
Abstract
Although the preventive occupational therapy intervention program Lifestyle Redesign® has proven to be effective in maintaining and improving the health and quality of life of older adults, a similar program has not yet been culturally adapted to the Spanish population. As a preliminary step in developing a lifestyle intervention tailored to healthy Spanish older adults living in a nursing home (Lifestyle Choice; originally in Spanish “Elección de Estilo de Vida”), we aimed to identify and describe the life domains of this population and determine overlap with content areas addressed in the Lifestyle Redesign® program. An observational cross-sectional study was carried out using quantitative methods, including 30 healthy older adult residents in the “Virgen del Prado” nursing home in Talavera de la Reina (Toledo), based on the development of a questionnaire and a survey. Six life domains were identified: self-care, sleep and rest, mobility, personal safety, health maintenance, spirituality, and free time usage. The results of this study reveal important overlaps with content areas of Lifestyle Redesign®, suggesting that it may be feasible to develop a lifestyle intervention (“Elección de Estilo de Vida”) tailored to the sociocultural features of the healthy Spanish population over 65 years old living in nursing homes.
The Lifestyle Redesign® program has proven to be effective in maintaining and improving the health and quality of life of older adults. However, a similar program has not yet been culturally adapted to the Spanish population.
The research reveals that it may be feasible to develop a lifestyle intervention (“Elección de Estilo de Vida”) tailored to the sociocultural features of the healthy Spanish population over 65 years old living in nursing homes.
This research shows that life domains are not universal, but are conditioned by culture, health status, and the environment in which older adults live. This knowledge can be used by health professionals when implementing interventions that promote the health and quality of life of older adults.
Introduction
The number of older adults is significantly increasing worldwide. 1 This trend is also observed in Spain, where the percentage of the population over 65 years of age, which represented 20.0% of the total population in 2022, would reach a peak of 30.4% by 2050. 2
This demographic change is a major challenge to society, as the increase in the older population is likely to be associated with a decline in physical health, psychological well-being, and functional capacity. 1 Therefore, effective interventions are needed to preserve and improve the health and quality of life of older adults. 3
Such interventions can be enhanced with an occupational therapy perspective, since “occupational therapy practitioners develop and implement occupation-based health approaches to enhance occupational performance and participation, quality of life, and occupational justice for populations.” 4 Moreover, as a social and health care field that addresses the prevention of disability and dependency conditions using occupation-based interventions, it becomes a vehicle for the improvement and maintenance of the health and quality of life of older adults.5,6
In line with the above, one of the preventive occupational therapy intervention programs that has demonstrated sufficient evidence of the effectiveness of occupational therapy intervention on the physical and mental health, occupational functioning, and quality of life of community-dwelling older adults is Lifestyle Redesign®.7 -9
Developed by the University of Southern California, Lifestyle Redesign® is based on the assumptions of occupational science and is informed by 2 previous research studies on occupations and their association with well-being in older adults.10,11 Initially, Jackson 10 conducted a qualitative description of the adaptive strategies used by a group of community-dwelling older adults with disabilities. The results reveal that engaging in symbolically meaningful occupations is essential to well-being among this group.
Subsequently, Clark et al 11 used a qualitative method to study the subjective perception of life domains (areas of activity of personal importance) in older adults, as well as to collect data on occupationally relevant adaptive strategies within each domain. Ten life domains have been identified: activities of daily living, adaptation to a multicultural environment, free time usage, grave illness and death-spirituality, health maintenance, mobility maintenance, personal finances, personal safety, psychological well-being and happiness, and relationships with others. This categorization of life domains played a relevant role in defining the thematic content areas within the Lifestyle Redesign® program. 11
The Lifestyle Redesign® program, structured through monthly 1-hour individual sessions and weekly 2-h group sessions over 9 months, demonstrated a reliable and cost-effective positive intervention effect on a wide range of outcomes, such as life satisfaction, role functioning, and self-rated physical and emotional health of community-dwelling older adults.7,8,12
Given these positive effects, the program has been widely implemented and adapted to other culturally specific settings, including UK residents,13 -15 migrants in the Netherlands, 16 Swedish population, 17 Latinos in California,18 -20 French-Canadians,21,22 and Israeli population. 23
However, despite its effectiveness in maintaining and improving the health and quality of life of older adults, the literature review did not identify any studies in which a similar program was culturally adapted to the Spanish population. To address this literature gap, based on the original paper of Clark et al 11 and the cultural adaptations of the Lifestyle Redesign® program found in a literature review, we consider it essential to know what healthy Spanish older adults living in nursing homes perceive as the most relevant and meaningful areas of activity (life domains). The absence of such programs aimed at Spanish older adults is significant for several reasons. Spanish older adults, like individuals of any cultural group, have unique needs, interests, and values that must be respected and incorporated into their care to have a positive impact on their health. In the absence of a culturally adapted program, there is a risk of neglecting or overlooking these specific cultural aspects. In summary, the cultural relevance and sensitivity of programs developed in nursing homes are essential to improve the quality of care, the effectiveness of health outcomes, and psychological well-being.
