
Abstract
A good death is a human right. Unfortunately, patients with chronic heart failure (CHF) in the terminal stage still receive inappropriate life-sustaining treatment before death. There is limited understanding of the status of intensive care unit (ICU) admission, mechanical ventilation (MV), cardiopulmonary resuscitation (CPR), and even extracorporeal membrane oxygenation (ECMO) for patients with CHF before death, as well as their use of hospice-related services. This study investigated the trends and trend changes in intensive procedures and hospice-related services for patients with CHF in the last month of life. This population-based retrospective observational study included 25 375 patients with CHF from the National Health Insurance research database in Taiwan and collected information on their intensive treatments during the last month of life. We computed intensive treatment utilization rates and analyzed the trends and trend changes via joinpoint regression. The average percentage of patients with CHF admitted to ICUs was 53.27% (n = 13 516). A total of 327 (1.29%) patients with CHF received ECMO. The percentages of patients receiving MV (54.3%’41.5%) and CPR (41.5%’17%) decreased over time. Conversely, the percentage of ECMO use (0.52%’1.78%) increased. However, only 222 (0.87%) patients with CHF received hospice care in the last month of life between 2001 and 2013. The rates of ICU admission and life-sustaining treatment among patients with CHF in the month before death remain high, and hospice-related services remain inadequate. This study highlights the need for research and training in providing palliative and hospice care for patients with CHF.
A good death is a human right. Studies have found that many end-stage patients with heart failure were still receiving inappropriate life-sustaining treatment, including intensive care hospitalization and, cardiopulmonary resuscitation.
The ICU admission rate before death in patients with CHF changed by introduction of hospice care for CHF patients. Despite this downward trend, nearly half of all patients with CHF were admitted to the ICU before death and received life-sustaining treatment. However, even though the number of people who have adopted hospice-related services has increased, few patients with CHF received hospice care in the last month of life. Therefore, the overall utilization of hospice services was diminutive.
The progression of heart failure is highly variable, and the course is uncertain in clinical practice. Early multidisciplinary palliative care may benefit the quality of life and even medical utilization for patients with limited prognoses with CHF. Enhancing cardiologists’ awareness and confidence in managing the end of life care and advance care planning in collaboration with palliative care teams to communicate and prepare patients at the end of life is a future effort in caring for patients with CHF.
Introduction
Chronic heart failure (CHF) is a global health concern that affects nearly 40 million people worldwide each year and places constant pressure on public health systems and healthcare institutions due to substantial mortality, morbidity, and hospitalization rates. The incidence of CHF is expected to continue to rise with an aging global population. 1 The global economic cost of heart failure includes the direct costs to healthcare systems and the indirect costs to society due to lost productivity. The greatest expenses occur in the last 3 months of life. 2
Recent studies have shown that the average three-year survival rate after diagnosis with CHF is only 25%, which is even lower than that of cancer patients. 3 Therefore, the American College of Cardiology and the American Heart Association have jointly proposed an integrated care model for CHF that advocates comprehensive, palliative care. 4 However, the proportion of cardiac patients who receive hospice or palliative care before death is insufficient.5,6 A study on the location and cost of death among CHF patients found a significant increase in medical treatment and consumption of medical resources among patients admitted to intensive care units (ICUs) in the last 30 days of life. 7 However, resuscitation, intubation, and ventilation are high-cost treatments that neither significantly reduce patient mortality nor improve satisfaction with care. 8 Another study found higher terminal care costs to be correlated with poorer quality of care in the last stage of life. 9
Assessment of the quality of life and the quality of care at EOL can only be performed with the data available. Therefore, such research is usually conducted, either prospectively or retrospectively, with patients in ICUs. 10 To date, little is known about the practices for ICU admission, mechanical ventilation (MV), cardiopulmonary resuscitation (CPR), and extracorporeal membrane oxygenation (ECMO) adopted for terminal CHF patients or about their utilization of hospice-related services. Therefore, this study aimed to investigate trends in intensive care and hospice care among patients with CHF in the last month of life in Taiwan.
Methods
Study Design and Population
This was a population-based retrospective, observational study using data from the National Health Insurance (NHI) research database of Taiwan.11,12 We aimed to investigate trends in intensive procedures and hospice care for patients with CHF in the last month of life from 2001 to 2013. Since September 2009, NHI coverage for hospice and palliative services was expanded to include 8 non-cancer chronic diseases, including CHF, officially extending hospice and palliative care to CHF patients. We also focused on the impact of introducing palliative care for CHF in 2009.
