
Abstract
Within a few years, 1 in 6 people will be aged 60 years or older. Extreme situations, such as the COVID-19 crisis, constitute a challenge to older adults. However, the literature on the daily functional characteristics of older adults in the past and during the COVID-19 crisis and their relationships to their physical and mental health is scarce. This study aimed to examine the past and present daily functional factors associated with physical and mental health in older adults. Using an online platform, 204 Israelis aged 60 years and older reported their physical health symptoms and anxiety levels. They completed questionnaires about past (negative life events and childhood daily functional self-actualization) and present (adulthood daily functional self-actualization, functional cognition and sleep quality) factors. Structural equation modeling revealed correlations between functional cognition and childhood daily functional self-actualization (β = −.18) and anxiety (β = .15); adulthood daily functional self-actualization and past negative life events (β = −.18), anxiety (β = −.50), and physical symptoms (β = −16); and sleep quality and past childhood daily functional self-actualization (β = −.19), negative life events (β = .22), anxiety (β = .18), and physical symptoms (β = .40). These findings shed light on potential functional factors for older adults’ health, indicating that these functional factors play a vital role in reducing health problems in later life.
Keywords
Introduction
According to the World Health Organization, 1 the proportion of adults aged 60 years or more is expected to nearly double—from 12% to 22% of the global population—by 2050. Aging, a natural process associated with biological, psychological and social changes, increases the risk of mental and physical decline. 1 Thus, the literature gives great attention to physical and mental health as factors important to integrating older adults’ overall health.1,2
The older adult population, especially those already at risk for physical and mental decline, found the extensive COVID-19 lockdowns challenging.3,4 Older adults commonly experience physical health symptoms, such as headaches or back pains.5,6 In times of crisis, these symptoms may appear more frequently,7,8 and older adults may experience increased state anxiety, an emotional reaction to a potentially dangerous situation.8,9
Previous studies indicated that self-reported physical symptoms might signal severe illness and predict mortality. 6 For example, Petrie et al 10 reported that back and chest pain, common in older adults, predicted hospitalization and mortality among primary-care patients. 6 Thus, in our study, physical health is measured by the existence and frequency of physical symptoms. Similarly, as found in prior research, the most widespread mental disorders among older adults are anxiety disorders (eg, Petkus et al 5 ). Therefore, our study assesses mental health by participants’ state anxiety levels.
Numerous studies have highlighted various factors affecting mental and physical health among older adults during the COVID-19 pandemic. For instance, the literature associated present factors, such as cognitive functioning, with COVID-19’s health implications, 10 showing improved cognitive abilities among healthy older adults. 11 Conversely, a link between physical impairments and cognitive decline was identified in frail older adults. 12 Furthermore, studies showed that the pandemic influenced the sleep patterns of older adult residents in Hong Kong, leading to increased sleep duration but decreased quality of life. 13 Recent research also explored the impact of daily functional activities, like returning to work and engaging in spiritual, physical, and social activities, on physical and mental health and overall quality of life.14 -17
However, the current literature does not comprehensively cover daily functional characteristics and their intricate connections to physical and mental health among older adults during crisis periods. Specifically, only scarce research addressed daily functional aspects that influence health within this context, such as self-actualization or functional cognition. 21 Comprehending older adults’ past and present circumstances offers invaluable insights into resources pivotal to promoting their overall health. Therefore, this study aimed to examine the past and present daily functional characteristics associated with physical and mental health risks among older adults.
