
Abstract
Many nursing homes operated at thin profit margins prior to the COVID-19 pandemic. This study examines the role of nursing homes’ financial performance and chain affiliation in shortages of personal protection equipment (PPE) during the first year of the COVID-19 pandemic. We constructed a longitudinal file of 79 868 nursing home-week observations from 10 872 unique facilities. We found that a positive profit margin was associated with a 21.0% lower probability of reporting PPE shortages in chain-affiliated nursing homes, but not in non-chain nursing homes. Having adequate financial resources may help nursing homes address future emergencies, especially those affiliated with a multi-facility chain.
Nursing homes faced challenges obtaining necessary personal protection equipment (PPE) during the early phase of the COVID-19 pandemic. Nursing homes were often operating at thin profit margins prior to the pandemic.
Chain-affiliated nursing homes on better financial footing were less likely to experience any PPE shortages, especially during the period with high COVID-19 infection rates. Profit margins were not associated with PPE shortages in non-chain nursing homes.
The ability of nursing homes to obtain PPE is related to their financial strength, indicating that shoring up their financial situation may help nursing homes address future emergencies.
Introduction
The COVID-19 pandemic has disproportionately affected nursing homes (NHs) in the United States because of their congregate nature and the vulnerability of their residents. As of July 2023, over 1.6 million COVID-19 cases have been confirmed in residents, plus another 1.6 million cases in staff. 1 The nature of NH care requires staff and residents to wear personal protective equipment (PPE) to prevent transmission of the COVID-19 virus, especially prior to the availability of COVID-19 vaccines.2,3 Despite federal recommendations on PPE use in NHs, 4 many facilities faced challenges obtaining necessary PPE, especially during the early phase of the COVID-19 pandemic. These challenges were also widespread in all other sectors and services (eg, hospitals, clinics), because PPE supply could not meet the demand.5,6 PPE shortages in NHs contributed to COVID-19 infections among their residents and staff.7,8
To monitor the progress of the COVID-19 pandemic, the Centers for Medicare and Medicaid Services (CMS) began publishing weekly COVID-19 cases, COVID-19 deaths, and PPE supply in May 2020.1,9 About 1 in 5 NHs reported a shortage of PPE in May 2020,8,9 and approximately half of NHs reported PPE shortages at some point from late May to August of 2020. The PPE supply improved in early 2021 following the introduction of COVID-19 vaccines. 10 Nursing home characteristics associated with PPE shortages included for-profit status, private equity ownership, and a high percentage of Medicaid residents.2,8,11 NHs with lower 5-star ratings and those in rural areas also reported more PPE shortages, especially when COVID-19 infection rates were high. 12
The financial performance of NHs may be an important factor in PPE shortages during the pandemic, although empirical evidence is lacking. NHs often operate at thin profit margins; most facilities have profit margins of 3% or less prior to the pandemic. 13 The financial performance improved slightly during the pandemic due to the relief funds and the relaxation of the 3-day rule for skilled nursing admissions. 14 Limitations in financial resources may hamper the ability of NHs to purchase PPE, especially during the early pandemic when the price of PPE increased substantially. 15 NHs with better financial performance invest more in staffing and other resources, resulting in better quality of care and fewer infection control citations.16,17 Such facilities may be more willing to invest in infection mitigation measures like PPE.
NHs affiliated with a multi-facility chain may have different organizational structures and pandemic responses to PPE shortages than non-chain facilities.18,19 One study found that chain affiliation was associated with a higher probability of PPE shortages in June-July of 2020. 8 This disadvantage may make financial resources more important to chain-affiliated NHs, suggesting that chain affiliation can potentially moderate the association of financial performance with PPE shortages. No study has examined this possibility.
To mitigate these knowledge gaps, we analyzed longitudinal, publicly available NH data: (1) to investigate the role of facility-level financial performance in PPE shortages during the first year of the COVID-19 pandemic; and (2) to assess whether chain affiliation moderates the association of financial performance with PPE shortages. We hypothesize that NHs with better financial performance were less likely to experience PPE shortages and that the association was stronger in chain-affiliated NHs.
