
Abstract
This study investigates the association between socioeconomic position (SEP) – in terms of income and education – and mortality from neurodegenerative diseases, that is, dementia, parkinsonism, and motor neuron diseases (MNDs). We calculated age-standardized mortality rates and mortality rate ratios using log linear Poisson regression for different SEP groups, stratified by gender, age-group, and care home residency, utilizing the 2011 Belgian census linked to register data on cause-specific mortality for 2011 to 2016. Mortality was significantly higher in the lowest educational- and income groups. The largest disparities were found in dementia mortality. Income had a strong negative effect on parkinsonism mortality, education a positive effect. We found no significant association between SEP and MND. Our study provides evidence supporting the presence of socioeconomic disparities in mortality due to neurodegeneration. We found a strong negative association between SEP and NDD mortality, which varies between NDD, gender and care home residency.
Keywords
NDDs are recognized as a significant global public health concern, with documented connections to SEP, underscoring the critical importance of addressing these conditions for comprehensive public health strategies worldwide.
Our research provides evidence of socioeconomic disparities in mortality due to neurodegeneration, while unveiling distinct patterns for dementia, parkinsonism, and MNDs across gender and care home residency.
The findings underscore the importance of addressing socioeconomic inequalities in healthcare, emphasizing the need for targeted policy interventions, particularly in the context of NDDs.
Introduction
Neurodegenerative diseases (NDD) have become a major public health issue globally.1,2 With aging being the primary risk factor, 3 prevalence and mortality of NDDs are increasing at an alarming rate, especially in high-income countries.2,4,5 Belgium, in particular, is one of Europe’s leading countries when it comes to NDD mortality, with dementias being the leading cause of death among women and the fourth leading cause of death among men. 6 However, research on the association between socioeconomic position (SEP) and NDD mortality is scarce. 7 Addressing these inequalities in NDD mortality is critical as they impact the health and well-being of affected individuals and their families, and also have significant economic implications. Research on NDD risk factors impacts NDD disease management by early disease detection, leading to reduced disease incidence and health system burden. 8 By utilizing a high-quality population-based dataset including several socioeconomic (SE) indicators linked to information on cause-specific mortality, we can for the first-time study SE disparities in NDD mortality in Belgium.
As cognitive decline 9 is a clinical manifestation of dementia, education is the most commonly studied indicator of SEP in dementia research. 10 Studies among various elderly populations have shown that low education is associated with higher dementia mortality.11-17 Similarly, there is evidence to suggest that the risk of dying from dementia is higher in deprived income deciles.7,10,11 Fewer studies have been conducted for parkinsonian syndromes such as Parkinson’s Disease (PD) or secondary parkinsonism.18,19 The first study, conducted in Sweden, showed higher mortality rates in lower occupation-based SEP. 18 A Korean study found increased mortality in lower SE groups, measured by income and insurance type. 19 No studies have been conducted yet on the association between education and PD mortality, while research on PD prevalence and incidence is inconclusive; some studies showing a positive relationship between education and PD risk,20,21 others no association at all. 22 Motor neuron diseases (MNDs) are much rarer diseases than dementia and parkinsonism, and as such, few studies have focused on MND mortality. Hence, the relationship between SEP and MND mortality has never been studied before. Evidence provides insufficient support for an association between SEP and MND risk, 23 although some suggest there might be an association.24,25
The aim of this study is to unravel the association between different dimensions of SEP and NDD associated mortality. By simultaneously including various types of major NDDs – dementias, parkinsonism and MND – and by considering different SE indicators – educational attainment and income – this study will provide crucial insights into social inequalities in NDD mortality for the first time in Belgium. First, we will explore the relationship between SEP, measured by educational attainment and income, and mortality associated with NDDs. Given that these diseases predominantly affect the elderly population, 3 our secondary objective involves stratifying the analysis to determine if institutionalization in care homes influences the relationship between SEP and NDD mortality. This is important as NDDs have a huge impact on the quality of life of patients, often reducing their independence and requiring institutional care. By differentiating between individuals living at home and those living in care home, our study aims to shed light on whether institutionalization affects social inequalities in NDD mortality.
