
Abstract
To identify program characteristics that influence the retention of women of reproductive age in the
Keywords
Socioeconomic, structural, and cultural factors contribute to women of childbearing age with Substance Use Disorder (SUD) motivation and decision to both enter and remain in treatment for SUD.
This research contributes to a deeper understanding of the characteristics of participants and peer recovery coach’s (PRC) roles and attributes associated with enrollment and retention of women with SUD in the CARE program.
The inclusion of PRC as integral members of SUD recovery programs may preferentially provide Black women with SUD the opportunity to build more trusting relationships with these peer coaches, thereby increasing their participation and retention.
Introduction
Substance use disorder is characterized by the recurrent, uncontrolled use of alcohol, legal or illegal drugs, and/or medications that causes clinically significant impairment and/or harmful behavioral, social, or legal consequences.1 -3 According to the National Survey for Drug Use and Health, there were >136.5 million individuals aged >12 who had a reported substance use disorder (SUD) in 2022,4,5 and of those, only 11.2% received treatment for illicit drugs. 6 This not only represents the prevalence of SUD in the United States, but the overwhelming barriers to access treatment, particularly among people of color. 4 It is important to explore the unique barriers among individuals living with SUD to optimize treatment programs and facilitate retention.
Growing evidence underscores commonly cited barriers to treatment, such as needing insurance to afford treatment, stigma, decreased health literacy, and psychiatric comorbidities.7,8 However, barriers to treatment vary among genders and racial groups. For women, especially those who are pregnant and/or have children, the barriers to accessing care include lack of childcare services provided in treatment facilities, fear of being reported to child protective services, and fear of losing custody if they seek treatment. 7 Additionally, women with SUD are more likely than men to have psychiatric comorbidities including depression, anxiety, and PTSD, 8 which can lead to higher levels of family and social impairments. This dynamic can introduce a new set of internal barriers of shame and fear of judgment by providers. 8
In interviews with patients with SUD regarding barriers to treatment access, stigma was a more pervasive theme in Black patient entries compared to White patients. 9 Medical mistrust among Black patients seeking SUD treatment is also a pervasive theme in the literature. In a survey of 143 Black patients recruited from addiction treatment facilities, 79% reported that they had experienced racial discrimination in healthcare. Participants reported that they would be more likely to seek treatment earlier and adhere to treatment recommendations if they had not feared discrimination from the medical personnel. 10
Treatment motivation and the perceived need for treatment for SUD are also culturally different among patient populations.9,11 In addition to discussing barriers to SUD treatment, assessing factors that influence retention are just as essential to improving patient outcomes. Studies have shown that even patients who are successfully linked to treatment services often end up dropping out early in the enrollment process or well before maximizing treatment benefits. 12 The lack of continued engagement in specialty care for SUD could be partially attributed to patient attitudes regarding treatment need, in addition to structural barriers, including low engagement from providers. 12 This lack of engagement with treatment services can be addressed with the incorporation of Peer Recovery Coaches (PRC) within the treatment algorithm. Studies have shown that PRC implementation in SUD treatment found significant reductions in opioid overdose and adherence to drug abstinence.13,14
To address the need for more effective SUD treatment interventions, the CARE program connected women of reproductive age with SUD with PRC to provide personalized supports throughout recovery. CARE PRC were trained and certified recovery coaches, who were also trained as Perinatal Home Visitation (PHV) Community Health Workers (CHW). This additional training prepared them to work specifically with pregnant, postpartum, or any other woman of reproductive age who also needed the support and assistance provided by a PRC. The purpose of this study was to identify characteristics of participants and PRC attributes associated with enrollment and retention of women with SUD in the CARE program.
Methods
Participant Eligibility and Recruitment
Women between the ages of 18 and 45 who were pregnant, postpartum, or planning on becoming pregnant in the coming year and had a history of or current SUD were eligible for this study. Eligible participants were referred through local health systems, behavioral and mental health clinics, treatment recovery centers, shelters, needle supply services, county jails, and from community referrals and/or word-of-mouth, and contacted by phone or in-person in response to referrals. Exclusion criteria included cognitive impairment or psychiatric disorder that would limit the ability to complete surveys and/or review educational materials, and unwillingness to provide informed consent. A total of 251 women enrolled in the prospective community-based implementation science intervention; 45 declined enrollment. Eleven women did not meet inclusion criteria. Enrollment took place between May 2018 and March 2022.
