
Abstract
Institutional betrayal occurs when the institutions that people depend on fail to protect them from harm, which was exemplified by a failure to manage COVID-19 risks. Inpatient psychiatry provides a rich context for which to understand the effects of institutional betrayal, and this is amplified in the context of the COVID-19 pandemic. Using a retrospective cohort design, we administered an online survey to former patients (n = 172) of inpatient psychiatry hospitalized at the height of the COVID-19 pandemic (March 2020 to February 2021) to understand the relationship between facilities’ use of COVID-19 mitigation activities (ie, offering or requiring face masks, keeping patients and staff 6 feet apart, access to hand sanitizer, use of telemedicine for clinical consults, and routine cleanliness of the unit) and former patients’ reports of institutional betrayal, changes in their trust in mental healthcare providers, fear of getting sick, and having contracted or witnessed someone else contract COVID-19. The quantity of COVID-19 mitigation activities was monotonically negatively associated with the probability of reporting any betrayal, the probability of reduced trust in mental healthcare providers, and the probability of being afraid of getting sick always or most of the time while hospitalized. COVID-19 mitigation activities either directly affected these psychological outcomes, or facilities that engaged in robust mitigation had greater cultures of safety and care quality. Additional qualitative work is needed to understand these mechanisms.
Keywords
We know that experiences of institutional betrayal have been associated with reduced trust and negative health outcomes in general healthcare settings.
This research extends our understanding of how the COVID-19 pandemic affected patient experience within inpatient psychiatric facilities, including experiences of betrayal and changes in patients’ trust in mental healthcare providers.
Our findings highlight the importance of inpatient psychiatric facilities in being able to implement robust COVID-19 mitigation activities, suggesting that doing so is positively aligned with other indicators of patient experience and outcomes.
Introduction
As a society, we depend on institutions, such as healthcare systems, schools, and courts, to provide the structure, norms, and rules that govern and shape our lives and social interactions. The relationships between individuals and the institutions they interface with can be powerful, often requiring that individuals have a certain degree of trust that such institutions will protect them or, at the very least, not unduly harm them. There can be serious psychological effects when institutions fail to protect the individuals who depend on them from harm. This type of failure to protect, including the direct infliction or maintenance of harm, is referred to as institutional betrayal.1,2
Institutional betrayal has been studied in many contexts, such as sports, military, healthcare, government, and educational institutions, all reporting similar negative psychological outcomes.1,3 -7 Some of the foundational empirical work on institutional betrayal was focused on the general context of healthcare, finding that experiences of institutional betrayal are associated with lower levels of trust and engagement with care. 1 Inpatient psychiatric care is arguably one of the most vulnerable settings in healthcare, 8 where patients are especially dependent on the hospital. This dependency coincides with the discounting of psychiatric patients’ realities and the limiting of autonomous decisions. Indeed, it is the only healthcare setting where patients can be subjected to involuntary treatment and imprisonment without committing a crime. Given this, inpatient psychiatry provides a rich context for which to understand the effects of institutional betrayal, and this is amplified in the context of the COVID-19 pandemic.
Through the lens of COVID-19, several studies have examined the effects of an institution’s actions and inactions related to COVID-19 on the health of those dependent on the institution. For example, a study of undergraduate students’ experiences of institutional betrayal found that students reported experiencing betrayal due to their universities’ handling of COVID-19 and that this institutional betrayal was related to psychological distress. 9 In addition, a study examining the impact of the COVID-19 pandemic on adults with serious mental illness found that of the 20 adults interviewed in their study, several indicated an inability to access mental health care and public health benefits. 10
In the context of inpatient psychiatry, specifically, there are extreme power imbalances, and the patient is particularly dependent on clinicians, hospital policies, and organizations’ overall structure and norms. Compared to other healthcare settings, inpatient psychiatric facilities have congregated care environments. Patients spend their days in shared living spaces, often share a bedroom with others, and receive treatments in group settings. This congregate nature increased the risk of COVID-19 spread, similar to nursing homes, jails, and prisons. During the pandemic, inpatient psychiatric facilities had to balance the need to protect patients in these facilities from contracting the virus, while also attempting to provide treatment for the conditions they presented with. 11 The latter requires close contact, face-to-face meetings, and even group therapy, all increasing the risk of spreading COVID-19. Mitigation efforts included using proper personal protective equipment (eg, face masks) by providers and patients, use of telehealth for clinical consults, accessibility of hand sanitization, social distancing, and unit cleanliness. 12
Moreover, unlike patients in other inpatient hospital settings, patients in inpatient psychiatry are being treated principally for reasons related to psychological and emotional distress, many of whom have high rates of prior trauma, making them especially sensitive to the mishandling of COVID-19 risk mitigation and betrayal. Therefore, both patients’ risks of harm and their vulnerabilities were exacerbated during the pandemic. Physical harm could have derived from contracting the virus during one’s hospitalization. Psychological harm could have come from patients feeling betrayed by their respective facility’s lack of COVID-19 mitigation, mismanagement of their care, and fear of contracting the virus or witnessing another patient suffer or even die from the virus. These harms could have impacted proximal outcomes, such as changes in patients’ trust in mental healthcare providers.