Methods
Data Sources
We combined several public data sources to acquire detailed NH characteristics, COVID-19 information, market factors, and state policy. For NH characteristics, we merged the 2018-2019 Certification and Survey Provider Enhanced Reports (CASPER) with the 2019 Medicare Cost Reports, 2019 LTCFocus.org, 2020 Care Compare data archive, and 2020 COVID-19 Public File. CASPER collected detailed NH characteristics, including chain affiliation and bed size. We used the 2018-2019 CASPER data because CMS suspended recertification surveys of NHs in March 2020. 20 Medicare Cost Reports allowed the calculation of profit margin for each NH prior to the pandemic. 21 LTCFocus.org provided NH-level summary statistics of resident characteristics. Care Compare publicly reported staffing and 5-star ratings. The CMS Nursing Home COVID-19 Public File (COVID-19 File) published weekly counts of resident and staff COVID-19 cases and PPE shortages. PPE data were available from May 24, 2020 to March 7, 2021. Finally, the 2010 Rural Urban Commuting Areas Codes identified the rurality of NHs.22,23
The 2019 Area Health Resources File supplied county market factors. New York Times-Coronavirus Data in the United States provided cumulative COVID-19 cases for each county in 2020. 24 Finally, the 2019 CMS report on Medicaid expenditures (including managed care) for NHs allowed us to calculate state Medicaid reimbursement rates.25 -27 This study was reviewed and approved by the University of Texas Medical Branch Institutional Review Board.
Study Cohort
Supplemental Figure 1 presents our cohort selection process. We first obtained 14 590 unique NHs from 2018-2019 CASPER. We then removed NHs lacking profit margin information or those considered outliers (beyond ±4 standard deviations of the mean) (N = 2232). Excluding outliers in NH finance studies is necessary due to frequent reporting errors, ensuring the maintenance of reasonable cost values.28 -30 Hospital-based NHs were excluded at this step because they do not have Medicare Cost Report data and focus primarily on subacute or post-acute care patients. Because CMS reported COVID-19 data weekly, we selected NHs with data in the last week of each month to simplify the analysis and excluded facilities with incomplete weekly PPE data (N = 1179). Finally, we dropped NHs with outliers or missing data on chain affiliation or total staffing levels (ie, zero staff, beyond ±4 standard deviations, >24 h per resident day) (N = 181). 31 Our final study cohort consisted of 79 868 NH-week observations from 10 872 unique facilities from May 31, 2020 through the week of December 27, 2020. Compared to study NHs, excluded facilities were less likely to be chain-affiliated, for-profit, or located in rural areas (Supplemental Table 1). They also had a smaller number of beds, lower occupancy rates, a higher percentage of Medicare residents, and a lower percentage of Medicaid residents.
Main Variables of Interest
The outcome variable was whether an NH experienced any shortages in one or more types of PPE: N95 masks, surgical masks, eye protection, and gowns. CMS required NHs to answer whether they had a 1-week supply of each type of PPE (yes/no) in the weekly survey. Profit margin, the main independent variable measuring financial performance, was defined as total revenues minus total expenses divided by total revenues, expressed as a percentage. 17 We calculated 2019 profit margins from Medicare Cost Reports to represent the financial status before the pandemic. Because outliers from data errors are common in profit margins, we excluded NHs with profit margins that were beyond 4 standard deviations of the mean.17,32 We then dichotomized profit margins as positive or negative, to account for the skewness of the distribution and a potential non-linear relationship of profit margins with PPE shortages.17,32 Chain affiliation indicated whether a NH was affiliated with a multi-facility chain (yes/no).