Roles and procedures for peer recovery coaches
The 8 PRC were women; 5 were Black; 2 White, and 1 Hispanic. The CARE PRC enrolled in and completed in-depth PRC training through Indiana Counselors’ Association on Alcohol & Drug Abuse to receive the Certified Addiction Peer Recovery Coach I certification. CARE PRC were also required to complete SAMHSA Screening, Brief Intervention, and Referral to Treatment grant-funded e-modules on the “Introduction to Motivational Interviewing” and “Drug Overviews.” 15
Additional in-depth training was provided to the CARE PRC by the study investigator (DL) and a perinatal psychiatrist in preparation to administer the CARE battery of validated surveys. CARE PRC could work one-on-one with women having addictions to any substances. PRC also received training as PHV CHW. This training consisted of successfully completing 9 online modules and reading corresponding chapters in the PHV CHW Manual on topics such as safe sleep, breastfeeding, postpartum depression, nutrition, and motivational interviewing. 16 Trainees participated in interactive learning through role-playing and practice case conferences over each topic in the manual, and shadowed experienced PHV CHW as they interacted with their participants.
CARE PRC partnered with representatives of over 30 programs/facilities, including residential and outpatient treatment centers, recovery homes, the Marion County Jail, etc. to meet potential CARE program participants. Typically, CARE participants were complicated cases, and each CARE PRC had weekly one-on-one meetings with her supervisor to share concerns or to ask for suggestions on how to handle difficult cases. Each PRC also had her supervisor’s and the perinatal psychiatrist’s cell phone numbers in her business phone should difficult situations suddenly arise.
Procedure
Participants agreed to meet quarterly for 1 year with PRC, who provided support, education on healthy lifestyle practices, and information on treatment and recovery resources. PRC helped connect participants to medication-assisted treatment (MAT) and behavioral and mental health providers within the network of referring clinics and recovery treatment centers. PRC utilized motivational interviewing and client-centered approaches to engage participants in an open, non-judgmental manner. Beyond the required quarterly meetings, the frequency, location (home, clinic, in the community) of meetings, phone calls and/or text messaging, and focus of the visit were individually determined between the participant and PRC. The average time per PRC-participant contact ranged from 15 to 30 min. PRC helped participants identify and follow through with personalized recovery goals and healthy behaviors related to their pregnancy, postpartum period, and parenting. Participants were given a $50 gift card for completing surveys at enrollment, and a $10 gift card for completing follow-up surveys. PRC also helped participants access free resources such as diapers and wipes, food, cribs, clothing, bus passes, and other personalized needs.
Data Collection
Written informed consent, demographics (including age, race/ethnicity, and gestational status) and contact information were obtained at intake. Data on substance use history (including tobacco and alcohol), history of childhood trauma, measures of treatment for motivation, and partner data (including abuse/violence, drug use, support of treatment, participation in treatment, and involvement in parenting) were collected at intake, 2, 6, 9, and 12 months. Validated survey tools were used to measure depression (HAM-D), 17 anxiety (HAM-A), 18 domestic abuse or interpersonal violence experience (Abuse Assessment Screen), 19 childhood trauma (Adverse Childhood Experience questionnaire) quantifying the number of adverse events experienced, 20 and readiness for treatment (Treatment Motivation Scale). 21 These and other validated survey tools used in the CARE study22, 23 are described in more detail elsewhere. 24 PRC read the survey questions to the participants and documented their responses in a secure Research Electronic Data Capture (REDCap) database. 25 PRC also documented field notes in the REDCap database summarizing the focus of each participant encounter.
Quantitative statistical methods
Chi-square test or Fisher’s exact test for comparison of categorical measures were used to test for differences between groups in the study (ie, Black, White, other). To achieve 80% power for a chi-square test with 8 degrees of freedom, a sample size of 167 would be required to detect a medium effect size (W = 0.30). 26 The observed sample of 251 has more than 80% power to detect medium effect sizes using the chi-square test for all planned outcomes.