Materials and Methods
Data
Data were derived from record linkage between the Belgian 2011 census and register information on emigration and mortality for the period October 1, 2011, to December 31, 2016. In a first stage, a link was established between the census and the register data on deaths and emigrations. In a second stage, cause-specific mortality data were added using anonymous individual linkage with death certificates. This database is a unique source of information containing nationwide individually linked data on all-cause and cause-specific mortality, emigration, and background characteristics of all individuals legally residing in Belgium at the time of the 2011 census. The study population comprised all official inhabitants of the country aged 65 years or older during the follow-up period (N=1,883,182). The lowest age limit was set because of the small number of NDD deaths before the age of 65 (N = 805).
Neurodegenerative Disease Mortality
Mortality data included the causes of death issued from the death certificates. The specific NDDs were identified using the tenth revision of the International Classification of Diseases (ICD-10). This study focused on mortality associated with major NDDs including Dementia in Alzheimer disease (F00), Alzheimer disease (G30), Vascular dementia (F01), Parkinson disease (G20), Secondary parkinsonism (G21) and Motor Neuron Disease (G12.2). NDDs are often underreported in death certificates. Therefore, we applied the multiple-cause approach and included all death certificates with any mention of the above outcomes (as an underlying, immediate, intermediate, or additional cause of death).11,26 To eliminate the possibility of bias associated with the multiple-cause approach, we conducted a sensitivity analysis that exclusively considered NDD as the primary cause of death. Although the results from this analysis exhibited reduced statistical significance due to the limited sample size, there were no substantial deviations in the underlying nature of the association. Further details on the sensitivity analysis are available in the Supplemental materials.
Socioeconomic and Sociodemographic Characteristics
SE and sociodemographic (SD) characteristics were measured at the time of the 2011 census, with our analysis assuming a consistent SEP between 2011 and 2016. SEP was measured using educational attainment and income. Educational attainment is based on the highest level of education and is categorized using the International Standard Classification of Education (ISCED): lower secondary education or less (ISCED 0-2, “low”), higher secondary education (ISCED 3-4, “mid”) and tertiary education (ISCED 5-6, “high”). Income is based on net taxable income, recoded into quartiles by sex and age group. Sociodemographic covariates included age, gender and care home residency. Collinearity analyses utilizing Spearman’s rank correlations for both SD and SE variables indicated the absence of problematic multicollinearity. The correlation matrix is provided in the Supplemental materials (S1).
Methods
To obtain a full picture of inequalities in NDD mortality, we calculated both absolute and relative inequalities. First, directly age-standardized (and site-specific) mortality rates (ASMR) were calculated by SEP variable to assess absolute SE inequalities. The Belgian population at the 2011 census was used as the standard population. Second, mortality rate ratios (MRRs) were calculated by SE indicator using Poisson’s regression with the log of the person-time as the offset. Finally, we explored the impact of living in a care home by stratifying the MRRs by care home residency status. All analyses were stratified by sex and age group (65-74 years, 75-84 years, and 85+ years), because different results were observed by sex and age group and conducted separately for the main types of NDDs (dementia, parkinsonism, and MND). All statistical analyses were performed using Stata 17.0 statistics software.
Results
Burden of NDD Mortality in the Study Population
The study population consisted of 1 883 182 people officially residing in Belgium, among whom 34 700 died of an NDD during the 2011 to 2016 study period. Additional demographic characteristics of the study population are presented in Table 1. The highest overall NDD ASMRs were observed in the oldest age group. Specifically, dementia had the highest site-specific mortality rate for both sexes. For instance, in the oldest age group, women had a dementia ASMR of 48‰ (95% CI: 47.2-48.8) compared to 16‰ (95% CI: 15.5-16.5) among men. Regarding parkinsonism ASMRs, it was found that in the youngest age and middle age group, men exhibited higher rates (respectively 0.5‰ (95% CI: 0.4-0.5) and 2.2‰ (95% CI: 2.1-2.4)) than women (0.3‰ (95% CI: 0.2-0.3) and (1.7‰ (95% CI: 1.6-1.8). In the oldest age group, in contrast, women had a higher parkinsonism ASMR (3.6‰ (95% CI: 3.4-3.9)) than men (2.4‰ (95% CI: 2.3-2.6). For MND, ASMRs were largest in the middle age group, but not significantly different between men (0.2‰ (95% CI: 0.2-0.2)) and women (0.2‰ (95% CI: 0.1-0.2)))).