Understanding Physical and Mental Health Through the Embodied Cognition Theory
The theoretical framework of embodied cognition suggests that sensorimotor factors are fundamental to forming cognition. 18 This perspective implies that past experiences, even those from childhood, significantly shape how people perceive the world and navigate their functioning within it. It views the mind and body as an integrated whole, acknowledging their reciprocal influence on each other. Because declining physical and cognitive abilities often accompany aging, this theory provides a framework for understanding complex past and present daily functional characteristics. 19
In line with this theoretical lens and the previous literature, we identified several past and present factors that may have influenced older adults’ physical and mental health during the COVID-19 crisis. A previous study examined gender differences in daily functional self-actualization and functional cognition as a factor associated with state anxiety. 32 It provided evidence that these factors differed between genders during the COVID-19 pandemic. Thus, to better understand physical and mental health among the older adult population, our study enhances the dimensions with past and present factors. For past factors, we focus on life events and childhood self-actualization; for present factors, we examine daily functional self-actualization, cognition and sleep quality.
Past daily functional characteristics
According to the embodied cognition theory, 19 life events and memories result from experiences throughout life. People can experience life events as negative or positive. Events considered negative pose risks to physiological responses and affect the individual’s health and self-esteem. 20 Events that trigger negative feelings—such as unemployment, divorce, or the death of a relative—can lead to reduced participation in daily activities. Therefore, past negative (stressful) life events have been associated with mental health implications—specifically, depression in later life. 21
However, life events viewed as positive can promote self-actualization, one’s motivation and active pursuit of self-fulfilment. 22 Positive childhood experiences have been linked to better performance in cognitive assessments of older adults’ central executive functioning and verbal recall. 12 Being self-actualized involves growing and advancing rather than remaining static. In other words, self-actualization is the search for meaning and purpose in life and being fully functional. 23
Self-actualization has been mentioned as a factor contributing to the well-being of individuals during the COVID-19 pandemic. 23 The functional self-actualization concept was developed during the pandemic period based on Maslow’s 24 self-actualization theory and the WHO’s International Classification of Functioning, Disability and Health (ICF). 21 The concept incorporates daily functional abilities, which are related to physical and psychological risks and can enhance feelings of control and health. 32 Thus, the term functional self-actualization includes components like environmental resources, health, daily doing/work satisfaction, mood, self-fulfilment, and life control.
Present daily functional characteristics
This study refers to past (childhood) and present (daily) functional self-actualization. Both share a similar theoretical structure, but the former focuses on the past, whereas the latter focuses on the present. Recent research indicated a correlation between functional self-actualization and state anxiety and a relationship between functional cognition and anxiety during the COVID-19 pandemic. 32
Functional cognition is the cognitive abilities (eg, executive function, memory and monitoring) required to perform everyday tasks and complex activities. This concept involves the individual’s capacity to perform tasks and emphasizes overall abilities, such as habits, routines and environmental resources. 28 In age-related changes, older adults as a whole experience cognitive decline; however, the pandemic may have accelerated this process. 23 Thus, this study also encompasses functional cognition to shed light on functional features.
A person’s quality sleep can also be considered a risk factor in how well an individual performs daily tasks. 26 For example, low sleep quality has been associated with anxiety and cognitive decline among older adults. 27 Despite its importance, the definition of subjective sleep quality is not well known. The Pittsburgh Sleep Quality Index (PSQI) has been widely used to gauge subjective sleep quality.25,26 In recent studies using this assessment, researchers reported that the COVID-19 pandemic caused sleep disturbances in older adults, likely due to increased stress. 28 Whether from personal or natural causes, these events may accelerate sleep disturbances, especially among older adults, who already experience changing sleep patterns due to aging. 29 However, regardless of the pandemic, more than half of older adults report sleep disturbances due to age-related changes in their sleep construct, including slower wave sleep, advanced circadian rhythms and early awakening. 30
These present and past functional factors appear to be interconnected in contributing to an individual’s health. 19 Although the literature gave certain aspects of these factors attention during the COVID-19 era, their precise relationships and predictive influences on physical and mental health remain unclear. Therefore, the aim of our study was to examine past (life events and childhood self-actualization) and present (daily functional self-actualization, functional cognition and sleep quality) functional factors related to physical and mental health risks. Figure 1 illustrates a proposed model based on previous studies and the embodied cognition theory 19 ; arrows indicate the hypothesis.