Qualitative analytic methods
Qualitative analysis of all abstracted narrative entries (fieldnotes entered into the REDCap database by the PRC) was conducted using qualitative description.27,28 No data were collected using visual or audio recordings. Qualitative description involves coding data from narrative entries, identifying similar themes, looking for similarities and differences, deciding on groupings, and examining findings in the context of existing knowledge. 29 Authors (AY, WG, AW, SR, PD, DB, and DL; all female), who had no prior relationship with any of the participants, independently read through all narrative fieldnotes, generated preliminary codes, and resolved any discrepancies between initial codes, and agreed data saturation was achieved. A subset of the re-coded data was discussed by paired authors to ensure consistency in coding following the constant comparative method for developing coding schemes. 30 All authors had training in qualitative analytic methods; author pairings for coding purposely included both a health services research investigator and a research coordinator in each pair to balance level of experience.
Four emergent themes were generated using an iterative multi-step thematic content analysis. 31 Upon review and comparison with existing literature, the emergent themes matched the 4 types of support identified by SAMHSA and the facilitators and barriers of each, 1 including emotional, informational, instrumental, and affiliational. Authors also coded entries as either facilitators or barriers for each of the 4 types of support. Paired authors selected representative entries for each theme, which were reviewed by AY and DL to assess the fit and relevance before finalizing.32,33 Each quote was from a unique participant.
Narrative entries for each of the 4 support categories were broken into Group A and Group B based on the race of the participants. Blinded to the racial assignment for Group A and Group B, paired authors for each of the 4 support categories reviewed the entries for similarities, differences, and any other notable observations. Together, all paired authors reviewed coding for similarities and differences and were able to achieve full agreement on any initial discrepancies.
Results
Participants
A total of 251 women enrolled in the study (see Table 1). About half (47%) of the subjects were either pregnant or postpartum at the time of intake. The majority (78%) of the women were 26 to 35 years of age with ages ranging from 18 to 35+ years of age. Women in the study were predominately White (59%) or Black (39%). Participants self-reported their race during the initial intake session.
Demographic Characteristics.

Percentages may not sum to 100% due to rounding.
Survey data
Comparisons between White and Black participants showed no significant differences in age, gestational status, or in the pattern of intravenous substances. Statistical analyses comparing differences between survey responses by race revealed that White race women compared with Black women showed no significant differences in scores on the anxiety and depression scales, adverse childhood events, and experience of abuse at intake. Independent of race, scores on Ham-A, Ham-D, Abuse Assessment, and ACE document high percentages of women experiencing moderate-to-severe mental health challenges, domestic/interpersonal abuse, and past and/or ongoing trauma (see Table 2 for interpretation and distribution of scores for various levels of severity). However, White participants compared with Black participants were significantly more likely to be in treatment (P < .001); on medication-assisted treatment (MAT) (P < .001); and on Methadone (P < .006), Buprenorphine (15%vs 8%, NS), or other medications (P < .033) at intake. White women compared with Black women in CARE were significantly more likely to report being more motivated to engage in recovery treatment (P < .001). Despite being less likely to be receiving treatment, including lower use of MAT and reporting less motivation to engage in recovery treatment at intake, a greater percentage of Black women compared to White women were retained in the CARE Program at 2 months (P < .006), 6 months (P < .011), and 9 months (P < .004) (Table 2).
CARE Survey Data at Intake.

Only 2% of the study participants self-identified race as “other.” All the above analyses were run by dropping the “other category” participants and also collapsing “other” participant into “White” then “Black” categories; the results of these analyses did not change the findings.