Covariates
The COVID-19 File provided weekly numbers of resident and staff COVID-19 cases from the week of May 31, 2020 through the week of December 27, 2020.9,33 We scaled the number of cases to the number per 100 beds, to account for differences in facility size. 9 We included the following NH characteristics potentially associated with PPE shortages: ownership, number of beds, occupancy rate, dementia special care unit, total staffing hours per resident day (including registered nurse, licensed practical nurse, and certified nursing assistant), minority-serving facility, case-mix acuity index, percentage of Medicaid residents, percentage of Medicare residents, rurality, and overall 5-star quality rating.9,33,34 Minority-serving facility indicated whether a NH served a high proportion of Black, Indigenous, and People of Color (BIPOC) residents in the state. 35 We first ranked facilities in terms of the proportion of BIPOC residents within the state, then identified facilities in the top decile from each state. Rurality was defined as urban, micropolitan (large rural city/town), and rural (small rural town/isolated small rural town).26,30 We dichotomized overall 5-star ratings into 4 to 5 stars versus 1 to 3 stars, to indicate high versus low quality of care.
County-level market factors included number of COVID-19 cases, number of primary care physicians per 1000 population, the concentration of total NH beds measured by the Herfindahl–Hirschman Index, 36 Medicare Advantage penetration rate (percentage of all Medicare beneficiaries in the county with Medicare Advantage), median household income ($), and percentage of older population (≥65 years).33,37,38 We calculated Medicaid reimbursement at the state level as the ratio of the state’s total Medicaid expenditures on NHs divided by the total number of Medicaid bed days. 27 We approximated Medicaid-paid bed days in a year using the following formula: total number of residents × occupancy rate × percent Medicaid residents × 365. 27
Statistical Analysis
We plotted the trends in any PPE shortages and individual PPE shortages from the week of May 31, 2020, through the week of February 28, 2021. We also presented the distribution of 2019 profit margins, after excluding outliers. We then described PPE shortages, COVID-19 factors, NH characteristics, market factors, and state policy. We also compared the differences in these factors by positive profit margin, using t-tests for continuous variables and chi-squared tests for categorical variables.
This study employed a longitudinal design for 2 primary reasons. First, descriptive analyses examined the longitudinal changes in PPE shortages over time. Second, although the independent variable (profit margin) was only cross-sectional, we observed fluctuations in the outcome over time. We built a longitudinal analytical file with multiple observations for each nursing home over time. To accommodate the longitudinal data structure, we employed random effects models, accounting for both within-subject correlation and individual variation. Using a random effects logistic regression, we examined the relationship of positive profit margin and chain affiliation with any shortages in PPE supply, with a maximum of 8 observations per NH (May 31, 2020 to December 27, 2020). A fixed effects model was inappropriate because the 2019 profit margin did not change within a facility. We built the final multivariable regression model in 2 steps. First, we ran a full model with all NH characteristics, market factors, and Medicaid reimbursement rates, as described in the previous section. Second, we removed variables with P > .05 to simplify our model, except for 4 important variables associated with PPE shortage in prior studies (resident COVID-19 cases, total staffing hours, 5-star rating, and rurality).2,8,10 To assess the moderation effect, we included the interaction of profit margin and chain affiliation. Continuous variables were standardized at overall means and standard deviations. 26 Marginal effects of positive profit margin by chain affiliation were computed using the “margins” function in Stata after the regression. A sensitivity analysis repeated the random effects logistic regression for raw profit margins (Supplemental Table 2).
Separate logistic regressions with state indicators were conducted to examine the association of positive profit margin with any PPE shortages by chain affiliation for each reporting week. Logistic regressions controlled for the same covariates in the random effect model. We separately plotted the marginal effects and 95% confidence interval (CI) of profit margin. We also compared whether the marginal effects differed in chain versus non-chain NHs for each week and overall (Figure 2 and Supplemental Table 3).
All statistical analyses were performed in SAS 9.4 (SAS Institute Inc., Cary, NC) and Stata 16.0 (StataCorp LLC, College Station, TX). Two-tailed statistical significance was considered for alpha at the .05 level.