Hence, the main objective of this study is to (1) identify and describe the life domains of healthy Spanish older adults (over 65 years old) living in nursing homes and, consequently, to develop the thematic content areas that will comprise a culturally specific lifestyle intervention (Lifestyle Choice; originally in Spanish “Elección de Estilo de Vida”) informed by the original Lifestyle Redesign® program for older adults in the United States. This study is based on the hypothesis that life domains will be different in the Spanish and U.S. older adult population, and therefore it is necessary to examine them in depth.
Methods
Study Design
Following a quantitative methodology, a cross-sectional descriptive observational study 24 based on the development of a questionnaire and a survey was conducted from October 1 to 31, 2022. The study participants were 30 healthy Spanish older adults (over 65 years old) living in the “Virgen del Prado” nursing home in Talavera de la Reina.
The Research Ethics Committee (CEIm) of the Integrated Healthcare Management of Talavera de la Reina approved the study (Research Ethics Committee reference number: 34/2022; approved on September 30, 2022).
Setting
Recruitment of participants was carried out from October 1 to 15, 2022, in the “Virgen del Prado” nursing home in Talavera de la Reina (Toledo).
This nursing home is a public institution owned by the Regional Government of Castilla-La Mancha and managed by the Department of Health and Social Affairs. The nursing home offers the following services: accommodation (both permanent and temporary), personal care and food and nutrition program, cleaning and disinfection services, ironing, and laundry, Also, the facility offers geriatric medical care and nursing care, physiotherapy, occupational therapy, basic podiatry services, hairdressing, cafeteria, library, and chapel, as well as activities of entertainment, integration, participation, communication with families, volunteering, and social relations.
In addition, data collection was performed from October 16 to October 31, 2022, in an office specifically equipped for this purpose to preserve confidentiality at the “Virgen del Prado” nursing home in Talavera de la Reina.
Participants
The study sample was selected according to the following inclusion criteria: aged 65 years or older, living in the “Virgen del Prado” nursing home in Talavera de la Reina, normal cognitive function (score ≥ 24 on Cognitive Mini-Test), 25 functionally independent (score ≥ 80 on the Barthel Index) 26 and Spanish-speaking. It should be noted that the inclusion criteria related to cognitive functioning and functional independence of the participants were the same as those established by the Lifestyle Redesign® program. Those older adults who did not authorize their participation in the study, those with disabling health conditions (chronic diseases, physical or cognitive impairment, or social problems causing dependence), and those who were not Spanish nationals (to facilitate interaction with the participants) were excluded.
For the recruitment of participants, the director of the “Virgen del Prado” nursing home in Talavera de la Reina was first contacted. After the director’s approval to carry out this study, a meeting with the occupational therapists of the nursing home was held to identify and collect data from participants who met the eligibility criteria, using their occupational history. Subsequently, 42 residents who met the eligibility criteria were invited to participate in the study. They were verbally provided with information about the study and the implications of their participation. They were also informed that their refusal to participate would have no consequences, and it was emphasized that they could discontinue their participation in the study at any time. Finally, 30 residents volunteered for the study, signed the written informed consent, and attended a brief presentation on the objectives and methods of the study by the investigator C.U. The remaining 12 residents did not participate, as 2 of them were hospitalized and the other 10 refused to sign the written informed consent.