Narrative Data
Emergent themes
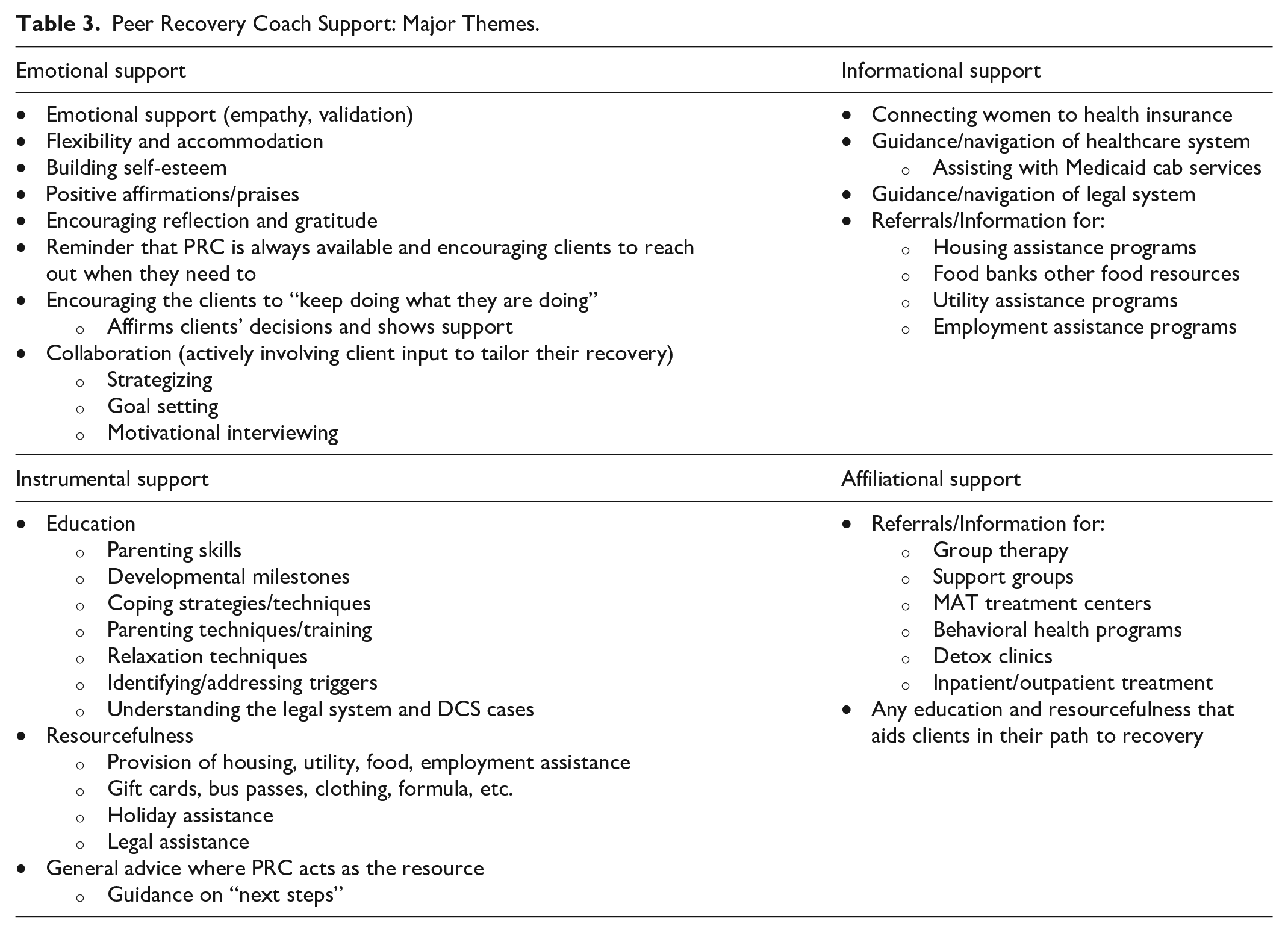
The PRC narrative entries were initially coded and mapped to the 4 types of support provided by PRC, as outlined by SAMHSA (Table 3).
1
Entries coded as
Peer Recovery Coach Support: Major Themes.
Barriers and facilitators to retaining women in CARE
Numerous facilitators and barriers to retaining women in CARE emerged from the analyses of the narrative entries (Table 4). CARE provided insight into the barriers participants faced including perceived stigma, counseling turnover at treatment centers, and pregnant women feeling “judged” by their providers or fearful of their children being taken away. CARE participants found CARE PRC to be highly relatable, because the PRC have personally experienced life challenges, such as being a single mother along with other insecurities, as well as having personal, lived experience with SUD.
Barriers and Facilitators to Retaining Women in CARE.

CARE exposed several weaknesses and lack of resources in our community, including dependable transportation to MAT providers; the lack of local MAT options (some clinics offered only Methadone treatment, and a scarcity of providers could prescribe Buprenorphine with/without Naloxone); the concern of patients being wait-listed for a treatment facility, and eventually changing their minds; and the lack of housing for pregnant moms and moms with infants (lack of beds, liability, barriers due to prior felonies or criminal involvement).
Key findings for 4 types of support
In general, the number of narrative entries for Black participants (Group B) as compared with White participants (Group A) were far more frequent, even though there were about 50% more White (n = 147) than Black (n = 97) participants. For each of the 4 areas of support, similarities, differences, and key observations with quotes exemplifying the differences between Group A and Group B entries are described below.
Emotional Support
Similarities
For all participants, PRC provided listening, congratulating, validating and positive affirmations as demonstrations of emotional support. They also offered their availability and encouraged participants to reach out as demonstrations of coach support.