Results
Figure 1 shows the trends of NHs with any PPE shortages over the study period. In the week ending May 31, 2020, 26.3% of NHs reported shortages in one or more types of PPE, most commonly gowns and N95 masks (Supplemental Figure 2). In late July and August 2020, over 20% of NHs still reported PPE shortages. The proportion of NHs with PPE shortages started to decrease in September 2020, with 9.6% reporting shortages by December 2020.
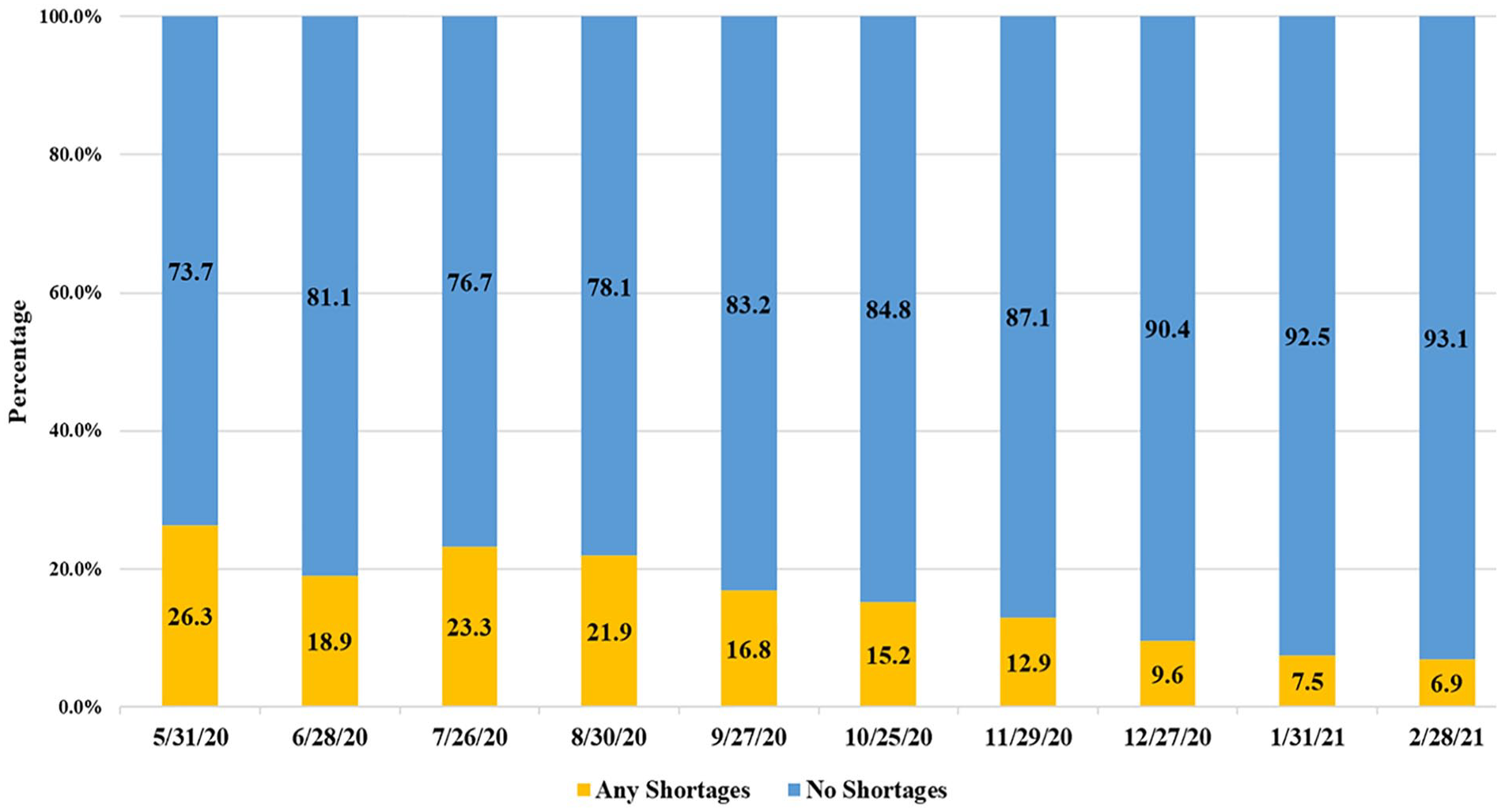
Trends of nursing homes with any PPE shortages from May 2020 through February 2021.