A proposal model for predicting state anxiety and physical health symptoms.
Methods
Participants and Procedure
Ethical approval (No. 190/20) was received from the University of Haifa Faculty Ethics Committee. The sample comprised 204 Israeli individuals aged 60 years and older living in the community and capable of independently completing online questionnaires. Data collection occurred during 2 months of the COVID-19 lockdown (from 20 September to 10 October 2020) using an Israeli survey company, Panel4, which has access to tens of thousands of panel members representing the adult population in Israel. The participants were a random sample of those who had registered as panellists. Before initiating the study, we sent prospective participants a Qualtrics web link containing written informed consent to confirm their participation in the study. After signing their consent, participants anonymously and independently completed the following assessments:
Demographic questionnaire
Questions about physical health symptoms
State-Trait Personality Inventory (STPI) 31
Questions related to negative life events
Childhood Daily Functional Self-Actualization Questionnaire for Adults (C.DailyFA)
Daily Functional Self-Actualization Questionnaire for Adults (DailyFA) 32
Daily Living Questionnaire (DLQ) 33
Pittsburgh Sleep Quality Index (PSQI) 34
Data Analysis
Sample size calculation
Power analysis was conducted to determine the sample size at 80% power with an 0.15 effect size and a .05 significance level. The power analysis for 2 phases and 5 predictors equaled 68. Because the study included 2 dependent variables, the required sample size was 136, exceeded the calculated minimum requirement.
We used descriptive statistics to describe the sample and questionnaire results, and the structural equation modeling (SEM) AMOS 25 program for analysis and examination. Three criteria were considered in evaluating the model’s goodness-of-fit: chi-square estimator (χ), comparative fitted index and Steiger’s root mean square error of approximation. According to Weston and Gore 43 a nonsignificant χ would indicate that the model fit the data well. However, large samples frequently induce significant χ because of the increased power. Thus, comparative fit index values should be at least 0.90 (values closer to 1.0 indicate a better fit), and the root mean square error of approximation should be equal to or less than .08. 35
Instruments
Most Common Physical Health Symptoms Scale
Participants rated how much they suffered the symptoms of stomach-, back-, head- or chest ache and vertigo on a Likert scale of 1 (not at all), 2 (seldom), 3 (sometimes), 4 (largely), and 5 (too largely). These items were chosen based on previous research indicating that such symptoms are common among older adults. 10 Internal consistency in this study was acceptable (α = .76). The mean score of the entire sample for each item was calculated.
State-Trait Personality Inventory
We used the STPI to measure state and trait levels of subjective emotions, such as anger, depression, curiosity and anxiety (referred to as state anxiety), comprising 10 items in this study. Participants rate how they presently feel on a 4-point Likert-type scale from 1 (not at all) to 4 (very much so); higher scores indicate greater state anxiety. 31 This questionnaire has displayed high internal consistency and good reliability and validity among community-dwelling older adults. The Hebrew version was also found to be reliable and valid. 36 Internal consistency was acceptable in this study (α = .71).
Past daily functional characteristics
Negative Life Events Scale
Participants completed a Hebrew checklist designed for this study with 15 negative life events. A further open question was included in the original scale, which asked participants to describe any further events that occurred. Due to the lack of important information obtained from this question, we did not include it in the calculation of the overall score. These events were chosen based on events noted in the literature, such as the death of a relative, divorce, financial crisis and severe disease (eg, Wilson 19 ). Participants responded yes or no to whether they had experienced any of the items and reported the total number of negative life events experienced.