Differences
The main differences in emotional support were seen in entries coded for the type of advice and encouragement PRC provided to participants. For Black (B) participants, the PRC offered advice and encouragement focused on boosting participants’ confidence and encouraging them to move forward. After such talks, participants sometimes responded in a positive manner.
The PRC followed by encouraging positive actions and then promoting self-advocacy.
These patterns in communication suggested the PRC expected the clients to take action and be involved in improving situations.
The PRC did encourage White participants to focus on goals, but there appeared to be less of an expectation for the participant to take action and/or ownership as compared to Black participants. Also, the PRC’s encouragement of the participant in Group A to self-advocate occurred less often than in Group B.
Instrumental Support
Similarities
For all participants, PRC provided items needed by participants (eg, items for baby [diapers, wipes, portable cribs, formula], mother [maternity clothing], bus passes, holiday/food assistance, household cleaning supplies, personal hygiene items), provided education (eg, on breastfeeding, safe sleep, smoking cessation, birth spacing, self-care and stress management, domestic and intimate partner violence, gun safety), and offered direct assistance (eg, pre-arranging transportation, appointment reminders, finding shelter and/or housing, contacting organizations on participant’s behalf).
Differences
The main differences in instrumental support were the more detailed entries about how to access needed items, messaging about potential consequences and accountability for a participant’s action, and direct assistance PRC provided to Black participants.
Informational Support
Similarities
For all participants, PRC provided information about resources for needed items [e.g., housing (low-income housing, shelters, rental assistance), employment (staffing agencies, job fairs, places hiring), baby needs (diapers, car seat, pack-n-play), food pantries, transportation (Medicaid cabs, Lyft, Uber, ways to get bus passes), healthcare needs (locating healthcare facilities, encouraging follow-up appointments)].
Differences
PRC provided more detailed guidance to participants when sharing both general and employment resources with Black participants.
Entries for Black participants more often proactively asked about and offered to explore or provide information compared with entries for White participants.
The wording in entries for Black women more frequently included encouraging messages.
Affiliational Support
Similarities
For all participants, PRC considered participant’s input when discussing treatment decisions (e.g., PRC provided multiple options and determined willingness for treatment), helped identify triggers for substance use and address underlying mental health conditions, advocated for the participants, walked participants through the treatment process, provided a “hands-on” approach, and encouraged participants to reach out to providers.
Differences
The main differences in affiliational support were the more detailed entries about treatment options and resources to mitigate barriers to engaging in treatment (e.g., locations and phone numbers for treatment centers and obtaining MAT, times and place for Alcoholics Anonymous and Narcotics Anonymous meetings). Differences between groups were also reflected in conversations on triggers to using, explaining delays when seeking help, and directing communications with behavioral health and medical providers when needed.
Discussion
Our findings support that PRC are key members of effective SUD treatment and recovery programs particularly for women of childbearing age. Our qualitative analyses of field note entries validated the key roles, responsibilities, and types of support characteristic of effective PRC as defined by SAMSHA. 34 CARE PRC repeatedly demonstrated a high level of competency in delivering all 4 types of support, addressing common barriers, and promoting facilitators to achieve personal goals toward recovery.
In contrast to the fear of being shamed and judged by traditional health care providers, 10 the participants and PRC were able to connect through their shared experiences and develop a trusting relationship. Literature suggests that traditional health providers tend to less proactively address the many social and structural determinants of health and/or provide passive referrals, 12 whereas CARE PRC embraced these as part of their primary roles. PRC allowed participants to focus encounters on their highest priorities, which often included secure housing, food, diapers, or safety from interpersonal violence, before the focus could turn to other aspects of SUD treatment and recovery.
Quantitative analyses of our data at intake documented that, irrespective of race, women enrolling in the CARE program were experiencing a high prevalence of moderate-to-severe anxiety, moderate-to-very severe depression, high scores on experiences of ACE, and past or ongoing interpersonal violence relative to the general population (refer to scores in Table 2). 35 The high prevalence of these co-morbid conditions in association with persons experiencing SUD, as well as racial differences found in our intake data, are consistent with previous findings. 36 We found that Black women were less often in treatment, which may be related to reports of perceived stigma. 11 The literature reports that Black patients have described treatment for SUD as being reserved for criminals, labeled addicts, and homeless individuals. Patients saw that treatment served as a “marker” indicative of needing help and revealing a true problem.