Age-Standardized Mortality Rates (‰), Men and Women Aged 65 to 74, 75 to 84, and 85 or Older, Belgium 2011 to 2016.

Source. Belgian 2011 census linked to National Population Register (2011-2016).
Note. PY = person years; N = number of deaths; ASMR = age-standardized mortality rates per 1000.
Directly standardized to the sex-specific Belgian population in 2011.
Absolute Inequalities in NDD Associated Mortality
Table 2 presents the ASMRs by SEP indicator for men and women across different age groups. Educational attainment and income both showed a negative correlation with NDD mortality rates, with the most significant disparities observed in educational attainment. Among the oldest men, those with low education had an NDD ASMR of 42.2‰ (95% CI: 40.7-43.7), while men with high education had an NDD ASMR of 7.7‰ (95% CI: 7.7-8.4), resulting in an absolute difference of 34.7‰. For women, the disparities were even more pronounced, with an absolute difference of 51.7‰ between the oldest women with low education (55.7‰ (95% CI: 54.6-56.9) and high education (4‰ (95% CI: 3.7-4.3).
Age-Standardized Mortality Rates (‰), Men and Women Aged 65 to 74, 75 to 84 and 85 and Older, by Education and Income, Belgium 2011 to 2016.

Source. Belgian 2011 census linked to National Population Register (2011-2016).
Note. PY = person years; N = number of deaths; ASMR = age-standardized mortality rates per 1000.
Directly standardized to the sex-specific Belgian population in 2011.
Regarding income, we consistently observed the lowest ASMRs in the highest income quartile, but the gradient was not outspoken. The most significant disparities were observed in the youngest age group. Men in the lowest income quartile had an NDD ASMR of 1.9‰ (95% CI: 1.8-2.0), while men in the highest income quartile had an NDD ASMR of 0.3‰ (95% CI: 0.3-0.4), resulting in an absolute difference of 1.6‰. The youngest women showed an absolute difference of 0.7‰ between the lowest (1‰ (95% CI: 0.9-1.1) and the highest income quartile (0.3‰ (95% CI: 0.2-0.3).
By NDD subtype, we observed the same patterns for dementia and parkinsonism as for NDDs in general, with a negative association between mortality and both educational attainment and income. For MND, we found a negative association between mortality and educational attainment, but no association with income.
Relative Inequalities in NDD Associated Mortality
Table 3 presents the results of the Poisson regressions, confirming the presence of relative inequalities by SEP in NDD mortality. Educational attainment was strongly negatively associated with NDD mortality in women, particularly in the youngest age-group where mortality was 1.37 (95% CI: 1.11-1.70) times higher in the low education group compared to the highest. In men, a significant association with education was observed in the middle age group only, with mortality being 1.11 (95% CI: 1.01-1.21) times higher in the low education group compared to the highest. Income had the strongest negative association in the youngest men, where mortality was 1.57 (95% CI: 1.26-1.88) times higher in the lowest income quartile compared to the highest. However, the association with income was not significant in the oldest men, and no clear gradient of NDD mortality by income was observed in women.
Relative NDD Mortality Inequality (MRRs and 95% CI) by Education and Income, Men and Women Aged 65 to 74, 75 to 84 and 85 and Older, Belgium 2011 to 2016.

Note. Reference categories are high educational attainment and highest income quartile.
All analyses are adjusted for attained age, All results significant at the p < .05-level are in bold.
Source. Belgian 2011 census linked to National Population Register (2011-2016).