Childhood daily functional self-actualization questionnaire for adults
The C.DailyFA was designed for this study to evaluate perceived childhood functional self-actualization. The questionnaire was developed parallel to the urgency of the COVID-19 crisis period to examine health-related issues. The items were chosen based on Maslow’s self-actualization theory 24 and the ICF. 21 We established content and face validity according to the literature on self-actualization. Four occupational therapy researchers participated in the expert validation process, certifying that the items encompassed the construct of daily functional self-actualization. Participants rated their feelings about their childhood functioning—manifested by aspects such as mood, relationship, expression of abilities, support and happy childhood—on a 10-point scale from 1 (very false) to 10 (very true). We used the items’ overall average scores and established the questionnaire’s content and face validity with high (α = .92) internal consistency in this study.
Present daily functional characteristics
Daily functional self-actualization questionnaire for adults
The DailyFA 32 is a 10-item scale measuring present daily functional self-actualization. As part of the current study, the Hebrew version was used. Its items cover the themes of environmental resources, health, daily doing/work satisfaction, mood, self-fulfilment and life control. Participants rate their feelings or satisfaction with those items on a 10-point scale from 1 (not good at all) to 10 (very good). We computed a mean score for the items. The questionnaire’s content and face validity have been established 32 and showed high (α = .94) internal consistency in this study.
Daily Living Questionnaire
The DLQ 33 is a functional cognition scale assessing everyday difficulties in activities and participation tied with higher level cognitive deficiency. Participants rate their levels of mental or cognitive difficulty when performing 52 daily activities on a four-point Likert-type scale from 1 (no mental or cognitive difficulty) to 4 (unable to complete). The first domain, Part A (28 items), relates to activities and participation and consists of 4 factors: household tasks, activities involving language and comprehension, community/participation and complex tasks. The second domain, Part B (24 items), relates to cognitive symptoms or impairments. It consists of 3 factors: executive functions, memory and executive function monitoring. Outcome measures are the mean scores of each part (A and B) and each factor. The DLQ’s content and face validity have been established and found to have acceptable internal consistency for both parts. 33 Internal consistency in the current study was high for all 52 items (α = .94) and for each part separately (Part A, α = .87; Part B, α = .94).
Pittsburgh Sleep Quality Index
The PSQI 34 assesses sleep quality and disturbances that may have affected participants’ sleep quality in the past month. It consists of 18 items divided into 7 components (eg, sleep quality, sleep latency, sleep duration and habitual sleep efficiency), with scores ranging from 0 to 3. A summary score is calculated for each component; the 7 component scores are summed to the global PSQI score (range 0-21). Higher scores indicate lower sleep quality. The PSQI’s validity and reliability have been established. 34 In this study, internal consistency values of all components were acceptable (α = .75).
Findings
Sociodemographic Characteristics
The sample comprised 204 Israeli adults (102 women and 102 men) aged 60 years or older (M = 69.14 years, SD = 5.95, range 60-88). Most participants lived in a city (87.3%) and spoke Hebrew (93.1%). More than half were married and retired, and most had at least 12 years of education (M = 13.62, SD = 4.31), indicating high school completion. Table 1 displays additional demographic characteristics.
Sociodemographic Characteristics.