Table 1 presents descriptive characteristics by profit margin for September 2020. The average 2019 profit margin was −0.53%, with 53.2% of NHs reporting a positive profit margin (distribution provided in Supplemental Figure 3). Most NHs were chain-affiliated (62.3%), for-profit (73.7%), and in urban areas (66.3%). Table 1 also identifies several characteristics that differed in NHs with positive versus negative profit margins, such as chain affiliation and 5-star ratings. A lower percentage of NHs with positive profit margins experienced any PPE shortages (16.2%vs 17.6%, P = .047). No differences between facilities with positive versus negative profit margins were found for number of weekly resident and staff COVID-19 cases and county COVID-19 cases.
Nursing Home Characteristics, Market Factors, and State Policy by Profit Margin in September 2020.

Note. Data sources included the 2018-2019 Certification and Survey Provider Enhanced Reporting, 2019 Medicare Cost Report, 2019 LTCFocus.org, 2020 Nursing Home COVID-19 Public File, 2020 Care Compare data archive, 2019 Area Health Resources File, and 2019 CMS report on Medicaid expenditures.
Total Staffing = registered nurse, licensed practical nurse, and certified nursing assistant; Micropolitan = Large Rural City/Town; Rural = Small Rural Town/Isolated Small Rural Town; HHI = Herfindahl-Hirschman Index; SD = standard deviation; PPE = personal protection equipment.
P < .05. **P < .01.
P values measures whether nursing homes with positive or negative profit margin had the same characteristics using t-tests for continuous variables, and Chi-square tests for binary variables.
Table 2 presents model estimates and marginal effects of the random effects logistic regression on any PPE shortages. Overall, a positive profit margin was associated with a higher probability of any PPE shortages, but the association was only marginally significant (marginal effect = −0.9%, P = .066). Chain affiliation was associated with a 3.7% increase in PPE shortages (P < .01). We found a significant interaction of chain affiliation with profit margin. Chain-affiliated NHs with a positive profit margin were 21% less likely to report any PPE shortages than chain-affiliated NHs with a negative profit margin (marginal effects = −21%, 95% CI = −37%, −5%, P = .01), but this association was not found in non-chain NHs. We also found that several NH characteristics were associated with PPE shortages, including the number of beds, for-profit, any staff COVID-19 case, and percent of Medicaid residents. Staff hours per resident day and star ratings were not associated with PPE shortages. Interestingly, neither the raw profit margin nor the interaction term of raw margin and chain affiliation was not associated with PPE shortages (Supplemental Table 2).
Random Effects Logistic Regression Examining Factors Associated with Any PPE Shortages in Nursing Homes From May 2020 through December 2020.

Note. Standard errors were clustered at the county level. State indicators were not presented.
PPE = personal protection equipment; CI = confidence interval; Micropolitan = Large Rural City/Town, Rural = Small Rural Town/Isolated Small Rural Town; HHI = Herfindahl-Hirschman Index.
Continuous variables were standardized with a mean of zero and a standard deviation of one.
Overall marginal effect of was −0.9% (95% CI: −2.0%, 0.1%, P = .066) for positive profit margin and was 3.7% (95% CI: 2.7%, 4.8%, P < .001) for chain affiliation.
Marginal effects of profit margin were −21.0% (95% CI: −37.4%, −5.0%, P = .01) in chain-affiliated nursing homes, and was 6.0% (95% CI: −15.8%, 28.0%, P = .588) in non-chain nursing homes.
The interaction term of positive profit margin and ownership status was not significant and hence excluded in the final model.