Our study defined end-of-life as the last 30 days before death. All terminal CHF patients with NHI were included, with both primary and secondary diagnostic codes, as defined by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), assigned at hospital admissions used to identify CHF patients. The primary diagnostic code was 428, while the secondary codes were 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, and 404.93. The ICD-9 code of heart failure admission under NHI research database with high accuracy and validated by previous studies.13,14
In the claims data, each patient’s last hospital discharge was recorded as discharged against medical advice (DAMA), against advice discharge (AAD), discharged in critical condition (critical AAD), or in-hospital death. A hospital admission date was mandatory for inclusion in this study so that the 30 days before critical AAD could be determined. We considered discharge records indicating death in the hospital conclusive because Taiwanese people usually prefer to die in their homes.15,16 We excluded patients aged <18 years, patients with a cancer diagnosis, and those for whom there was no outpatient or inpatient information declared within 6 months due to a diagnosis of CHF before death.
After identifying patients in the database who were suitable for inclusion, we collected and collated information on intensive treatments received (including ICU admission, MV, CPR, and ECMO) and hospice-related services utilized during the last month of life. We computed utilization rates and analyzed the trends in intensive treatment and hospice-related service use. These treatments or hospice care were identified based on the NHI procedure or order claim codes (the total included 1653 item codes).
Ethics Statement
This study was conducted in accordance with the 2013 revision of the Declaration of Helsinki and the World Medical Association Declaration of Taipei on ethical considerations in the research use of health databases. The study protocol was reviewed and approved by the Institutional Review Board of Kaohsiung Medical University, Chung-Ho Memorial Hospital (No. KMUHIRB- E(II)-20170146). The requirement for informed consent was waived because of the low-risk nature of this retrospective study, and all data converted from the original NHI claim records were anonymized and encrypted according to strict regulations.
Measurements
Mortality due to CHF
The deaths of CHF patients with a final discharge status of in-hospital death, DAMA, or critical AAD were classed as death due to CHF. In Taiwan, critical AAD is unique to patients with terminal illnesses. Some Taiwanese people, especially older adults, believe that dying at home brings good fortune. Critical AAD is also described as impending death discharge or terminal discharge. The validity of discharges recorded as critical AAD in Taiwan has been investigated, and the overall accuracy and positive predictive value for mortality coding on discharge status were higher than 97% in the week after discharge. 17
Intensive procedures and hospice-related services
Medical procedures defined as intensive have been identified in previous studies as ICU admission, MV, CPR, and ECMO.7,8,15,18 Indicators of hospice-related service utilization were identified as hospice ward admission, receipt of hospice shared care, and hospice home care. All information on these indicators was obtained from the NHI research database using the claims order code for the last month of life.
Patient demographics and disease characteristics
Patient demographics, including sex and age at the time of death, were collected. Patient disease characteristics were classified according to Charlson et al Comorbidity Index (CCI) scores, 19 which were calculated according to the ICD-9-CM codes recorded in the last year of admission before death. 20 The CCI score was used for the last month of life hospitalization records and grouped into 0, 1, and ≥2.
Healthcare institutions and primary physician specialties
We identified the primary hospital as the hospital to which the patient was last admitted during the last month of life. We recorded the characteristics of the healthcare institutions, including hospital level (medical center, regional hospital, or district hospital), teaching status (teaching or nonteaching hospital), ownership (public or private), and medical department (cardiology, cardiovascular surgery, thoracic and critical care, or other).
Statistical Analysis
Descriptive statistics were used to describe the demographic characteristics of the patients and healthcare institutions. A joinpoint regression analysis was performed to analyze trends in the administration of intensive procedures and the use of hospice-related services. 21 All statistical analyses were performed using SAS® Enterprise Guide 7.0 (SAS Institute Inc., North Carolina, USA) and Joinpoint trend analysis software 4.5.0.1 (National Cancer Institute, Bethesda, Maryland, USA).