When comparing inequalities between NDDs, we found that dementia mortality had the largest disparities. Education was found to have a stronger negative association with dementia mortality compared to total NDD mortality, and the association remained significant even in the oldest age group. The association between income and dementia followed the same trend as for total NDD mortality. For parkinsonism, in contrast, we observed a reversed pattern with education. The oldest men with low education had 0.73 (95% CI 0.57-0.94) times lower parkinsonism mortality compared to men with high education, and women with low education had 0.74 (95% CI 0.59-0.93) times lower parkinsonism mortality compared to women with high education in the middle age group. Income only showed an association with parkinsonism mortality in the youngest men, where mortality was 1.61 (95% CI 1.11-2.34) times higher in the lowest income quartile compared to the highest. Lastly, we did not observe a significant association between SEP and MND mortality.
Stratification by Care Home Residency
During the study period (2011-2016), a total of 22 375 men (2.9%) and 99 534 women (9.9%) aged 65 years or older were residing in care facilities in Belgium, as presented in Table 4. The proportion of care home residents increased with age and was higher in women than in men. Specifically, in the youngest age group, 1.2% of men (N = 5067) and 1.5% of women (N = 7163) were care home residents, compared to 3.2% of men (N = 8651) and 6.9% of women (N = 26 914) in the middle age group and 13.2% of men (N = 8657) and 33.2% of women (N = 43 424) in the oldest age group.
Age-Standardized Mortality Rates (‰), Men and Women Aged 65 to 74, 75 to 84, and 85 or Older by Care Home Residency, Belgium 2011 to 2016.