Data Sources/Measurement
Two instruments were used to collect the data for the study. First, a background questionnaire was used to record the socio-demographic aspects of the participants: age, gender, marital status, educational level, number of years residing in the nursing home, pension, and self-reported health status (see Appendix S1). This questionnaire has been designed based on the analysis of the most relevant sociodemographic data on the health of the population over 65 years old. 1 These data were used to describe the sample and to determine the characteristics of the residents that might influence the identification of life domains.
The second instrument was a Likert-type meaningful activities survey designed ad hoc by culturally adapting the occupations described in the Occupational Therapy Practice Framework. 4 This survey aimed to identify the most meaningful areas of activity and those of most personal relevance to the participants. It consists of 25 items, structured into 6 occupational areas: activities of daily living (ADLs), instrumental activities of daily living (IADLs), health management, sleep and rest, leisure, and social participation. Each item scores from 1 (not important) to 5 (very important) (see Appendix S2).
The questionnaire and the survey were individually and anonymously administered to each of the participants by the researcher C.U., in a place conditioned for this purpose to preserve confidentiality. This study was carried out with special attention to the confidentiality of the study participants. All information generated and collected during this study complies with the Organic Law 3/2018, of December 5, on the Protection of Personal Data. The documents containing the sociodemographic data of each participant and their responses to the survey were coded with a letter and a number. In addition, documents containing personal information were always kept under lock and key, accessible only to the researchers of this study.
The data were collected from October 16 to 31, 2022, in the “Virgen del Prado” nursing home and registered in a data coding sheet by the researcher P.M., using Microsoft Excel®, version 16.16.21 software.
The response rate for both the questionnaire and the survey was 100.0%.
Bias
To avoid potential selection bias, the occupational therapists at the nursing home were responsible for identifying and collecting data from participants who met the eligibility criteria, based on their occupational history. In addition, to address potential confirmation bias, data were collected from a representative sample.
Also, the questionnaire and survey were administered individually and anonymously to each participant by the researcher C.U., who received appropriate training for this purpose, to avoid participant nonresponse bias and interviewer bias, respectively.
Study Size
The sample size was calculated using the OpenEpi, version 3 software (https://www.OpenEpi.com)
N is population size (for finite population correction factor or fpc) = 42; p is the hypothesized (%) frequency of outcome factor in the population (50% ±10; confidence limits as % of 100) (absolute ±%); (d) = 10%; DEFF (design effect = 1); Z is a constant = 1.96 for 95% confidence interval. Based on the above parameters the minimum required sample size (n) was 30 participants.
Statistical Methods
The completed questionnaires and surveys were manually coded and checked for completeness and consistency. The data were then, cleaned and recorded on a data coding sheet, using Microsoft Excel®, version 16.16.21; in which, to ensure data privacy and confidentiality, no clinical or identification data of the participants were included.
The socio-demographic characteristics and the results of the meaningful activities survey were analyzed using descriptive statistics: mean (M), percentages, and standard deviation (SD). Also, association indices were used for the qualitative and ordinal variables (Wilcoxon rank-sum tests), and the quantitative and ordinal ones (Pearson’s correlation coefficient). The level of statistical significance was set at P-value < .05.
To control for confounding factors, a restriction strategy was used, that is, restrictive inclusion and exclusion criteria were specified with the aim of making the included participants as homogeneous as possible in terms of factors that could distort the association.
Data processing and analysis were performed using the Spanish version of the IBM SPSS-Statistics®, version 26.0 for Windows software.
All data were analyzed and supervised by a specialized statistician who was responsible for data input and management, as well as statistical analyses.
Results
Study participants were aged between 65 and 97 years (M ± SD = 80.6 ± 10.4). Most of the subjects were male (56.7%), widowed (50.0%), with a primary level of education (compulsory education) (86.7%) and received a contributory pension (76.7%). One-third of them rated their health status as good (33.3%), and the mean of years residing in the nursing home was 4.3 ± 3.6 (M ± SD) (see Table 1).
Socio-demographic Characteristics of the Participants (N = 30).