Results
Patient Characteristics
We analyzed the data of 25 375 CHF patients in the last month of life in Taiwan between 2001 and 2013. The cohort included 12 831 females (50.57%) and 12 544 males (49.43%). Patients aged 75 to 84 years constituted the largest proportion (37.15%) of the cohort, followed by those aged >85 years (32.48%). A total of 55.91% of patients had CCI scores ≥1. Inpatient treatment was most often in cardiology departments (41%), followed by thoracic and critical care departments (39%). The largest proportion of patients were treated at regional hospitals (43%), and most of the healthcare institutions were private teaching hospitals. Further details are provided in Table 1.
Demographic and Clinical Characteristics of CHF Patients in the Last Month of Life in Taiwan Between 2001 and 2013, Including Intensive and Supportive Treatments Received.

CCI = Charlson Comorbidity Index; CHF = chronic heart failure; CPR = cardiopulmonary resuscitation; ECMO = extracorporeal membrane
Intensive Care and Hospice Care
Among the patients in our cohort, 13 516 (53.27%) were admitted to ICUs. MV and CPR were administered to 50.37% and 28.69% of the patients, respectively. A total of 327 (1.29%) patients received ECMO. However, only 222 (0.87%) received hospice care in the last month of life (Table 1).
Trends in Intensive Procedure Administration
There was an upward trend in ICU admissions between 2001 and 2003 (53%–57%) and then a significant decrease between 2003 and 2013 (57%–48%, annual percent change [APC] = −1.65, P < .05) (Table 2 and Figure 1). Treatment with CPR also showed a significant decrease from 2003 to 2013 (41%–17%, APC = −7.49, P < .05) (Table 3 and Figure 2). Treatment with ECMO showed a significant increase from 2001 to 2008 (0.52%–2.22%, APC = 23.17, P < .05) and then a nonsignificant decrease from 2008 to 2013 (2.22%–1.78%, APC = −1.54, P > .05) (Table 3 and Figure 3). From 2001 to 2013, the use of mechanical ventilation decreased significantly (54%–42%, APC = −2.29, P < .05). Hospice resource utilization did not exceed 1% from 2001 to 2010. It rose to 4.36% in 2013, but this increase did not reach statistical significance (Table 2).
Intensive Procedures Used With CHF Patients and Their Use of Hospice Services in the Last Month of Life in Taiwan Between 2001 and 2013.