While there has been some emerging research on institutional betrayal in general healthcare settings, as well as within the context of COVID-19 and risk mitigation management, we are unaware of any study that focuses on institutional betrayal in the setting of inpatient psychiatric facilities, specifically. In this study, we describe patients’ experiences of COVID-19 mitigation activities in inpatient psychiatry and its relationship with reports of institutional betrayal, as well as outcomes of trust, fear of contracting COVID-19, and contracting or witnessing someone else contract COVID-19 while hospitalized during the peak of the COVID-19 pandemic. Given both the theory and prior empirical evidence of institutional betrayal, we hypothesized that the use of COVID-19 mitigation activities would be inversely associated with participant’s experiences of institutional betrayal, reduction in trust, fear of contracting the virus, and the likelihood of contracting the virus or witnessing someone else contract the virus.
Methods
Procedure
Using a retrospective cohort design and convenience sampling strategy, we administered an online survey in early 2021 to former adult patients of inpatient psychiatry who had been hospitalized between March 2020 to February 2021, which captured the height of the COVID-19 era. The aim of the current study was focused on the COVID-19 era, though this was part of a larger study that included people hospitalized before the COVID-19 era; findings from the larger study have been published elsewhere. 13 We aimed to recruit at least 80 participants hospitalized during the COVID-19 era, enabling us to detect a moderate effect size with 80% power. To be eligible for the study, participants had to have been hospitalized at least once during the target timeframe, been aged 18 or older during their most recent psychiatric hospitalization, and their most recent hospitalization had to have taken place in the United States. The survey was disseminated through social media platforms and email listservs. Participants were presented with a consent form and were then asked to report on a series of questions related to demographic and clinical information, followed by distinct measures of care experiences, including measures of COVID-19 mitigation and institutional betrayal. Participants could enter to win a $20 gift card through a lottery. Data were screened for suspicious responses (eg, bots) using best practices. This study was approved by the Institutional Review Board at the University of Pennsylvania (#844878).
Measures
Demographic characteristics included age (18-24, 25-34, 35-44, 45, and over), gender (male, female, non-binary), race (Non-Hispanic white, Non-Hispanic Black, Non-Hispanic Asian, Non-Hispanic Native/Pacific Islander, Non-Hispanic “Other”), ethnicity (Hispanic/Latinx vs not Hispanic/Latinx), income ($0 to $24 999, $25 000 to $49 999, $50 000 to $99 999, $100 000 and greater), education (high school diploma/GED or less, some college, trade school or associate degree, 4-year college degree, advanced degree [eg, master’s, Ph.D., M.D., J.D.]), had health insurance (yes vs no), first time being hospitalized in a psychiatric facility (yes vs no), voluntary status (yes vs no), hospitalized for suicidality (yes vs no), year of hospitalization (2020vs 2021), and degree of trust in receiving high-quality care at time of admission (not at all, very little, a good deal, or very much).
Analysis
Analysis was performed using STATA/BE 17.0. We first report univariate descriptive statistics to describe the distribution of COVID-19 mitigation activities experienced by participants, as well as their experiences of institutional betrayal. We then fit a series of parametric multiple linear probability models predicting the 4 outcomes: Having experienced any betrayal, reporting a reduction in trust in mental healthcare providers due to the hospitalization, being always or mostly worried about contracting COVID-19 while hospitalized, and contracting COVID-19 or witnessing someone else with it while hospitalized. All regression models controlled for demographic characteristics. This significance threshold defined for our analyses was 0.05. To support ease of interpretation, the only continuous variable in our study, a measure of institutional betrayal, was converted into a binary variable. Since we were primarily interested in the presence of betrayal, and not the number of betrayal events, the dichotomization of this variable was both conceptually and pragmatically appropriate. Predicted probabilities of outcomes were produced from each regression model across quartiles on the COVID-19 mitigation summary score. Lastly, presence of multicollinearity among the 4 models was checked; no evidence of multicollinearity was found as indicated by variance inflation factors not exceeding the default cut-off value of 5.