Figure 2 presents the stratified marginal effects of positive profit margin on any PPE shortages by chain affiliation from May to December 2020. The association of positive profit margins with any PPE shortages in chain-affiliated NHs grew stronger from May to June 2020, but remained insignificant. From July to November 2020, chain-affiliated NHs with positive profit margins were less likely to have any PPE shortages, with marginal effects ranging from −14.5% to −30.4% (all P < .05) (Supplemental Table 3). In late December 2020, the significant association went away. Non-chain NHs, however, showed no significant association of positive profit margins with any PPE shortages at any time during the study. The marginal effect of positive profit margins in chain-affiliated NHs significantly differed from that in non-chain NHs from August to November of 2020 (all P < .05) (Supplemental Table 3).

Stratified marginal effect of positive profit margin on any PPE shortages by chain affiliation.
Discussion
Using Medicare Cost Reports and self-reported PPE shortages data, we assessed the association between facility-level financial performance in 2019 and PPE shortages during the first year of the COVID-19 pandemic, as well as the moderation effect of chain affiliation on this association. In 2019, over half of NHs were operating at a positive profit margin. As an independent factor, profit margin was not associated with any PPE shortages, whereas chain affiliation was correlated with a higher probability of any PPE shortages. Yet, chain affiliation moderated the association of profit margin with PPE shortages. Among chain-affiliated NHs, a positive profit margin was associated with a 21% lower probability of reporting any PPE shortages, a rate which fluctuated over the study period. This association was insignificant in non-chain NHs throughout 2020.
More than 20% of NHs reported any shortages in one or more types of PPE from May to August 2020. PPE shortages were most pronounced for N95 masks and gowns, while eye protection was the least commonly reported PPE shortage. A reciprocal relationship might exist between PPE shortages and COVID-19 infections during this period. The persistent PPE shortages may have facilitated the transmission of the COVID-19 virus and led to higher COVID-19 infection rates, 39 which in return exacerbated the PPE shortages faced by NHs. PPE shortages may have contributed to avoidable hospitalizations and deaths among NH residents and staff. 39 Health policy makers and providers should reexamine their PPE supply chain and establish a more robust system for future emergencies.6,15
We also found that PPE supply improved starting in late August 2020, which may be attributed to several factors. 40 The first was an improved supply of PPE relative to demand. PPE production by existing and new manufacturers substantially increased in the middle of 2020, which resulted in decreased PPE prices. 40 The support and relief funds from the federal government might also have contributed to the improvement. 41
Our major finding is that positive profit margins were associated with a lower likelihood of PPE shortages, but only for chain-affiliated NHs. The finding of a protective effect of better financial performance on PPE shortages is similar to results reported by other studies that found a relationship between profit margins and quality.16,17 NHs with more financial resources have stronger purchasing power and may more able to pay higher PPE prices. We, however, observed this relationship only in chain-affiliated NHs. Chain-affiliated and non-chain NHs may have different organizational structures affecting the PPE supply chain.18,19,42 Non-chain NHs would need to assign an internal administrator to acquire PPE, one who is likely handling many other tasks. In contrast, chain-affiliated NHs may rely on chain-level personnel who specialize in supply acquisition. Through centralized purchasing and the purchasing power of a larger organization, chains may be better able to acquire and distribute PPE to their affiliated NHs. However, a centralized PPE supply system may reduce the flexibility of individual NHs to purchase PPE from new suppliers who have not partnered with them before. 15 This process also requires the chain to have the financial ability to purchase PPE, especially as financial resources become more important when infection rates are high. 43 In multi-facility chains, NHs that are not performing well financially may drain the financial resources of the organization, potentially reducing its ability to purchase PPE or discouraging it from purchasing PPE at inflated prices. Further investigation is needed to understand the exact mechanisms involved.