CHF = chronic heart failure; CPR = cardiopulmonary resuscitation; ECMO = extracorporeal membrane oxygenation; ICU = intensive care unit; MV = mechanical ventilation.
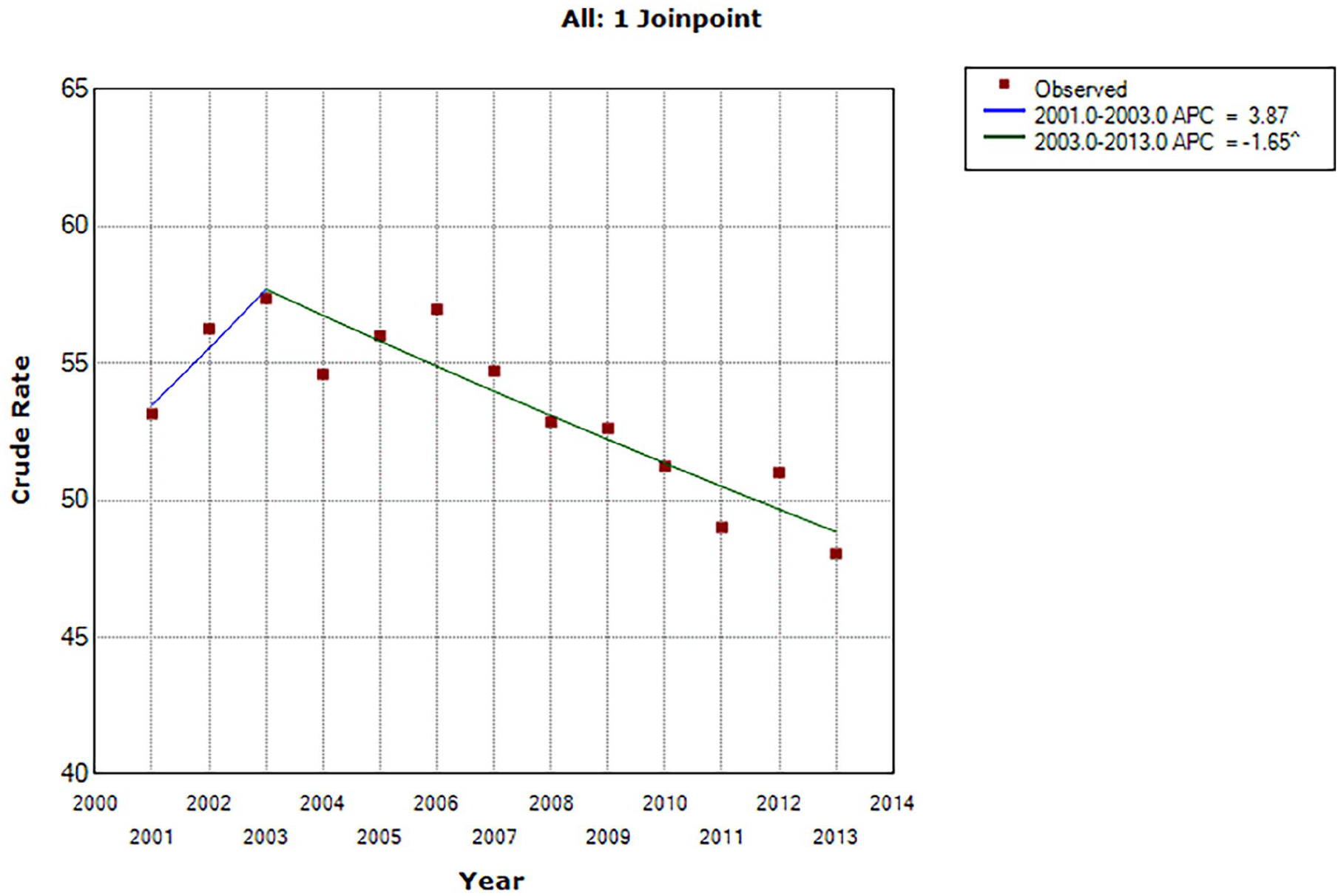
Joinpoint analysis of trends in Taiwan in chronic heart failure patient admission to intensive care units in the last month of life between 2001 and 2013.
Joinpoint Analyses of Trends in Intensive Treatment of CHF Patients in the Last Month of Life Between 2001 and 2013 in Taiwan.

APC = annual percentage change; CHF = chronic heart failure; CPR = cardiopulmonary resuscitation; ECMO = extracorporeal membrane oxygenation; ICU = intensive care unit; MV = mechanical ventilation.
P < .05.
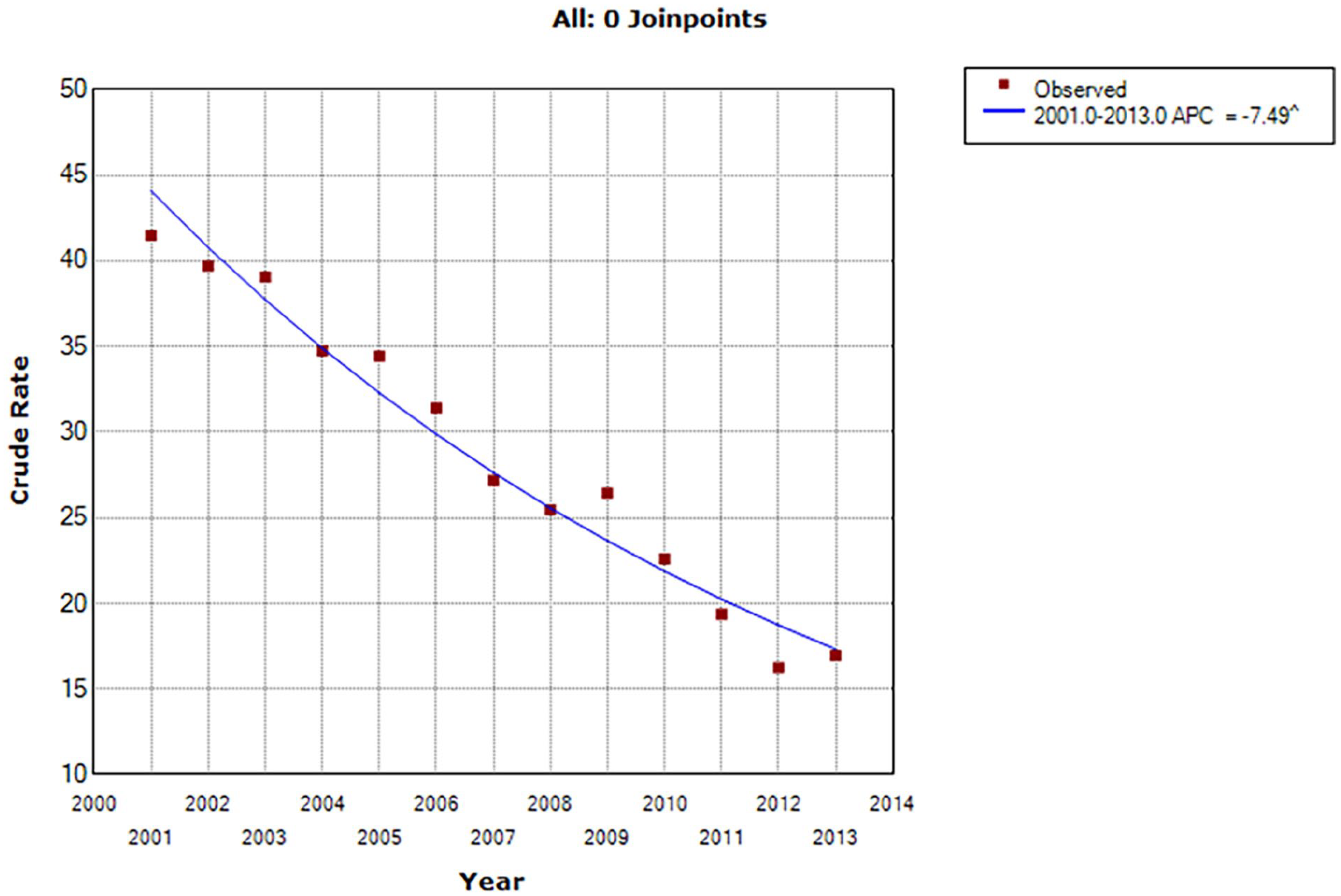
Joinpoint analysis of trends in Taiwan in the administration of cardiopulmonary resuscitation to chronic heart failure patients in the last month of life between 2001 and 2013.
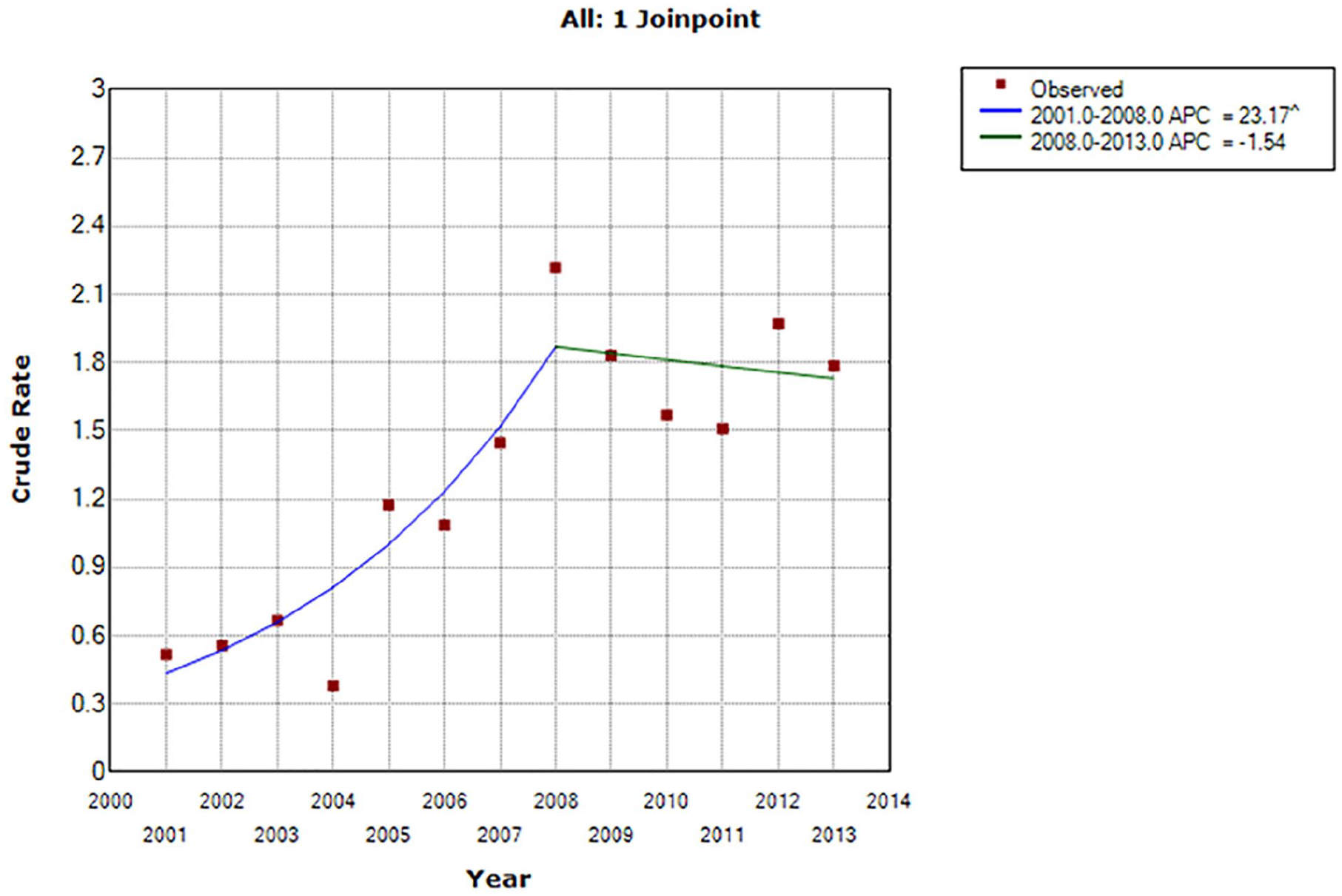
Joinpoint analysis of trends in Taiwan in the administration of extracorporeal membrane oxygenation to chronic heart failure patients in the last month of life between 2001 and 2013.
Discussion
To the best of our knowledge, this is the first study to examine the use of ICU, CPR, MV, ECMO, and hospice-related services among terminal CHF patients in a large Asian population. We found that 53% of patients were admitted to the ICU, and CPR, MV, and ECMO use significantly decreased between 2003 and 2013. In addition, while hospice resource utilization increased by 4.36% over this period, it remained within 1% between 2003 and 2013.
We found that the ICU admission rate before death increased from 53% in 2001 to 57% in 2003 and then significantly declined to 47% in 2013. Despite this downward trend, nearly half of the CHF patients in our cohort were admitted to the ICU in the month before their death and received life-sustaining treatment. A recent Taiwanese study among stroke patients in the month before death showed that 25.4% were admitted to an ICU in their last month of life. 16 Another study found that 28.58% of cancer patients were admitted to the ICU in the year before death. 