The results showed that most of the participants considered performing the following activities very meaningful or relevant: going to the toilet and toilet hygiene; washing and drying their face and hands; caring for their skin, eyes, nose, and ears; combing their hair; brushing their teeth; caring for their nails; shaving; removing their body hair; applying and removing creams or cosmetics (100.0%), dressing (100.0%), bathing or showering (93.3%), moving around their room or from one place to another in the nursing home (90.0%), and eating and drinking (70.0%). Sexual activity with oneself or others showed a greater variability of responses; whereas a large proportion of participants considered it quite important (40.0%) or very important (20.0%), some considered it as not important (23.3%).
Activities related to maintaining personal safety (100.0%), caring for others (70.0%), engaging in religious and spiritual (63.3%) activities, sending, and receiving information (56.7%), shopping (56.7%), and moving around within the community (53.3%) obtained high scores in the analysis of the results. Performing financial management activities showed a highly polarized response: half of the participants considered it not important (50.0%), and another large proportion considered it very important (43.3%). This division of responses is also observed in the activities of care, maintenance, and repair of the home, furniture, appliances, yard, garden, and vehicles; with half of the subjects considering it as very important (50.0%) and another large percentage considering it as not important (43.3%).
In addition, communication with the healthcare system (83.3%), use, cleaning, and maintenance of personal care devices (83.3%), coping with illness and death (83.3%), and engaging in physical activity (80.0%) were identified as very important activities by the majority of participants.
Additionally, high percentages of subjects rated as very important the activities related to preparing their room, undressing, reading, turning on the radio, and listening to music to induce or help them fall asleep (96.7%), the activity of sleeping well (80.0%) and rest, and taking short naps throughout the day (56.7%).
Activities related to the identification of interests and hobbies and engaging in leisure and free time activities were rated as very important by almost all participants (86.7%).
Furthermore, half of the individuals reported engaging in activities with family and friends as very important (53.3%). In contrast, engaging in activities at the community level and with other residents showed a great polarization of responses; whereas approximately half of the participants found them as not important (46.7% and 40.0%, respectively), another large proportion rated them as very important (36.7% and 33.3%, respectively) (see Table 2).
Results of the Meaningful Activities Survey (N = 30).
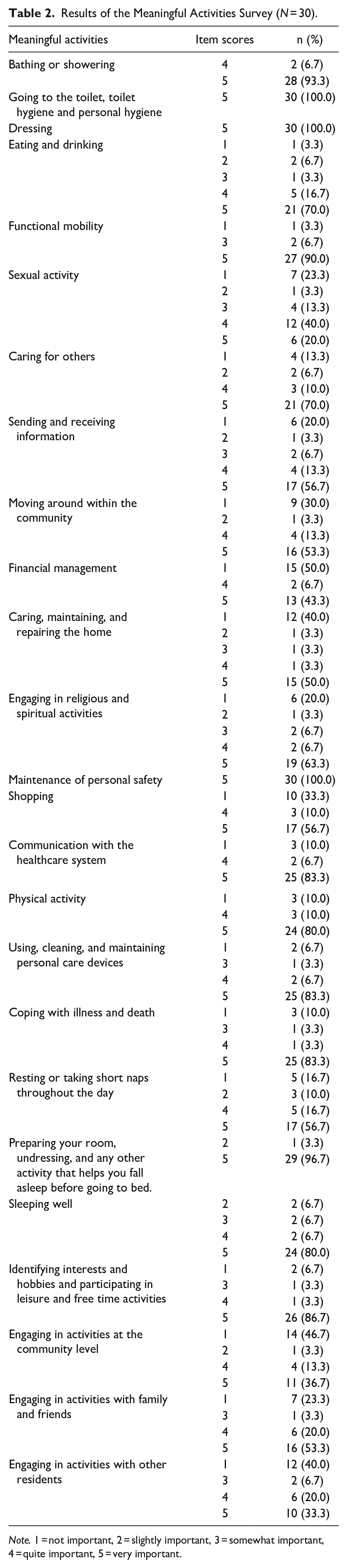
Note. 1 = not important, 2 = slightly important, 3 = somewhat important, 4 = quite important, 5 = very important.