Results
Table 1 reports descriptive statistics of our sample. A total of 172 people responded to the survey who had been hospitalized during the COVID-19 era, which was 21.1% of the larger study sample (n = 814). This sub-sample of COVID-19-era patients differed from those hospitalized before COVID-19 in several ways. Specifically, the COVID-19-era sample had a higher proportion of female and non-Hispanic white patients, as well as a higher proportion of individuals with low income (those earning $0-$24 999) and those hospitalized due to suicidality. See Appendix Exhibit 2 for full sample comparisons on clinical and demographic characteristics. Among our current study sample of participants hospitalized during the COVID-19 era, 77.9% (n = 134) were below the age of 35, 60.5% (n = 104) were female, 7.6% (n = 13) were non-binary, 71.5% (n = 123) were non-Hispanic/Latinx white, 43.6% (n = 75) made less than $25 000 a year, 11.6% (n = 20) made $100 000 or more a year, and the majority 62.2% (n = 107) had less than a 4-year college degree. About half had been hospitalized voluntarily 46.1% (n = 76), 33.1% (n = 57) were hospitalized for the first time, and most were hospitalized for reasons related to suicidality, 77.9% (n = 134). Missingness on individual items ranged from 0% to 8.7%. The summary score of the COVID-19 mitigation activities had good reliability (α =.84) as did the summary score of the IBQ measure (α =.88).
Sociodemographic Characteristics of Participants.

Table 2 reports the distribution of specific COVID-19 mitigation activities and Appendix Exhibit 3 reports the distribution across quartiles. Less than half (n = 78) and a third (n = 52) of participants reported always being offered and required to wear face masks, respectively, and almost a quarter (n = 37) were never offered a mask. Less than a third (n = 50) reported always having easy access to hand sanitizer, and over a quarter (n = 47) reported never having easy access to hand sanitizer. Just 10.4% (n = 17) reported that patients and staff were always kept 6 feet apart, and more than a third (n = 56) reported never being kept 6 feet apart. Just 6.7% (n = 11) of participants reported that they always met with clinicians via telemedicine, and the majority (n = 95) reported never meeting with clinicians via telemedicine. Finally, about a third (n = 56) reported that the unit was always properly cleaned and sanitized regularly, and 11.59% (n = 19) reported that the unit was never properly cleaned and sanitized regularly. See Appendix Exhibit 3 for full statistics on the mitigation summary score.
Distribution of COVID-19 Mitigation Activities and Checklist Measure of Institutional Betrayal That Participants Reported Experiencing While Hospitalized.