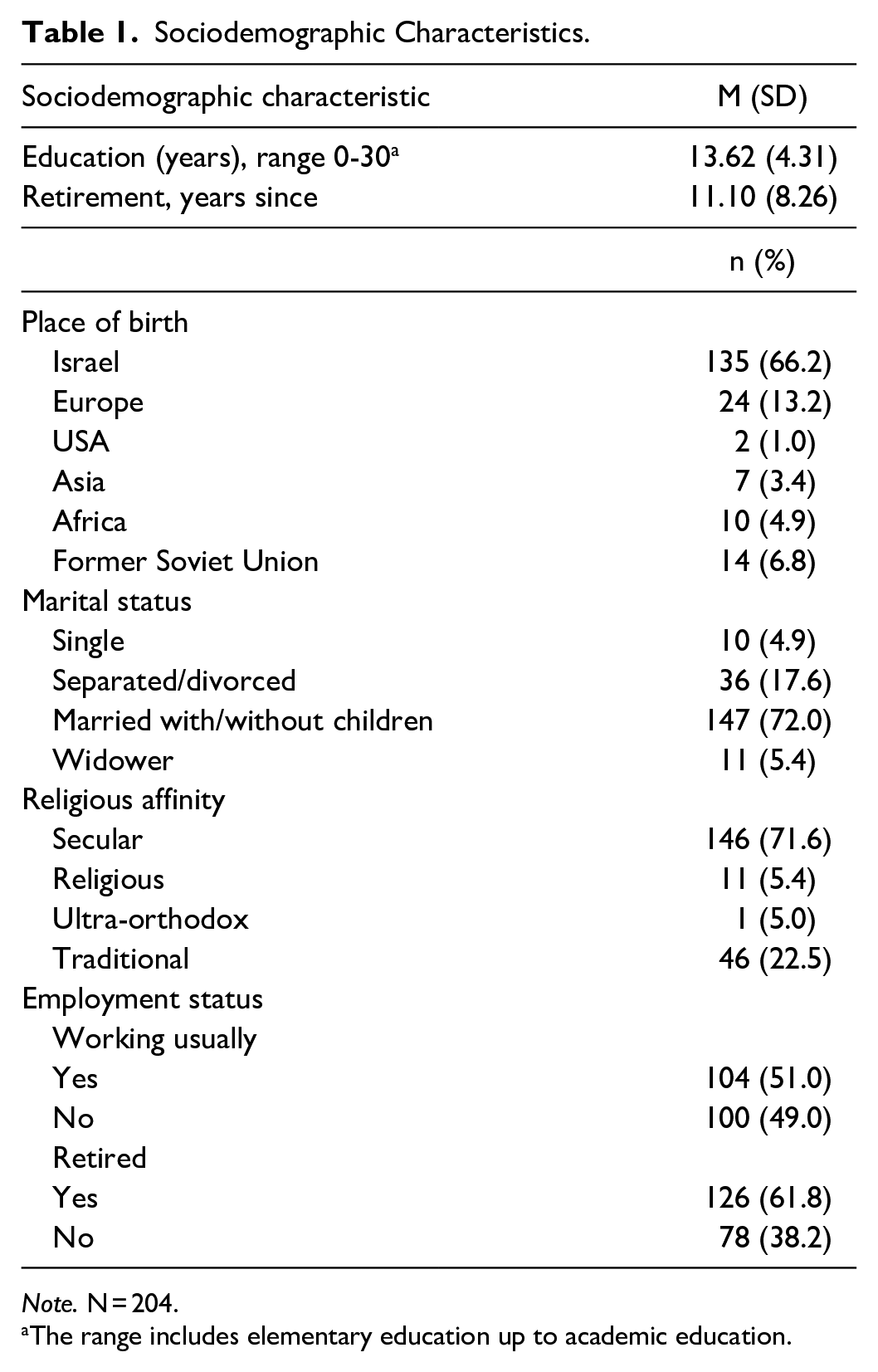
Note. N = 204.
The range includes elementary education up to academic education.
Most Common Physical Health Symptoms
The total mean score for items grading the frequency of physical health symptoms was 1.75 (SD = 0.65), falling between 1 (not at all) and 2 (seldom). Backache appeared in the highest frequency (M = 2.33, SD = 1.10), then headache (M = 1.90, SD = 0.95), vertigo (M = 1.59, SD = 0.88), stomach ache (M = 1.56, SD = 0.89), and chest ache (M = 1.41, SD = 0.71).
State Anxiety
The STPI state anxiety mean score was 23.44 (SD = 7.24), ranging between 10 and 40. According to these findings, all participants experienced some level of anxiety during the COVID-19 period.
Past Daily Functional Characteristics
Negative life events
The mean score for the number of negative life events the participants experienced was 5.96 (SD = 2.84). More than 25% of participants experienced neighborhood (25.2%), family (28.6%) or workplace (29.1%) conflict, and most experienced unsuitable work hours (50%), retirement (54.9%), illness (74.8%), or death of a loved one (94.2%).