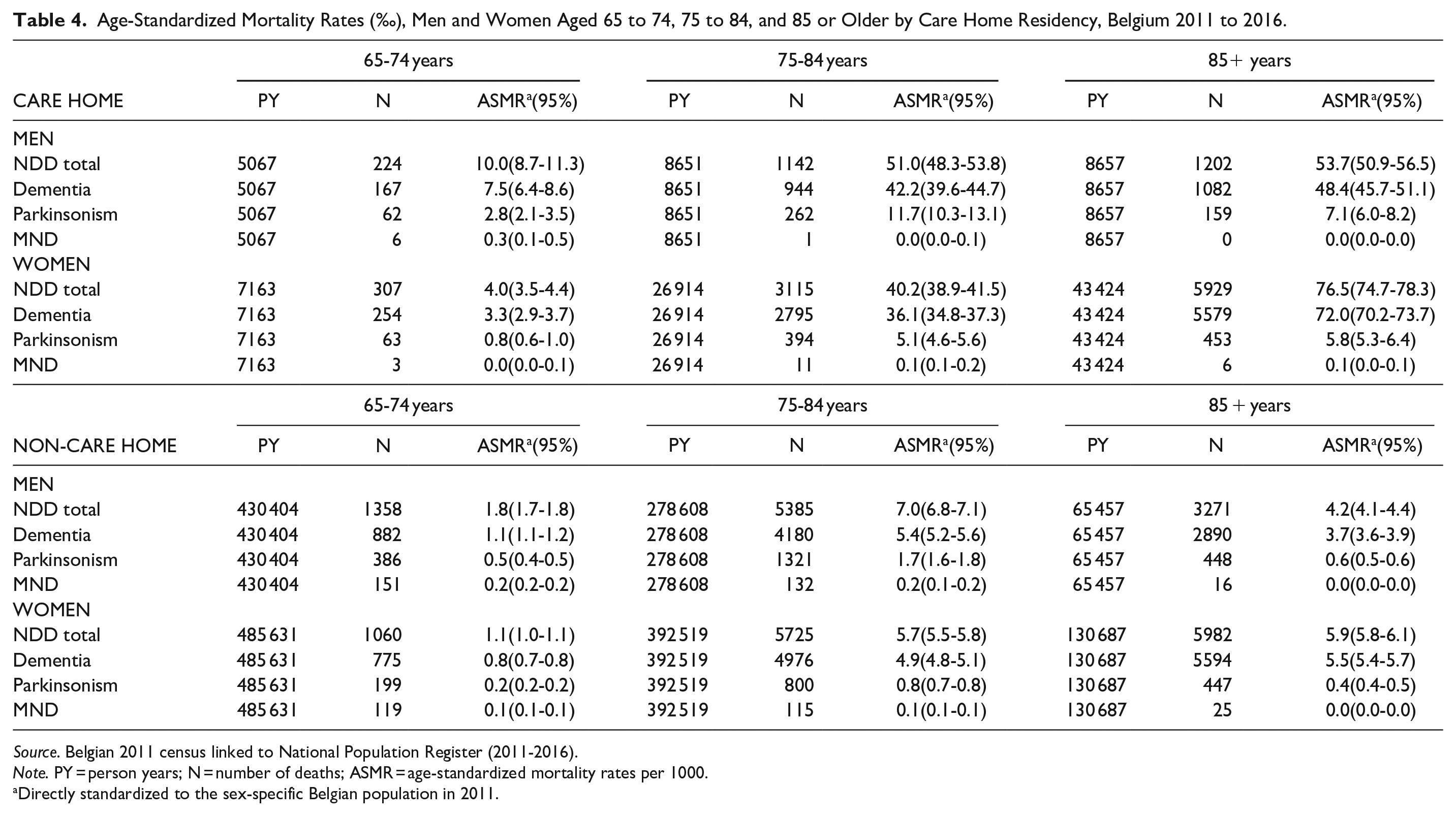
Source. Belgian 2011 census linked to National Population Register (2011-2016).
Note. PY = person years; N = number of deaths; ASMR = age-standardized mortality rates per 1000.
Directly standardized to the sex-specific Belgian population in 2011.
Table 4 shows that care home residents had higher ASMRs for NDDs compared to those living independently. In the oldest age group, care home residents had an NDD ASMR of 53.7‰ (95% CI: 50.9-56.5) for men and 76.5‰ (95% CI: 74.7-78.3) for women, resulting in an absolute difference of 49.5‰ for men and 70.6‰ for women between individuals living at home, where the NDD ASMR was 4.2‰ (95% CI: 4.1-4.4) for men and 5.9‰ (95% CI: 5.8-6.1) for women. It is worth noting that due to the small number of MND deaths in care home residents (N = 27), we did not include MND in the stratified analyses.
In Table 5, we present the MRRs of the stratified the analysis by care home residency. We found that education had a stronger negative relationship with NDD mortality in care home residents than in individuals living at home. For instance, in the youngest women in a care facility, dementia mortality was 2.13 (95% CI: 1.55-3.38) times higher in the low education group compared to the highest education group. In contrast, in women from the same age group living at home, the MRR was 1.34 (95% CI: 1.05-1.71). Furthermore, parkinsonism mortality showed a negative association with education in the population living in a care home, but a positive association in the population living at home.
Relative NDD mortality inequality (MRR and 95% CI) by SEP Indicators, Men and Women Aged 65 and Older, Stratified by Care Home Residency, Belgium 2011 to 2016.