Prior studies found fear of recognition within Black women’s communities remained a barrier to seeking out treatment; they were more willing to attend a specialty treatment program not outwardly identified as a service for individuals with SUD. 9 Perceived social support was also a barrier for Black patients, where they felt less inclined to disclose details of treatment with family members and friends for support, though this was attributed to success in treatment by White patients. 9
We found that Black women reported less motivation to seek treatment at intake. In a retrospective study of 16,939 patients who were enrolled in SUD specialty treatment facilities, rehabilitation centers, and mental health services, only 18% of patients perceived a need for treatment. 9 Factors that lead to an increased perceived need for treatment included greater problem severity, symptoms of mental distress within the last year, and co-occurrence of alcohol and illicit drug use disorders. 9 Black participants were less likely to report any contact with traditional health providers within the last year which corresponded to lower rates of perceived need for treatment.
Despite fewer Black women being in treatment and reporting lower motivation for engaging in recovery programs, we were encouraged to find that more Black women were retained in the CARE program even 9 months after enrollment. Black women’s reluctance to disclose their SUD to providers and fear of stigma may result in less engagement with more traditional treatment recovery programs, leaving peer recovery programs as a more viable option. PRC implementation can occur in many stages of the treatment algorithm, including linkage to care, retention in programs, and remission. Studies have shown that PRC implementation in SUD treatment found significant reductions in opioid overdose, adherence to drug abstinence, and higher meeting attendance in 12-step meetings. 37
Evidence also supports the importance of racial and gender concordance between health care providers and patients to optimize patient experience ratings. 38 Racial identity has been shown to influence the effectiveness of CHW interventions with Black adults. 39 We believe that the racial and gender concordance between our CARE PRC and participants may have contributed to the retention in the CARE Program, although closer analysis of pairings of PRC-participant’s race is ongoing .
Careful qualitative analyses of the PRC narrative entries also shed light on possible reasons for racial differences in retention. Key differences were noted in all 4 types of support as defined by SAMHSA.
34
While
The
Overall, the CARE program was unique in its structure with the intentionality and long-term commitment of the PRC in assisting each participant. The amount of time PRC had with women in the program was especially important, which is evidenced by the number of women who remained engaged in CARE for up to 12 months. Some participants took several months to build enough trust to fully engage with PRC. Retention of clients was often difficult, as they were frequently transient and/or had changed their phone numbers, but the PRC were flexible in working with the clients to meet their level of need. It became evident that there were different styles of preferred communication among the population with whom we worked. Most preferred meeting face-to-face, while some preferred to communicate through text messages or phone calls. Others responded or re-engaged through short written notes left for the participants at their treatment centers. This level of involvement by CARE PRC allowed the opportunity to learn about the resiliency of many participants overtime. We saw many women who became self-advocates making changes in family structure/lifestyle, changing treatment centers, requesting lower doses of Methadone, or deciding to completely stop using a specific substance that was causing harm in their lives.
Limitations
Although longer retention of Black women in a PRC program is an important outcome, a limitation of this study is lack of objective documentation of abstinence. However, of note, many women remained with their infants, few delivered infants with neonatal abstinence syndrome, and there were no overdose fatalities during the study period. More analyses are also needed to better understand any differences in racial concordance or discordance between PRC and participant pairs; these analyses are underway. This study was conducted in an urban setting, so results may not be applicable to other settings.
Conclusion
The inclusion of PRC as integral members of SUD recovery programs may preferentially provide Black women with SUD the opportunity to build more trusting relationships with these peer coaches, thereby increasing their participation and retention in SUD-related treatment.
Footnotes
Acknowledgements
We thank Donna Burgett, Justina Savage, and Melissa Thomas with their assistance with preparing the manuscript for submission.
Data Availability
Data are stored in a secure REDCap database. Requests for access to the data can be made to the corresponding author.
Declarations,Ethics,and Consent Statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Written informed consent, demographics (including age, race/ethnicity, and gestational status) and contact information were obtained at intake.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded, in part, with support from the Indiana Clinical and Translational Science Institute, in part by UL1TR002529 from the National Institutes of Health, and, in part, with support from the Fairbanks Foundation and the IU Addictions Grand Challenge.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the funding organizations.
Institutional Review Board
This study was approved by Indiana University Institutional Review Board as an expedited level of review (IRB Protocol #: 1808974969). Study Information Sheets describe the purpose for doing this research.