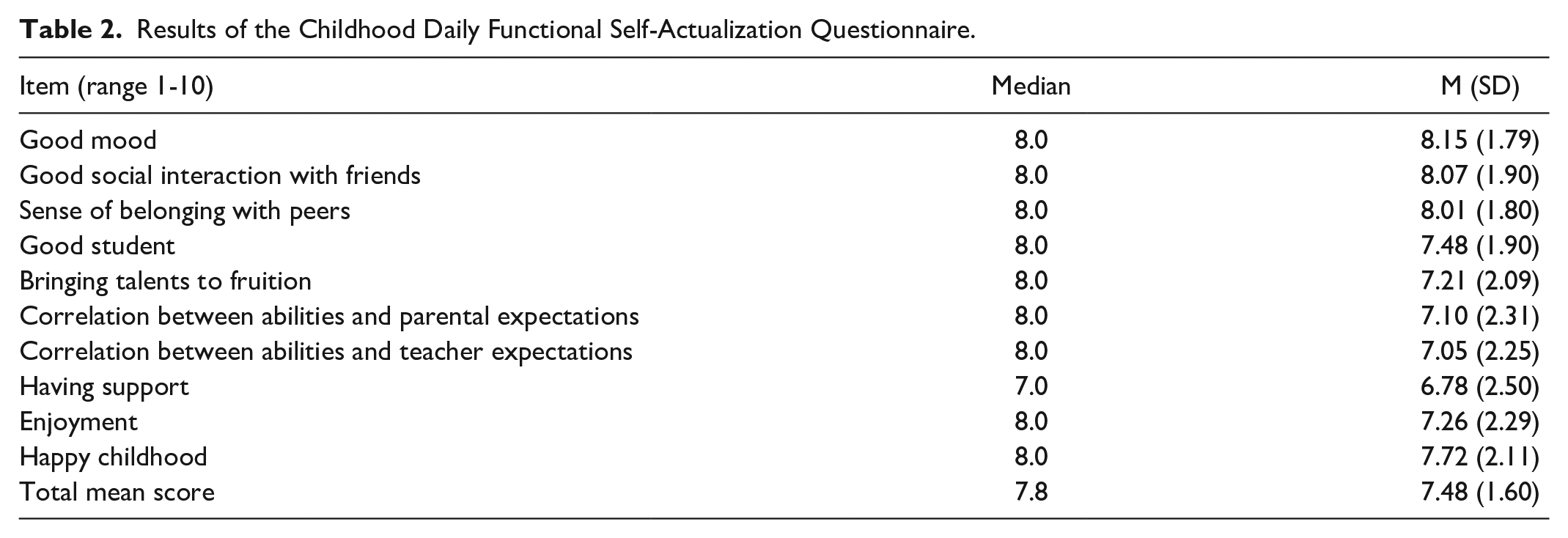
Childhood daily functional self-actualization
The C.DailyFA score medians, means and standard deviations illustrated the variations for each item (Table 2). According to the mean item scores, which ranged from 6.78 to 8.15 (SD = 1.6-2.5), participants felt a sense of self-actualization during childhood.
Results of the Childhood Daily Functional Self-Actualization Questionnaire.
Present Daily Functional Characteristics
Daily functional self-actualization
Table 3 presents the DailyFA score medians, means and standard deviations. Across all items, mean scores ranged between 5.47 and 7.41, which were lower than the reported childhood scores. Variability was exhibited within each DailyFA item and between participants, as reflected by the standard deviation range (1.97-2.75).
Results of the Daily Functional Actualization (Adult) Questionnaire.

Functional cognition (DLQ)
The mean score of the DLQ Part A (activities and participation) was 1.55 (SD = 0.50), and of Part B (cognitive symptoms that might be interfering) was 1.3 (SD = 0.51). In Part B, the mean domain score for executive functions was 1.54 (SD = 0.57), for memory was 1.47 (SD = 0.56) and for executive function monitoring was 1.39 (SD = 0.49). Based on these mean scores, participants reported some cognitive difficulty performing daily activities.