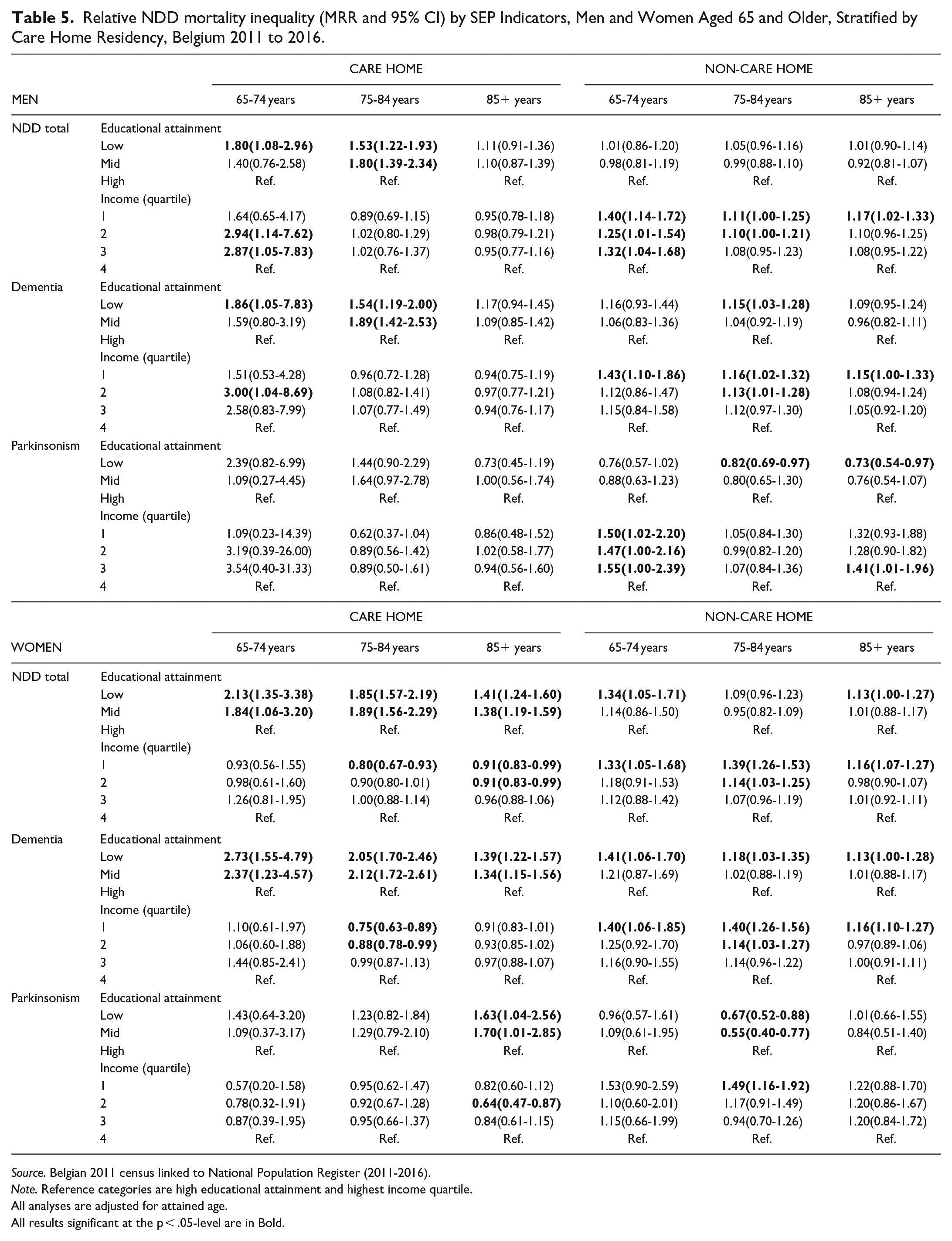
Source. Belgian 2011 census linked to National Population Register (2011-2016).
Note. Reference categories are high educational attainment and highest income quartile.
All analyses are adjusted for attained age.
All results significant at the p < .05-level are in Bold.
Conversely, income had a strong negative association with NDD mortality in the population living at home, whereas no significant association was observed in the population residing in a care facility. For instance, men in the youngest age group living at home had 1.50 (95% CI: 1.02-2.20) times higher parkinsonism mortality in the lowest income quartile compared to the highest, while no significant association was found in the same group residing in a care facility.
Discussion
Our study aimed to investigate the association between different dimensions of SEP and NDD associated mortality. To our knowledge, this is the first large-scale study that digs into the association between SEP and mortality of multiple NDDs. The findings showed a strong negative association between SEP - measured by educational attainment and income - and mortality related to dementia. Income showed a strong negative association with parkinsonism mortality, but only in youngest men. Conversely, we observed some reversed patterns for parkinsonism mortality with educational attainment. We did not find any significant correlation between MND mortality and SEP. When stratifying the analysis by care home residency, we found that educational differences in NDD mortality were stronger among care home residents, while income generated larger disparities in the population living at home, whereas differences were absent in the population living in a care facility.