22 In the present study, ICU admission rates between 2001 and 2013 ranged from 48% to 53%. Therefore, our data indicate that patients with CHF have a higher rate of ICU admission at EOL than those with stroke and cancer. Patients with heart failure experience multiple symptoms, particularly during the terminal stage. 23 Symptoms of respiratory distress and anxiety are as severe as the same symptoms in cancer patients. Heart failure patients often have an acute progressive phase; this gradual process often requires hospitalization. The clinical features of acute attacks are a combination of dyspnea and low-output symptoms. This may also be why HF patients have higher ICU admission rates than cancer and stroke patients. 24 However, patients with CHF have nearly double the ICU admission rate in the terminal stage of their lives, affecting the cost and quality of CHF terminal care. ICU admission is important for the assessment of EOL quality. 10 However, the corresponding increase in overall care expenditures at the EOL for illnesses produces no improvement in patient mortality or satisfaction with care.9,25 Furthermore, some studies have shown that the higher the cost of EOL care, the worse the10,26 patient’s quality of life. In addition, when patients were given a choice about life-sustaining treatment at EOL, 87% did not want to be intubated or placed on MV before death, even if such treatment could extend their life by 1 month. There were no significant differences in the proportion of patients that chose not to receive life-sustaining treatment in terms of age group, sex, or income level. Rather, 71% were willing to receive palliative drugs such as sedatives and painkillers even if they would shorten their lives. 27
CPR utilization showed a significant decrease from 2001 to 2013 (41%’17%, APC = −7.49, P < .05). In May 2000, the Legislative Yuan passed the “Hospice Palliative Care Act.” Taiwan is the first and only Asian-Pacific country to protect and respect natural death by legislation. Moreover, the act provides an official legal basis for rejecting CPR. Before the legislation, even though physicians might agree that first aid should not be performed based on the patient’s condition, not performing CPR risked legal action. The reduction in CPR may be partially attributable to attitudes toward the procedure in Taiwanese culture since many patients do not wish to receive the