Sleep quality (PSQI)
The global PSQI mean score was 5.80 (SD = 3.47), indicating that participants experienced some sleep difficulties. The results for each PSQI component ranged between 0.33 (SD = 0.62) and 1.33 (SD = 0.66).
Structural Equation Modelling Analysis
Figure 2 presents the SEM results demonstrating the regression coefficients, and Figure 3. shows the correlations between 2 study variables. Based on the analysis guidelines, we illustrated the observed (dependent) variables in the figures as rectangles. Single-headed (unidirectional) arrows represent regression coefficients; double-headed arrows represent correlations between 2 variables.37,38 Overall, the results indicate significant correlations between past and present functional factors, physical health symptoms and anxiety. The squared multiple correlations for physical health symptoms and anxiety as a reflection of mental health were 0.47 and 0.37, respectively.

Structural equation modeling for physical health symptoms and state anxiety.

Correlation between 2 study variables.
Further, present functional factors were found to mediate between past functional factors and physical health symptoms and anxiety. The direct and indirect effects that occurred when other variables (cognitive symptoms or impairments, daily functional self-actualization or sleep quality) mediated a relationship between variables were significant. The exception was the indirect effect between childhood and adulthood daily functional self-actualization, which was not significant (represented by a broken line in Figure 2).
Sleep quality was shown to mediate the relationship between negative life events and state anxiety [95% CI (LB 0.03, UB 0.23; P < .05)] and between negative life events and physical health symptoms [95% CI (LB 0.01, UB 0.04; P < .05)]. Furthermore, sleep quality mediated between childhood daily functional self-actualization and state anxiety [95% CI (LB −.4.6, UB −0.3; P < .05)] and between childhood daily functional self-actualization and physical health symptoms [95% CI (LB −0.07, UB −0.00; P < .05)].
Daily functional self-actualization was found to mediate the relationship between negative events and state anxiety [95% CI (LB 0.08, UB 0.46; P < .05)] and between negative life events and physical health symptoms [95% CI (LB 0.00, UB 0.16; P < .05)]. Finally, cognitive symptoms or impairments (DLQ B) was shown to mediate between the childhood daily functional self-actualization and state anxiety [95% CI (LB −0.34, UB −0.35; P < .05)].
Discussion
As an extreme human experience, the COVID-19 pandemic provided a unique opportunity to explore past and present daily functional factors and their relationships with physical and mental health implications among older adults. Prior studies demonstrated that the conditions of isolation during this time adversely affected this population’s physical health and anxiety,39,40 and this study offers a greater understanding of which physical health symptoms prevailed. Like other studies, our results show that older adults experienced certain physical health symptoms that may be part of the aging process,41,42 with back pain being the most reported. Sha et al 6 reported that 51% of adults older than 60 years described their health as deficient; the most prevalent self-reported symptoms were musculoskeletal, back pain, fatigue, shortness of breath and difficulty sleeping. Similarly, Jones et al 42 mentioned lower back pain among older adults’ most frequently occurring conditions. These health symptoms provide insight into the physical risks older adults might encounter as they age.
Later life is associated with additional changes and transitions, such as retirement, loss of close friends and family members and emotional health issues. 19 Our study confirmed findings from a study in China, 37 in which a significant number of participants reported having experienced such a life event (especially death, illness and work-related issues). These events were perceived negatively, affecting self-perception and even limiting participation in physical activities. 43 Life events that occur in later life (eg, the COVID-19 pandemic) complicate older adults’ ability to cope with other stressful situations. This could explain the associations between sleep quality, daily functional actualization and health symptoms we noted in our study.