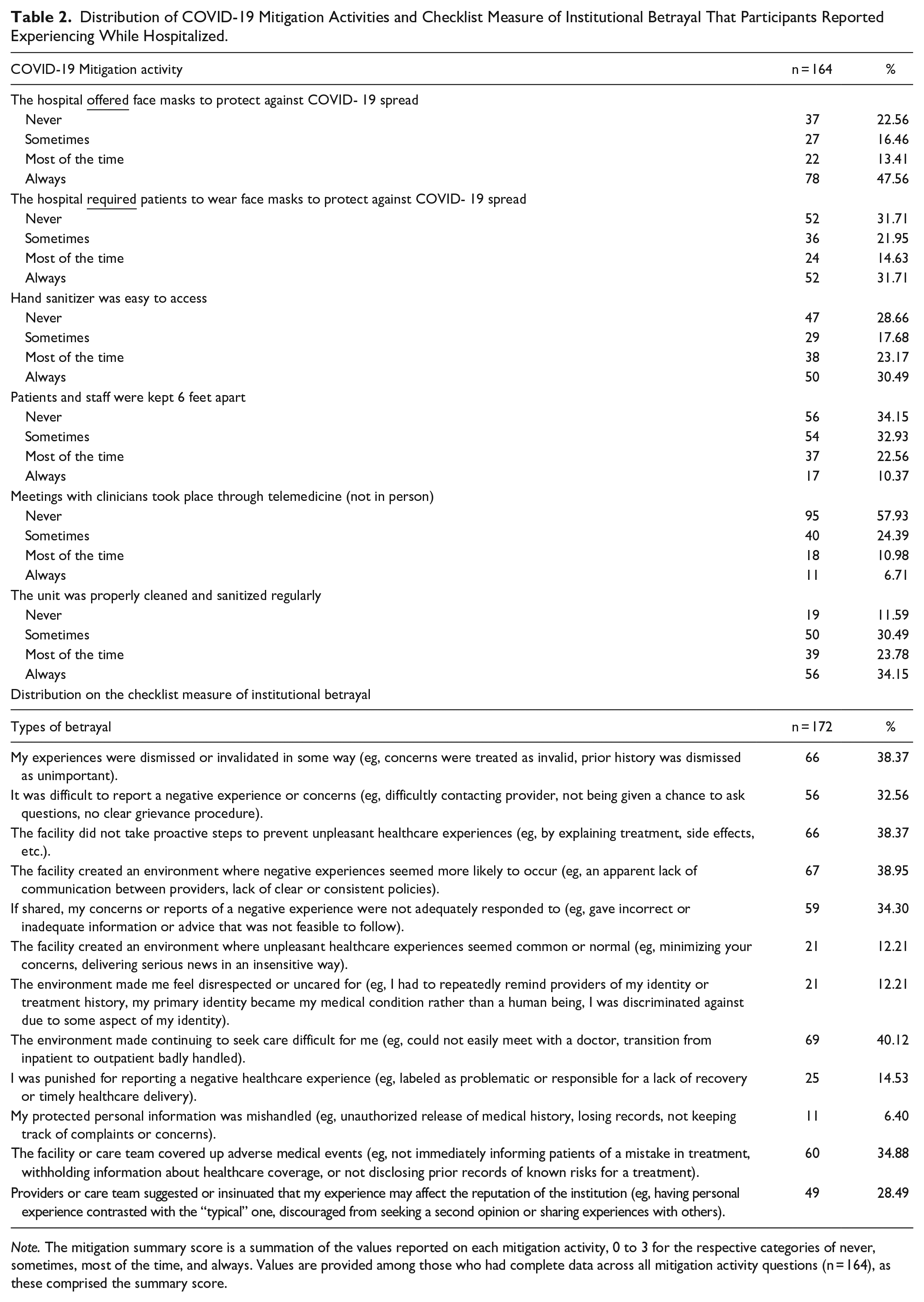
Note. The mitigation summary score is a summation of the values reported on each mitigation activity, 0 to 3 for the respective categories of never, sometimes, most of the time, and always. Values are provided among those who had complete data across all mitigation activity questions (n = 164), as these comprised the summary score.
Table 2 reports the distribution of the different betrayal types. The most common betrayal type was “The environment made continuing to seek care difficult for me (eg, could not easily meet with a doctor, transition from inpatient to outpatient badly handled)” at 40.12% (n = 69). The least common betrayal type was “My protected personal information was mishandled (eg, unauthorized release of medical history, losing records, not keeping track of complaints or concerns)” at 6.40% (n = 11). Appendix Exhibit 4 reports the full distribution in the quantity (number) of betrayal types. Furthermore, Appendix Exhibit 4 reports additional statistics on the institutional betrayal summary score. More than a third of participants (37.2%, n = 64) reported experiencing zero betrayal types during their hospitalization, and another third reported more than 3 betrayal types during their hospitalization (36.6%, n = 63). These extremes were followed by 10.5% (n = 18) who experienced 1 type, 8.7% (n = 15) who experienced 2 types, and 7.0% (n = 12) who experienced 3 types.
Table 3 reports predicted probabilities from the linear probability models. There was a monotonic negative relationship between the number of mitigation activities and the probability of experiencing institutional betrayal (predicted probability [PP] for the bottom 25% in mitigation activity = .85 versus .37 for the top 25%, P < .001). There was also a monotonic negative relationship between the number of mitigation activities and the probability of the participant reporting that their hospitalization experience reduced their trust in mental health providers (PP for the bottom 25% in mitigation activity = .74 vs .44 for the top 25%, P < .001). Finally, there was a negative relationship between the number of mitigation activities and the probability that the participant reported being mostly or always afraid of contracting COVID-19 while hospitalized (PP for the bottom 25% in mitigation activity = .51 vs .25 for the top 25%, P < .01). We do not show predicted probabilities from the regression model with the outcome of contracting or witnessing someone else contract COVID-19 while hospitalized because the mitigation quartile measure was not a significant predictor of that outcome. See Appendix Exhibit 5 for the full regression models.
Predicted Probabilities for Mitigation Summary Score Quartiles.