automated external defibrillation and extracardiac massage used during CPR. However, many are willing to receive intravenous fluids and blood transfusions to maintain blood pressure and to have an endotracheal tube inserted for MV. As a result, the rate of MV received by our cohort in the last month of life increased between 2001 and 2003 from 54% to 57% and decreased significantly between 2003 and 2013 from 57% to 42%. However, the percentage of patients treated with MV was much higher than that treated with CPR (from 41% in 2003 to 17% in 2013) at both ends of this downward trend, particularly by the final year of the study period. In Taiwan, MV is considered a less invasive treatment than CPR, and intubation is regarded as an acceptable means of sustaining life until all of the patient’s family has arrived to be present when the patient dies; this is seen as a symbol of fulfillment. Furthermore, maintaining a patient’s respiration so that they can die without a tube in their home is considered a preferable way to die, and this is likely to have contributed to the significant decrease in CPR.
In addition, in July 2000, to manage the shortage of ICU beds and restrict the use of medical resources, the NHI Board implemented an integrated delivery system (IDS) for patients in need of prolonged MV (PMV). This payment program is designed to encourage medical centers and regional hospitals to establish respiratory care centers. These programs provide active weaning ventilator support for hemodynamically stable patients receiving PMV. One study compared PMV usage after composite expected payments. They found that PMV was used in 3275 patients before IPP (1997-1999) and 4692 patients after IPP (2001-2003). 28 According to the IDS, the number of people who receive MV in Taiwan increased significantly from 2000 to 2005. The above reasons may be why CPR use dropped sharply from 41% to 17%, while MV use remained at 42% before death. Cultural circumstances affect the shared treatment decisions of physicians and EOL patients. Phua et al 26 found that while 48%–100% of physicians did not perform CPR on EOL patients, 6%–87% maintained MV, prescribed antibiotics, and provided vasopressors. These practices differ significantly from those of Western physicians who are more inclined to regard those at the EOL as do-not-resuscitate patients, with only 10%–40% of Western physicians maintaining ventilation, prescribing antibiotics, and providing vasopressors in last-stage terminal care. This suggests that Asian physicians are more aggressive in treating terminal illnesses in ICUs than their Western counterparts.29,30