Our results support previous findings of higher dementia mortality in individuals with low educational attainment.11-17 The cognitive reserve hypothesis is the most popular discourse to explain this relationship. 27 The hypothesis claims that higher education enhances brain health and protects against neurodegeneration. 11 We found a stronger negative association between education and dementia mortality in women compared to men. This gender disparity could be explained by women from older generations having had fewer opportunities for education and intellectual stimulation than men, leading to lower levels of cognitive reserve 28 and a stronger negative association between education and dementia mortality. 13
Additionally, our results align with previous findings showing that the risk of dying from dementia is higher in deprived income deciles.7,10,11 Various factors may explain this relationship, including barriers in access to lifelong learning/cognitive training, poor nutrition, poor management of cardiovascular risk factors (such as diabetes, obesity, and smoking), and stress.29,30 Furthermore, income showed a stronger association with dementia mortality in men, possibly due to traditional gender roles in older generations where women were more reliant on their husband’s income. This could imply that income is a less discriminatory indicator of SEP in women. Lastly, we found that the association between income and dementia mortality disappeared in the oldest age group. The dominant hypothesis to explain a diminishing relationship between income and mortality in advanced old age is the “age-as-leveler” hypothesis. This concept suggest that age suppresses the accumulated advantages from income through 3 proposed mechanisms: biological processes, such as frailty and health problems, that override the accumulated social advantages; social processes, such as reliance on pension schemes, that generate inequality; and a mortality pattern influenced by social factors (selective mortality). 31
Regarding parkinsonism mortality, our study only partially supports previous research that links SEP to parkinsonism mortality.18,19 Specifically, we found a negative association between income and parkinsonism mortality in men from the youngest age group only. The relationship between education and parkinsonism mortality has not been investigated previously, but our results are consistent with previous research on PD prevalence and incidence which suggest a positive relationship between education and PD risk.20,21 A hypothesis to explain this positive relation is that higher educated people have greater medical awareness and access to specialized care, 20 resulting in better diagnosis rates. PD is challenging to diagnose, and patients who seek care from specialized neurologists may have higher diagnosis rates than those who receive care from primary care physicians. 32 Differences in NDD diagnosis might also be projected in mortality rates, as SE biases in mortality reporting could lead to differential reporting on death certificates. 33
For MND mortality, we did not find a significant relationship with SEP, consistent with research on MND risk in Scotland. 23 Clouston et al (2016) provided an interesting framework which can help explain why we observed lower SE disparities in MND, and parkinsonism compared to dementia mortality. Their extended fundamental cause theory (FCT) characterizes 4 stages of disease: natural mortality, producing inequalities, reducing inequalities and reduced mortality. 34 MNDs are rare, and little is known about their risk factors, prevention, or treatment, explaining why there is no clear association between MND mortality and SEP, as the disease is still in its natural mortality stage. During the second stage, populations found the capacity to reduce the mortality burden of a disease. As FCT suggests, people with a high SEP will gain access to new preventions and treatments because they embody access to resources, resulting in mortality inequalities. 35 When health-beneficial innovations become more universal, social inequalities decrease (stage 3) and finally disappear (stage 4). This framework provides an interesting perspective that could explain the observed differences in disparities between NDDs, and future analyses on SE inequalities in mortality from these diseases will shed light on the validity of this theory in NDDs.
When stratifying the analysis by living situation, we observed differences between care home residents and individuals living at home. Specifically, education had a stronger negative association with NDD mortality among care home residents, whereas income showed no significant association among this group. Although a recent study found that low-income and low-educated individuals are more likely to live in a care home, 36 the availability of healthcare resources and access to quality healthcare may be more equitable within care home settings compared to independent living. Care homes typically provide standardized access to healthcare services, irrespective of income levels. This uniform access to healthcare may help mitigate the disparities in NDD mortality by income among care home residents. On the other hand, educational disparities may persist within care homes, as the benefits of higher educational attainment in health literacy and cognitive reserve remain relevant even in this setting. However, limited research is available on SE disparities in care home residents’ mortality, which highlights the need for further investigation in this area.