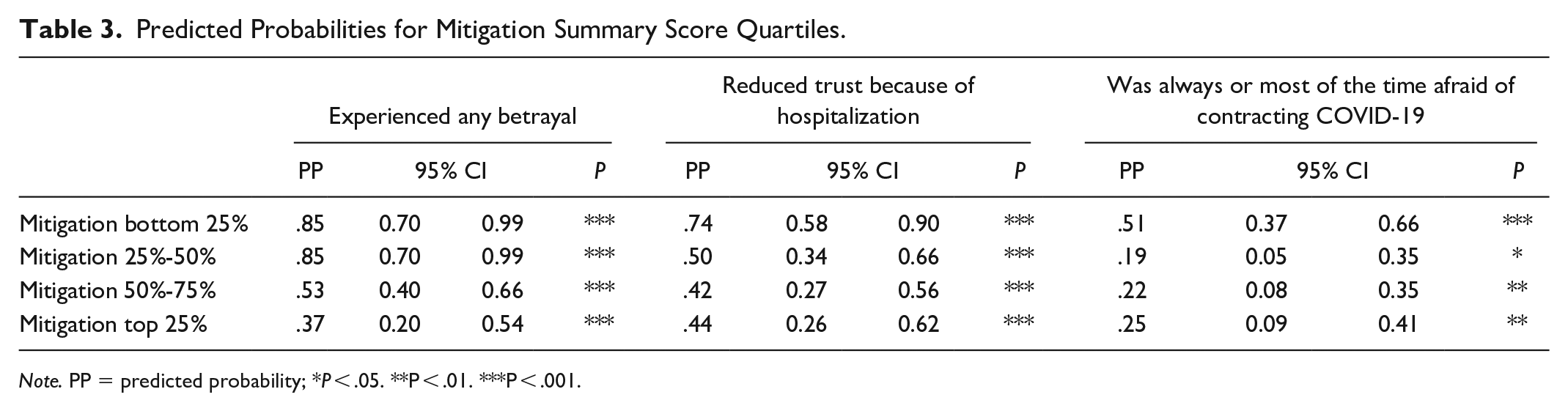
Note. PP = predicted probability; *P < .05. **P < .01. ***P < .001.
Discussion
Our results emphasize the complex dynamic between inpatient psychiatric facilities and the patients they serve, which grew more complex during the COVID-19 pandemic. We found that patients who were hospitalized in psychiatric facilities with relatively low use of COVID-19 mitigation activities had a higher likelihood of having experienced any institutional betrayal, reporting a reduction in trust in mental healthcare providers due to their hospitalization, and having a great deal of fear in getting sick while hospitalized. These findings echo the importance of trust between patient and provider, but also the impact that fostering safe environments within the healthcare setting can have on both proximal and distal healthcare outcomes. Moreover, our findings demonstrate the impacts that the COVID-19 pandemic had on vulnerable populations like those in inpatient psychiatric facilities. This population is particularly vulnerable not only because of the congregate nature of inpatient facilities which increased their risk of contracting COVID-19, but also because of the conditions they were being treated for, which are often rooted in psychological and emotional distress. Many of the patients in inpatient psychiatric facilities have high rates of prior trauma, making them especially sensitive to the mishandling of COVID-19 risk mitigation and betrayal. Consequently, these findings offer crucial insights into instances of institutional betrayal within the healthcare system. They underscore the significance of trust in the patient-provider relationship and shed light on the repercussions of the COVID-19 pandemic on a demographic that has not been thoroughly examined.
Inpatient psychiatry patients are an especially vulnerable patient population, regardless of COVID-19. Prior work has described patients’ reports of psychological harm resulting from their psychiatric hospitalization.15 -17 Indeed, the rates of suicide are highest immediately following discharge from inpatient psychiatry,18,19 leaving some to suggest that adverse experiences might cause iatrogenic harm and contribute to negative outcomes.20,21 The COVID-19 pandemic raised the risks of harm, which effectively reduced the benefits that patients could receive. Moreover, the pandemic created a unique opportunity for inpatient psychiatric facilities to protect patients from harm related to COVID-19 or to put them at risk, especially given the congregate nature of inpatient psychiatry. While our results demonstrate a relationship between mitigation activity and reports of betrayal, reduced trust in mental healthcare providers, and fear of getting sick, it is unclear what the association of mitigation activity was on more distal outcomes (eg, post-discharge engagement in care) and the mediating role that trust played in those associations. We did not find a relationship between mitigation activity and having contracted COVID-19 or witnessing someone else contract the virus while hospitalized; this is likely due to the rarity of this event in the data and, therefore, not enough statistical power to identify an effect.