Despite ongoing advances in medical treatment, there is not yet a cure for CHF. However, CHF patients have historically underutilized palliative and hospice care. Multidisciplinary palliative care may improve symptoms, increase patients’ quality of life and reduce the inappropriate use of medical resources for terminal CHF patients.31,32 The palliative care model aims to achieve physical, psychological, spiritual, and social well-being. The most important goal is the appropriate treatment of symptoms. In a study comparing patients with terminal CHF and end-stage lung or pancreatic cancer, those with terminal CHF displayed significantly more symptoms, a greater incidence of depression, and poorer mental health. 33 Patients with terminal CHF who received palliative care before heart transplantation complained of extreme distress from symptoms. However, their symptoms were significantly relieved by palliative care, and patient satisfaction with treatment improved. 34
Only 222 (0.87%) of the CHF patients in this study received hospice-related services in the last month of life between 2001 and 2013. In addition, almost no patients received hospice-related care between 2001 and 2009. However, the utilization of such services increased from 11 in 2010 to 88 in 2013. While this increase is encouraging, our results are consistent with those of previous research that has shown inadequate utilization of hospice and palliative care among CHF patients. 35 In 2009, medical insurance coverage for hospice and palliative services was expanded to include 8 noncancer chronic diseases, including CHF, dementia, and end-stage renal disease, officially extending hospice and palliative care to noncancer patients and publicly supporting the view that CHF patients at the EOL should also receive hospice and palliative care. As a result of this legislation, the overall utilization of hospice and palliative services has gradually increased in Taiwan since 2010.