After an initial analysis of the data, 9 domains were initially identified, comprising those activities rated as very important by at least 50% of the participants. These were activities related to (a) self-care, sleep, and rest; (b) mobility; (c) instrumental activities of daily living; (d) personal safety; (e) personal finances; (f) health maintenance; (g) spirituality; (h) free time usage, and (i) relationships with others.
Subsequently, in order to obtain a more refined, accurate, and consistent typology of life domains, the researchers selected activities that were rated as very important by at least 80% of the participants and that also showed greater homogeneity of response. As a result of this process, 6 life domains were identified, which are presented under the following subheadings.
Self-Care, Sleep, and Rest
The activities included in this life domains were going to the toilet and toilet hygiene; washing and drying your face and hands; caring for your skin, eyes, nose, and ears; combing your hair; brushing your teeth; caring for your nails; shaving; removing your body hair; applying and removing creams or cosmetics; dressing; bathing and showering; and those related to preparing to sleep or rest: preparing your room, undressing, reading, turning on the radio or listening to music or any other activity that helps you fall asleep before going to bed; and the activity of sleeping well.
Mobility
The activities identified in this life domains were mobility within the immediate environment where the older adult resides, moving around one′s room or from one place to another in the nursing home.
Personal Safety
This life domain was constituted of those activities related to the maintenance of personal safety, such as recognizing potentially hazardous or harmful situations, avoiding unsafe neighborhoods, going out accompanied, and calling emergency services.
Health Maintenance
The activities included in this life domains were those involving the development, management, and maintenance of health and wellness routines, including communication with the healthcare system, using, cleaning, and maintaining personal care devices, and engaging in physical activity, among others.
Spirituality
This life domain was composed of those activities involving religious beliefs, such as attending religious ceremonies or celebrations; in particular, those related to coping with grave illness and death, for example, visits to convalescents, care, and assistance to patients, and attending wakes and funerals.
Free Time Usage
The activities identified in this life domains were those related to the use and enjoyment of free time, such as identifying interests, and hobbies and participating in leisure, recreational, and free time activities.
Finally, the association of all the socio-demographic variables shown in Table 1 with the life domains was analyzed. Regarding qualitative and ordinal variables (gender, marital status, educational level, etc.), a significant association was found exclusively between gender and physical activity (Wilcoxon rank-sum tests, P ≤ .001). Regarding the degree of association between quantitative and ordinal variables (age, self-reported health status, financial management, etc.), significant associations were found exclusively among age and interests, hobbies and engaging in leisure and free time activities variables (r = −.367, P = .046); and between self-reported health status and financial management variables (r = −.482, P = .007). Also, in particular, a moderate negative association was found for both variables, that is, as the age of the participants increased, the importance of interests, hobbies and leisure activities decreased, or vice versa. Moreover, as the participants’ self-reported health status decreased, the importance of financial management increased, or vice versa.
Discussion
In brief, the key findings of this study have allowed us to identify 6 life domains particularly relevant to Spanish older adults: self-care, sleep and rest, mobility, personal safety, health maintenance, spirituality, and free time usage. Therefore, the main objective of this research, which was to identify and describe meaningful life domains of healthy Spanish older adults living in nursing homes, has been achieved.
This finding demonstrates its similarity to most of the life domains identified by the Lifestyle Redesign® program. 11 Similar life domains, containing comparable activities, such as self-care, mobility, and personal safety, have been found in both studies. We consider these domains to be particularly significant for Spanish older adults since they are closely related to the performance of the most basic activities of individuals and are the domains that are most closely linked to the survival and functional independence of older adults. This is due to the fact that if an older adult has difficulties in self-care, has mobility problems, or their safety is compromised, their autonomy, well-being, and quality of life are likely to decrease, as they will be dependent on others to perform activities of daily living. Therefore, we consider that it is feasible to develop a lifestyle intervention (“Elección de Estilo de Vida”) informed by the original program, attending to the social and cultural peculiarities of the Spanish population.
Some differences in the activities that are integrated with each life domain and their meaning for older adults were also observed. According to Muñoz, 27 the development of culturally responsive occupational therapy programs implies that they must be adapted to the particularities of the target population, as in the case of the Lifestyle Redesign® program.
