dynamic in an intimate relationship by refraining from violence and resorting to amicably resolving conflicts, whether real or imagined, by men.
Finally, the statistically significant association of IPV with having 3 or more living children found in this study has a fraught empirical evidence. Infertility has been reported to be associated with higher IPV, 28 no association between number of living children and IPV has also been reported, 14 but most studies report association of IPV and having children or having higher number of living children.10,16,20 -22 Perhaps having more children equates with additional financial and family care burden in general and could lead to potential stress in men as providers, that may serve as a conduit for IPV toward one’s intimate partner.
In addition to the physical and emotional pain experienced by the IPV victims, this practice also comes at the cost to the healthcare delivery systems; as IPV victims are reported to experience adverse mental health outcomes, and poor health outcomes in their newborns.39,40
The changing landscape of IPV in terms of findings from 2014 to 2021-22 using Cambodia DHSs revealed that IPV as a composite measure, as well as its 3 types, decreased across urban and rural areas of the country, in addition to nationally. This is definitely encouraging and promising, especially assuming that the current lower IPV trajectories will continue in future; but still a far cry from achieving SDG goals of gender equality and abolition of violence against women by 2030. IPV prevention interventions that leverage economic and gender empowerment, promote gender equality, and relationship skills building in both sexes, hold promise for eliminating IPV.
This study was based on cross-sectional survey data with its structural limitations: most importantly, study design obviates any casual determinations, as merely associations could be deciphered. Secondly, IPV was studied in the context of heterosexual relationships only, as such women who experience IPV perpetrated by a female intimate partner were not included; thus, potentially underestimating the true IPV burden experienced by women. Finally, owing to the study design the “reverse causality” or more specifically reverse associations could not be ruled out either. Perhaps women who justify/accept IPV might be the ones who have experienced IPV in the first place, using the same reasoning, IPV victims might be more likely to recall that their father ever beat their mother and so on. The inclusion criteria was also revised between the 2 surveys, as the CDHS2014 inquired about IPV from ever-married women only, while CDHS2021-22 also included women who were never married but have had been or were in intimate relationships with men. While the study’s strengths include the use of data emanating from the nationally representative survey conducted using standardized tools with rigorous and robust sampling and data collection methodologies.
Future avenues of research include determination of age at which certain toxic opinions including justification of IPV take root in women and conduct of longitudinal studies allowing for better casual inferences and antecedents of IPV. For better health and human rights in general in Cambodia, selecting prevention strategies that optimize neutralizing the pernicious correlates of IPV, offer the most opportune approach to mitigate and eventually eliminate the endemicity of IPV. Health education campaigns, entailing use of mass media, promoting gender equality, health, and human rights for women could help change country’s norms and mores on the status of women in Cambodia.
Conclusion
Intimate partner violence is globally rampant and Cambodia is no exception. Using the most recent representative survey data, emotional violence was found to be the most common type of IPV reported by women in intimate relationships. In the final multivariable model, women’s and her intimate partner’s educational attainment, number of living children, acceptance of IPV, partner’s use of alcohol, knowing one’s father ever beat one’s mother, and controlling behavior displayed by intimate partner were statistically significantly associated with IPV. Most of these correlates of IPV have been empirically demonstrated to be associated with IPV in several studies, auguring the need for better prevention and control strategies that harness the power of measures that promote economic and gender empowerment and gender equality. The changes from 2014 to 2021-22 show significant declines in all 3 types of IPV in urban and rural areas, as well as at the national level. However, meeting the SDG goals of eliminating violence against women and gender equality will be a marathon rather than a sprint in Cambodia.
Footnotes
Acknowledgements
The DHS Program is grateful acknowledged for granting access to the Cambodia 2014 and 2021-22 Demographic and Health surveys fully anonymized data.
Author Contribution Statements
N/A – Single author manuscript.
Data Availability Statement
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This manuscript is based on the fully anonymized data for the secondary analysis of Demographic and Health Surveys (DHS) conducted in Cambodia.
Grant Number
Not applicable.
Informed Consent/Patient Consent
This manuscript is based on the fully anonymized data for the secondary analysis of Demographic and Health Surveys (DHS) conducted in Cambodia. The ethical approval for the original Cambodia DHS 2021-22 was granted by the Cambodian National Institute of Statistics and the Ministry of Health, in addition to the ICF Institutional Review Board. Verbal consent was obtained from all the survey participants while the original survey was conducted.
Trial Registration Number/Date
Not applicable.