The timing of hospice care is usually based on duration estimates for patient survival. However, research indicates that approximately 40% of CHF patients overestimate their life expectancy, 36 making it more difficult to engage them in discussions about EOL care. It has also been shown that physicians often fail to provide adequate information to CHF patients and their families about the expected progression of their condition. One study found that only 37% of CHF patients were aware of their poor prognosis, with only 8% of patients and 44% of their families informed of a very short life expectancy. This is likely to have been a major factor in the finding by the same study that 36% of CHF patients died alone. 37 A survey of families of deceased CHF patients found that only a third of them were aware before the patient’s death of their poor prognosis. 38
Recent studies have confirmed that only 52% of physicians discuss hospice and palliative care issues with EOL CHF patients. Among these, 11% reported feeling uncomfortable discussing this issue, 33% felt the families were not mentally prepared to discuss it, 9% were concerned about destroying the hope of families, and 8% felt there was not enough time to discuss hospice care. In addition, 30% of these physicians reported low confidence in their ability to discuss hospice and palliative services. 39 The course of CHF is more variable and unpredictable than that of cancer. In terminal cancer patients, the condition worsens steadily as the cancer progresses and the patient approaches death. However, in CHF, patients may experience acute symptoms and then stabilize, so they are often unprepared for death because of fluctuations in their condition. 22 Therefore, hospice and palliative care for CHF patients is more challenging than for cancer patients. Strengthening the awareness of cardiologists and their confidence in the management and planning of EOL care and encouraging their collaboration with hospices and palliative teams 40 are areas of continuing professional development that should be addressed.
Strengths and Limitations
More representative and comprehensive data in the NHI research database facilitate better decision-making based on a wider range of sources. 41 Several international multidatabase studies have been published that include the NHI research database, which is among the core data resources for international comparative studies conducted by the Asian Pharmaco-epidemiology Network. 11 Taiwan’s NHI is a single-payer compulsory health insurance system launched in March 1995 that covers 99% of the national population. Hence, the database sufficiently covers all patient groups. An advantage of studies such as ours that use data from claims databases over randomized controlled trials is that they can be performed relatively inexpensively, include vast patient cohorts and have long follow-up periods. Our population-based results provide specific, valid, and reliable data on the evidence of EOL care for CHF patients in Taiwan.
However, this study had several limitations. First, we used claims data to assess EOL care. This may be imprecise as it depends on the accuracy of coding, some essential clinical information is not collected in claims data, and the data may not be an accurate means of identifying patients with CHF at the EOL. Second, as with all observational studies, our nonexperimental results could not establish causality. Finally, the data used were from 2001 to 2013, and more recent clinical practices and protocols may differ from those used in that period. Third, we did not analyze how institutional characteristics relate to CHF at the EOL. In the end, we only included patients with in-hospital death or critical illness discharge; the patients who chose not to come to the hospital before death were not evaluated in this study.
Conclusions
Palliative care is an essential component of integrated CHF care. 42 However, the rates of ICU admission and life-sustaining treatment among patients with CHF in the month before death are high, and there is poor utilization of hospice-related services. Improving palliative care and hospice services may reduce the symptoms and increase the quality of life of CHF patients at the EOL, as well as reduce their use of nonbeneficial healthcare resources and the associated economic costs.
Footnotes
Acknowledgements
The authors wish to acknowledge the support of the Maintenance Project (CLRPG3D0049) of the Center for Big Data Analytics and Statistics at Chang Gung Memorial Hospital for study statistical analysis.
Author’s Note
Pi-Ling Chou and Pei-Chao Lin is also affiliated to Department of Medical Research, Kaohsiung Medical University Chung-Ho Memorial Hospital, Kaohsiung, Taiwan;Institute of Medical Science and Technology, National Sun Yat-Sen University, Kaohsiung, Taiwan.
Chia-Chin Lin is also affiliated to Taipei Medical University, Taipei, Taiwan.
Hsiang-Chun Lee is also affiliated to School of Medicine, College of Medicine,Kaohsiung Medical University, Kaohsiung, Taiwan; Graduate Institute of Animal Vaccine Technology, National Pingtung University of Science and Technology, Pingtung, Taiwan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Ministry of Science and Technology (MOST), Taiwan (MOST-106-2410-H-037-016).
Ethics Statement
The studies were reviewed and approved by Kaohsiung Medical University Chung-Ho Memorial Hospital Institutional Review Board. (No. KMUHIRB- E(II)-20170146).