Firstly, activities related to sleep and rest, in particular, taking short naps throughout the day, are not included in the thematic contents of the Lifestyle Redesign®, whereas it is part of the life domain identified in our research. This discrepancy is likely a reflection of the characteristics of the Spanish physical and cultural environment. Taking a nap is a deeply rooted custom in Spanish culture and, possibly, an adaptive mechanism, given that temperature in the summer months often exceeds 35°C in the central hours of the day. 19 This difference may also be due to the time lag between the original Lifestyle Redesign® program and this research. It is quite possible that US culture has changed substantially since the initial development of the original program and now places greater importance on activities related to sleep and rest.
Secondly, activities related to health maintenance, specifically those of communicating with the healthcare system, are not included in the Lifestyle Redesign®, whereas they are included in our study. This is probably related to the importance that older people attribute to this type of activities nowadays, which leads us to reflect on their necessary incorporation into health and quality of life programs for the older population.28,29 Certainly, activities that have undergone the most changes in recent years are those linked to communication with the healthcare system. The progressive implementation of Information and Communication Technologies (ICTs) as a priority means of communication with the healthcare system, to the detriment of direct interaction with healthcare professionals, has been a difficulty and a challenge for people over 65 years of age.30,31
Another major difference concerns activities to identify interests in leisure and hobbies. The Lifestyle Redesign® focuses exclusively on the participation of older adults in leisure and free time activities, but not in those related to identifying interests and hobbies. In our view, promoting those activities among older adults is essential to improve their health and quality of life. This is supported by previous research,32 -34 which assume that identifying interests in leisure, and hobbies and prioritizing older adults’ ability for choice associated with the performance of personally and culturally meaningful activities, satisfies their needs for coping and influence in the nursing home environment, improves the performance of ADLs, reduces pain, and increases their perception of quality of life.
Furthermore, the life domain called spirituality in our study differs from the one called “grave illness and death-spirituality” in the Lifestyle Redesign®. Although there are similarities between them, as they refer to activities related to religious practices and beliefs, and especially those related to coping with grave illness or death, there are also significant cultural differences. The activities included in this life domain would possibly reveal some particularities of Mediterranean society and culture, giving substantial symbolic weight and meaning to those activities related to religious practices and beliefs. For example, in Spain a 24-h vigil is kept after the death of a person, several Catholic masses are dedicated to the deceased, and mourning can last for several years. 35
The results in the area of personal finances and activities related to relationships with others are probably the most remarkable difference between the results of this study and Lifestyle Redesign®.7 -9 The activities associated with these life domains of Lifestyle Redesign® have not been identified as particularly relevant in our study.
On one side, personal finance activities may not be relevant possibly due to the increase of digital banking services, to the detriment of direct and personalized customer service, which makes it difficult to carry them out, and leading older adults to delegate them to family members. 36 It may also be conditioned by the health status of older adults, as a significant negative association was found between self-reported health status and the importance of financial activities. This may indicate that older adults feel capable of performing them and therefore do not consider them particularly meaningful or important. In conclusion, while the increasing use of digital banking services for older adults may offer benefits in terms of convenience and accessibility, it also presents challenges related to technology adoption, security, and potential isolation. On the other side, the fact that activities related to relationships with others were not significant may be due to the unique characteristics of the environment. The “Virgen del Prado” nursing home is located in the center of a small town (less than 70 000 citizens) where there are accessibility difficulties due to the presence of architectural, urban, transport, and communication barriers. This may be related to a phenomenon called urban social iatrogenesis, which is characterized by the progressive isolation of older adults in their own homes or the center in which they reside, the loss of social ties, and the disengagement from full citizenship due to urban design. 37 Moreover, it should also be noted that these activities are closely linked to those in other domains with which they may overlap, such as spirituality (eg, attending mass with the church group), which are particularly relevant in the social and cultural life of the Spanish older adult population and often serve as a vehicle for social relations. 35 It may also be a sign of a process of medicalization of the older adult residents. This process is characterized, among other things, by the predominance in the programs of institutions for older adults of activities related to physical functionality and mental state, to the detriment of other types of leisure, educational, and social participation activities. 38
Finally, the “adaptation to a multicultural environment” life domain included in the Lifestyle Redesign® was not identified in this study. This may be due to the fact that in the age range (M = 80.6 years) of the participants the phenomenon of multiculturalism does not exist, given that in the society of this group of the population there was no immigration to Spain but emigration. 39
As we will point out below, the most relevant practical implications refer to the design and development of specialized care plans, particularly culturally relevant and sensitive occupational therapy programs. Considering the differences between the life domains identified and those of the Lifestyle Redesign® program, it would be necessary to design programs that give greater importance to activities related to sleep and rest, as well as those related to communication with the healthcare system. Moreover, activities to identify interests in leisure and hobbies should occupy a priority place in the programs developed for the Spanish population, given the significant differences found. In addition, activities linked to spirituality should occupy a prominent place, insofar as these activities are a vehicle for social relations among Spanish older adults.