We also found significant relationships between childhood daily functional self-actualization (C.DailyFA) and sleep quality and cognitive symptoms or impairments. This finding supports those in previous studies, suggesting that negative childhood events have adverse outcomes for older adults’ cognitive performance and sleep quality. 44 Despite addressing diverse childhood adversities (eg, parents’ divorce or separation, financial difficulties and feuds at home) and ages (eg, participants ranged from 20 to 54 years in Koskenvuo’s study 44 ), those prior studies provided evidence of the impact of childhood events on present adult life risks.
The potential risks and consequences of the COVID-19 period are emphasized in the present daily functional self-actualization concept (DailyFA). Self-actualization becomes relevant once basic physiological and safety needs are met 45 —but the COVID-19 pandemic threatened those basic needs. Therefore, it is unsurprising that participants did not score high for daily functional self-actualization. Instead, their scores were associated with health symptoms and state anxiety, pointing to the importance of relating individuals’ feelings to their daily functional ability to maintain well-being.
Besides reporting deficient daily functional self-actualization, participants also pointed to worsened daily functional cognition (DLQ) throughout the COVID-19 period. Although adequate abilities can serve as protective factors, older adults tend to lose cognitive functioning as they age—and difficulty executing daily tasks might raise their stress levels. 46 Their vulnerability to anxiety during COVID-19 could diminish or erase their functional cognitive abilities. The decline in their cognitive abilities may be associated with fewer intellectual activities, such as reading, writing, drawing and playing board games, and may negatively affect their health. 47 As such, the decline explains the significant correlation between cognitive symptoms or impairments (DLQ B) and physical health symptoms and state anxiety found in the current study.
Another essential component of participation is sleep. Sleep complaints are prevalent among older adults and may increase with age and crises such as COVID-19. 29 As evidence of this view, our results associated sleep quality with health symptoms, state anxiety and functional cognition. These findings highlight the importance of adequate sleep for healthy living.
Limitations and Future Research
This study’s findings should be interpreted considering several limitations. Importantly, most participants were married. Being unmarried has been identified as a risk factor for mortality from COVID-19 and may influence a person’s ability to cope with stressful events. 37 Moreover, the study was conducted urgently to investigate factors related to older adults’ health during the COVID-19 pandemic. Therefore, it used no exclusion criteria for diagnosed chronic conditions, neurological conditions, or mental illnesses. Nor did we consider social support variables, which might influence anxiety and physical symptoms. A further limitation pertains to participants completing the questionnaires online. Online questionnaires require adequate cognitive abilities, so only those with skills to use computers could participate in this study. Hence, the generalizability of these findings to encompass all older adults is constrained. In addition, due to the urgent circumstances associated with the pandemic, we created or used certain questionnaires (eg, to assess physical health symptoms, negative life events and childhood functional self-actualization) without further investigating their validity or reliability in the general or older adult populations.
In future studies among older adults, past and present functional features should be examined relative to physical health symptoms and state anxiety. Marital status and social support should be considered to represent the older adult population’s health characteristics better. Moreover, to include participants with a wide range of cognitive abilities, health care professionals could administer the questionnaires.
Conclusion
This study identified functional features associated with physical and mental health. Understanding these interconnected features expands our comprehension of available resources and offers crucial insights for individuals navigating stressful periods like the COVID-19 pandemic. By illustrating how an individual’s daily functional characteristics intertwine with health outcomes, this study contributes to the theoretical framework of embodied cognition, providing a nuanced understanding of coping mechanisms during difficult times. Acknowledging aspects of embodied cognition theory, this article emphasizes the importance of considering how both physical and mental health shape how older adults experience and function in society.
Practically, these results should also be considered when planning interventions to minimize health implications for older adults during crises. For example, these findings might apply to promoting physical activity, shown to influence behavior in a manner that may lead to improved quality of life in the long run. 48
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Science & Technology, Israel [grant number 83].
Statement of Ethics
The study protocol was approved by the University of Haifa’s Ethics Committee (approval number 199/20).