Given the retrospective design of the study, it is unclear to what extent COVID-19 mitigation activity had a causal impact on these outcomes, or if there was an underlying construct associated with both the propensity of organizations to engage in mitigation efforts and the quality of care provided to patients. It is reasonable to suspect that inpatient psychiatric facilities that already had “cultures of betrayal” were predisposed to not invest in COVID-19 mitigation as much as facilities that had greater cultures of safety and quality. Indeed, there is significant evidence demonstrating the role that healthcare cultures have on safety outcomes and patient-centered care environments,22 -24 and these may also be associated with the overall resources available to facilities (eg, flexible financing, opportunity for reinvestment, staff composition and retention).
Future research is needed to better understand differences in how psychiatric patients perceive institutional betrayal and its impacts on short- and long-term outcomes, including outcomes of suicide, readmission, engagement with care, and the development of hospital-acquired trauma symptoms. Additional research is also needed to understand the role that culture plays in both the everyday management of a psychiatric facility and care quality, as well as response to external crises that might destabilize care and require flexibility, diligence, and resources, such as with the COVID-19 pandemic.
Limitations
These results should be interpreted in the context of the limitations associated with this study. This study demonstrates that there is an association between COVID-19 mitigation activities and reports of experiencing institutional betrayal while hospitalized, changes in patient’s trust in mental healthcare providers, and fear of getting sick while hospitalized. Given both the cross-sectional design and omitted variables, we could not determine directionality or estimate a causal effect with certainty. As mentioned, a facility’s existing culture could underpin both robustness in mitigation efforts and other outcomes, such as trust. It is also possible that there were individual-level differences among participants that were associated with both their propensity to receive care at facilities with high or low mitigation and the valence of their outlook (ie, response bias on the questionnaires); however, we are not aware of any literature to support this speculation, and we controlled for observable patient characteristics in all regression models. Finally, participants were a convenience sample recruited online, so these results may not generalize to the average psychiatric patient hospitalized during the height of the COVID-19 pandemic.
In addition, some of the questionnaires administered to our study sample, particularly the COVID-19 mitigation activity questionnaire and questions relating to patient trust in mental healthcare providers, were not formally validated, though the institutional betrayal questionnaire checklist used in the study was validated.1,7,14 We are aware that the lack of validation of the listed questionnaires may contribute to possible measurement error. Nevertheless, the questions were associated with constructs in the expected direction, the questions related to trust were demonstrated to be associated with experiences of patient-centered care in the larger study, 13 and the questionnaire assessing the use of COVID-19 mitigation activities closely mirrors questions asked and validated elsewhere. 25
Conclusion
The results supported our hypothesis that former inpatient psychiatric care patients who were hospitalized in psychiatric facilities during the COVID-19 pandemic with relatively low use of COVID-19 mitigation activities had a higher likelihood of having experienced any institutional betrayal, reporting a reduction in trust in mental healthcare providers due to their hospitalization, and having a great deal of fear in getting sick while hospitalized. These results make a noteworthy contribution to the existing body of literature on institutional betrayal within healthcare settings. By specifically focusing on individuals with a history of inpatient psychiatric care during the pandemic, our study extends the understanding of how systemic factors, exacerbated by the unique challenges posed by the COVID-19 pandemic, can impact the trust dynamics between patients and mental healthcare providers. Moreover, our findings emphasize the pivotal role played by the pandemic in shaping the overall healthcare experiences of this particular demographic. The psychological and emotional distress often experienced by this patient population paired with the stress of a global health crisis and the congregate nature of their care unveils a complex interplay of factors that impacted certain healthcare outcomes. Lastly, the psychological impacts identified in our study, particularly the erosion of trust between patient and provider, emphasize the importance of fostering a more resilient and patient-centered mental healthcare system in the face of unforeseen challenges.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241237689 – Supplemental material for COVID-19 Mitigation Activities in Inpatient Psychiatry Were Associated With Patient-Reported Institutional Betrayal, Changes in Trust, and Fear of Getting Sick
Supplemental material, sj-docx-1-inq-10.1177_00469580241237689 for COVID-19 Mitigation Activities in Inpatient Psychiatry Were Associated With Patient-Reported Institutional Betrayal, Changes in Trust, and Fear of Getting Sick by Francis J. Ochman and Morgan C. Shields in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors report receiving a grant from the Centene Charitable Foundation (GF0012342, Shields).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.