To conclude, we would like to highlight the strength and relevance of the identified life domains for healthy Spanish older adults living in nursing homes. Practically, no socio-demographic variable has been found to be determinant in their definition. That is, for healthy older adults of all age groups, marital status, and educational and income levels, the activities included in the domains are key.
However, it cannot be concluded that these life domains are universal, as they are conditioned by culture, health status, and the environment in which older adults live. The potential impact of this study is based on the recognition of the need to develop culturally adapted programs for Spanish older adults living in nursing homes. The most relevant practical implications refer to the design and development of specialized care plans, in particular culturally relevant and sensitive occupational therapy programs, the specific training of staff in cultural competence, as well as the creation of welcoming and inclusive residential environments. In this way, it will be possible to improve the quality of care received, the health outcomes, and the well-being of Spanish older adults living in nursing homes. For this reason, the development of studies such as the present one is essential for the analysis of occupation-based interventions. That is the only approach that ensures sensitive attention to the cultural uniqueness of the population.40,41
Limitations
The setting of the nursing home where the study was carried out is located in a small town, which may have influenced the characteristics of the participants. Therefore, we must consider possible sources of selection and information bias. Although this study meets the criteria for a representative sample, the number of subjects included was relatively small, so extrapolation of the results obtained to other contexts or population profiles must be done with caution. Furthermore, this type of design is not sensitive to changes over time, so we cannot identify trends in individuals’ life domains.
Conclusion
In this study, 6 culturally sensitive life domains have been identified in the healthy Spanish older adult population living in nursing homes. These are self-care, sleep and rest, mobility, personal safety, health maintenance, spirituality, and free time usage. The similarities of the activities contained in these life domains with those addressed in the Lifestyle Redesign® approach for well older adults in the United States suggest that it may be feasible to develop a lifestyle intervention (“Elección de Estilo de Vida”) tailored to the sociocultural peculiarities of the healthy older Spanish population living in nursing homes.
In conclusion, the contributions of this study are significant for the development of culturally adapted interventions, since the cultural relevance and sensitivity of the programs developed in nursing homes are essential for improving the quality of care, the effectiveness of health outcomes and the psychological well-being of older adults.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231220217 – Supplemental material for Life Domains and Lifestyle of Older Adults Living in a Nursing Home: A Pilot Study
Supplemental material, sj-docx-1-inq-10.1177_00469580231220217 for Life Domains and Lifestyle of Older Adults Living in a Nursing Home: A Pilot Study by Cristian Uceda-Portillo, José-Ignacio Calvo-Arenillas and Pedro Moruno-Miralles in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The researchers of this investigation would like to thank the director, Joaquín Fernández; the occupational therapists, Nuria Corrochano and Begoña Mencias; the orderly attendants, and the older adults that participated in the study at the “Virgen del Prado” nursing home in Talavera de la Reina (Toledo).
Data Availability Statement
The data used to support the results of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the European Social Fund and the ONCE Foundation.
Declaration of Ethics
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee (CEIm) of the Integrated Healthcare Management of Talavera de la Reina (Research Ethics Committee reference number: 34/2022; approved on September 30, 2022).
Declaration of Informed Consent
Written informed consent was obtained from all subjects involved in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.