NHs with certain characteristics were more likely to experience PPE shortages. For example, NHs with more beds were associated with more PPE shortages. This finding suggests that larger facilities with more residents and staff potentially faced higher risk of COVID-19 transmission, 44 leading to an increased demand for PPE. Having any staff COVID-19 infection, but not staffing level, was associated with PPE shortages. Staff COVID-19 infections increased the demand for PPE, especially masks and gloves. 45 For-profit status was associated with higher probability of PPE shortage compared to non-profit and government facilities, which may suggest nursing homes with profit orientation may be less likely to prioritize PPE especially in a period with inflated prices. This finding aligns with a previous study that used data from mid-May 2020 to mid-July 2020. 8 Also, the insignificant interaction between profit margin and pro-profit status suggests that financial performance also matters for non-profit and government facilities. Staff levels, which did not change significantly during the pandemic, 46 were not predictive of PPE shortages in the longitudinal model. NHs with a higher proportion of Medicare residents were also more likely to report any PPE shortages. Given that Medicare covers post-acute care, and transitions in and out of a NH are more common in this population, NHs with more Medicare residents probably experienced a higher risk of initial COVID-19 infection and spread, 47 which increased the demand for PPE. Interestingly, NH star ratings, often used as a quality indicator, had no statistical relationship with PPE shortages, suggesting that PPE shortages were not solely dependent on the overall quality of NHs. This finding is consistent with a previous study that found no significant association between star ratings and PPE shortages. 2
Limitations
Several limitations should be acknowledged. (1) We included only NHs with full-year 2019 Medicare Cost Reports data, a common practice when studying NH profit margins. 17 As a result, our findings may not be generalizable to the excluded facilities, which were smaller and less likely to be chain-affiliated or for-profit. (2) The 2019 profit margins used to assess NHs’ financial performance, and hence financial standing prior to the pandemic. This financial standing may have changed between 2019 and before the start of the 2020 pandemic. (3) Our calculation of profit margins from Medicare Cost Reports could be subject to errors, which is why we excluded outliers from the analyses and dichotomized profit margins. 32 (4) The dichotomization of raw profit margins probably led to a loss of variation in the data. 30 (5) NHs’ self-reported weekly shortages of PPE may vary due to differences in interpretation among reporting individuals, potentially leading to discrepancies in reported shortage levels. 30 (6) We cannot determine whether our findings hold after March 2021, when PPE data became unavailable. (7) Like other observational studies, the causality between profit margin and PPE shortages cannot be ascertained.
Conclusions
PPE supply in NHs improved over time during the COVID-19 pandemic. Chain-affiliated NHs on better financial footing were less likely to experience any PPE shortages, especially during the period with high COVID-19 infection rates. Financial performance, however, did not lead to better PPE supply among non-chain NHs, suggesting a different organizational behavior than for chain-affiliated facilities. The ability of NHs to obtain PPE is related to their financial strength, indicating that shoring up the financial situation of NHs may help facilities address future emergencies. This requires that facilities have adequate financial reserves to cover the cost of future emergencies.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231219443 – Supplemental material for Financial Performance is Associated With PPE Shortages in Chain-Affiliated Nursing Homes During the COVID-19 Pandemic: A Longitudinal Study
Supplemental material, sj-docx-1-inq-10.1177_00469580231219443 for Financial Performance is Associated With PPE Shortages in Chain-Affiliated Nursing Homes During the COVID-19 Pandemic: A Longitudinal Study by Yejin Kang, Samuel V. David, John R. Bowblis, Orna Intrator, Brian Downer, Chih-Ying Li, James S. Goodwin and Huiwen Xu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We appreciate Amber McIlwain, MS, and Sarah Smith, PhD, from University of Texas Medical Branch for language proof.
Authors’ Note
Previous conference presentation: AcademyHealth 2021 Annual Research Meeting, June 2021, Virtual due to the COVID-19 pandemic.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JRB provides consulting services to various health care and long-term care stakeholders, including government agencies and providers. The other authors declare no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health [P30 AG024832, UL1-TR001439, R01AG081282, and R01AG087296].
Declarations,and Ethics and Consent
This study was reviewed and approved by the University of Texas Medical Branch Institutional Review Board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.