Strengths and Limitations
Strengths of our study include the large population-based dataset which covers the entire population in Belgium, enhancing the generalizability of the results. This also provided sufficient power to allow gender- and age-specific analyses and a series of explanatory factors. Moreover, we were able to perform sub-analyses by type of NDD. The population-based design minimizes selection bias, particularly important when investigating a variable such as SEP. By including 2 indicators of SEP, we respected the complexity of the construct which ideally should not be measured with a single indicator. 37
This notwithstanding, the study has some limitations. First, the Belgian long-term care system prioritizes enabling individuals to reside in their own homes for as long as possible. The eligibility for residential care is determined by assessing individuals based on the 0 to 7 Activities of daily living (ADL) or Katz-scale, supplemented with a mental criterion (disorientation in time or space). 38 Consequently, it is anticipated that the prevalence of NDDs would be higher among the care home population. This heightened prevalence could, to some extent, account for the observed disparities in mortality by SEP.
Second, a limitation of our dataset is the lack of data on individual risk factors such as behavioral and healthcare factors, limiting the possibility to examine specific pathways between SEP and NDD mortality. Moreover, we were unable to distinguish NDD incidence and survival as there is no Belgian population-based registry for NDDs. Population-based registers are utterly required to provide high-quality longitudinal data on the whole neurodegenerative spectrum, enabling comparative analysis. The lack of population-based registers for NDDs is a recognized issue worldwide. 39
Conclusion
In conclusion, our study provides compelling evidence supporting the presence of SE disparities in mortality due to neurodegeneration. We observed a strong negative association between SEP - measured by educational attainment and income - and dementia mortality. This finding highlights the importance of SE factors in shaping NDD mortality outcomes. Surprisingly, we found a contrasting pattern for parkinsonism mortality, where individuals with low educational attainment exhibited lower mortality rates. We did not identify a significant correlation between MND mortality and SEP.
To gain a deeper understanding of these SE disparities, future studies should focus on further investigating and explaining the underlying mechanisms contributing to these associations. Such studies will play a pivotal role in identifying and implementing effective interventions and policies aimed at mitigating these inequalities. By doing so, we can ultimately enhance the quality of life for individuals affected by NDDs.
Moreover, it is of utmost importance to raise awareness about SE disparities in the disproportionate mortality of NDDs. Effectively addressing these disparities requires the adoption of an interprofessional approach 29 that integrates various disciplines and capitalizes on global opportunities to promote brain health. This approach should prioritize gaining an understanding of health disparities and implementing strategies aimed at rectifying inequities. By actively addressing these disparities and implementing appropriate measures, we can strive for a more equitable and healthy aging society.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241237113 – Supplemental material for Socioeconomic Disparities in Neurodegenerative Disease Mortality: A Population-Based Study among Belgian Men and Women Aged 65 or Older
Supplemental material, sj-docx-1-inq-10.1177_00469580241237113 for Socioeconomic Disparities in Neurodegenerative Disease Mortality: A Population-Based Study among Belgian Men and Women Aged 65 or Older by Janna Dinneweth and Sylvie Gadeyne in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
N/A
Data Availability Statement
The data that support the findings of this study includes identifying information on participants and was used under license for the current study, and hence not publicly available. Data codebooks and syntaxes used for the statistical analyses are available from the authors upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by the Research Foundation – Flanders (FWO) and Fonds National de la Recherce Scientifique (FNRS) under the Excellence of Science (EOS) program [project number 40007537].
Ethical Statement
No ethical approval was required for this research, as it involved no direct interaction with human subjects or the collection of new data. The use of existing data was conducted in accordance with the terms specified in the license agreement, prioritizing privacy, confidentiality, and respect for the original data sources
Informed Consent/Patient Consent
N/A
Trial Registration Number/Date
N/A
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.