
Abstract
The retrospective study aimed to describe the epidemiological characteristics and trends of cancer in Anhui Province, China between 2010 and 2018. Cancer registry data were analyzed using the Joinpoint regression model to calculate trends in cancer incidence and mortality. Age-standardized incidence rate, calculated based on the world Segi’s population (ASIRW) was higher in males (239.34 per 100 000) than in females (157.13 per 100 000), and higher in rural areas (203.98 per 100 000) compared to urban areas (189.93 per 100 000). The ASIRW for males decreased with an AAPC of −3.0%, while that of females showed an upward trend with an AAPC of 2.1%. At the same time, the ASIRW in urban areas decreased with an AAPC of −2.4%, whereas it remained relatively stable in rural areas. Among males, lung cancer was the most prevalent type of cancer, while breast cancer was the most frequent cancer among women. The age-standardized mortality rate according to the world Segi’s population (ASMRW) was 115.32 per 100 000. The ASMRW was higher in males (156.70 per 100 000) than in females (75.51 per 100 000), and higher in rural areas (122.18 per 100 000) than urban areas (109.21 per 100 000). Lung cancer accounted for the majority of cancer-associated mortalities in the province. Attention needs to be focused on women and rural areas due to rapidly increasing incidence and mortality rates for cancer. Furthermore, an effective public health response is imperative, encompassing early screening, diagnosis, and treatment of prevalent cancers in high-risk populations and regions. It’s crucial to promote healthy lifestyles among the public through health education.
The burden of cancer was rapidly growing nationwide, including China, over the past decades.
This study describes the spectrum of tumors and their changing trends in Anhui Province, China.
There is an urgent need to focus more on females and rural areas in Anhui Province due to the alarming rise in cancer incidence and mortality rates.
Introduction
Cancer is a prominent cause of death and a significant obstacle to increasing life expectancy worldwide, posing a major public health concern.1,2 The latest cancer statistics report estimates that there were an estimated 19.29 million new cancer cases and 9.96 million cancer deaths occurred worldwide in 2020. 3 With China accounting for one-fifth of the world’s population, the country faces unprecedented cancer control challenges due to population aging and socioeconomic development. The Global Cancer Statistics estimates revealed that there were about 4.51 million cancer cases and 3.04 million cancer deaths in China in 2020. 4 Furthermore, the incidence and mortality rates of cancer have been rapidly increasing nationwide over the past decades. 5
The National Cancer Center Registry of China (NCCRC) was established in 2002. It has the responsibility for collecting, evaluating and publishing national cancer statistics from local population-based cancer registries across China. Subsequently, the national program of cancer registry was launched by the Ministry of Health in 2008. As of July 2019, there were 574 local population-based cancer registries, covering approximately 438 million people, which accounts for approximately 31.5% of the total national population. 6 High-quality and representative national cancer registry data can demonstrate the country’s cancer burden and play a critical role in identifying health priorities and monitoring progress in cancer control. Anhui Province, a southeastern province of China, has established a cancer registration framework, as part of the national registry. This paper aimed to provide an updated overview of cancer burden in this area by utilizing continuous data from cancer registries during 2010 to 2018. Additionally, new information on trends in cancer incidence and mortality can offer valuable evidence for designing and evaluating provincial cancer control programs.
Materials and Methods
Cancer Registry Data Sources
Located in southeast China, Anhui Province governs 16 Prefecture-level cities and covers an area of 140 100 km2. With a population of 61.13 million, representing 4.32% of China’s total population, the province has established a cancer registration framework. Cancer data in Anhui Province were collected from local registries through multiple sources, including hospitals, community health centers, insurance programs and the new-rural cooperative medical system. All cancer cases were coded according to the “International Classification of Diseases 10th Revision” (ICD-10). The statistical data on cancer has been publicly available through the Anhui Cancer Registration Annual Report since 2013. For the study, we utilized a consolidated database spanning 9 years, extracted from the 2013 to 2021 Anhui Cancer Registry Annual Reports. Please note that there was a 3-year delay between the data collection and publication.
Over the 9-year period, the cancer registries covered a population of 171 831 368 person-years, which accounted for approximately 27.72% of the population in Anhui Province. Specifically, it included 88 045 388 males and 83 785 980 females. The number of cancer registries increased from 12 in 2010 to 34 in 2018. Although population fluctuations from 1 year to the next may affect incidence and mortality rates, the improved coverage and the expansion of cancer registries have increased their representativeness. In 2018, a total of 40 cancer registration offices in Anhui Province reported cancer registration data. Of which, 34 offices met the data quality evaluation standards. According to national standards of cancer area classification, cities are classified as urban areas while other areas are classified as rural areas. There were 12 urban cancer registries and 22 rural cancer registries. Based on the distribution of cancer registries, Hefei City had the largest population coverage under cancer registration, whereas Huangshan City had the smallest population coverage (Figure 1).
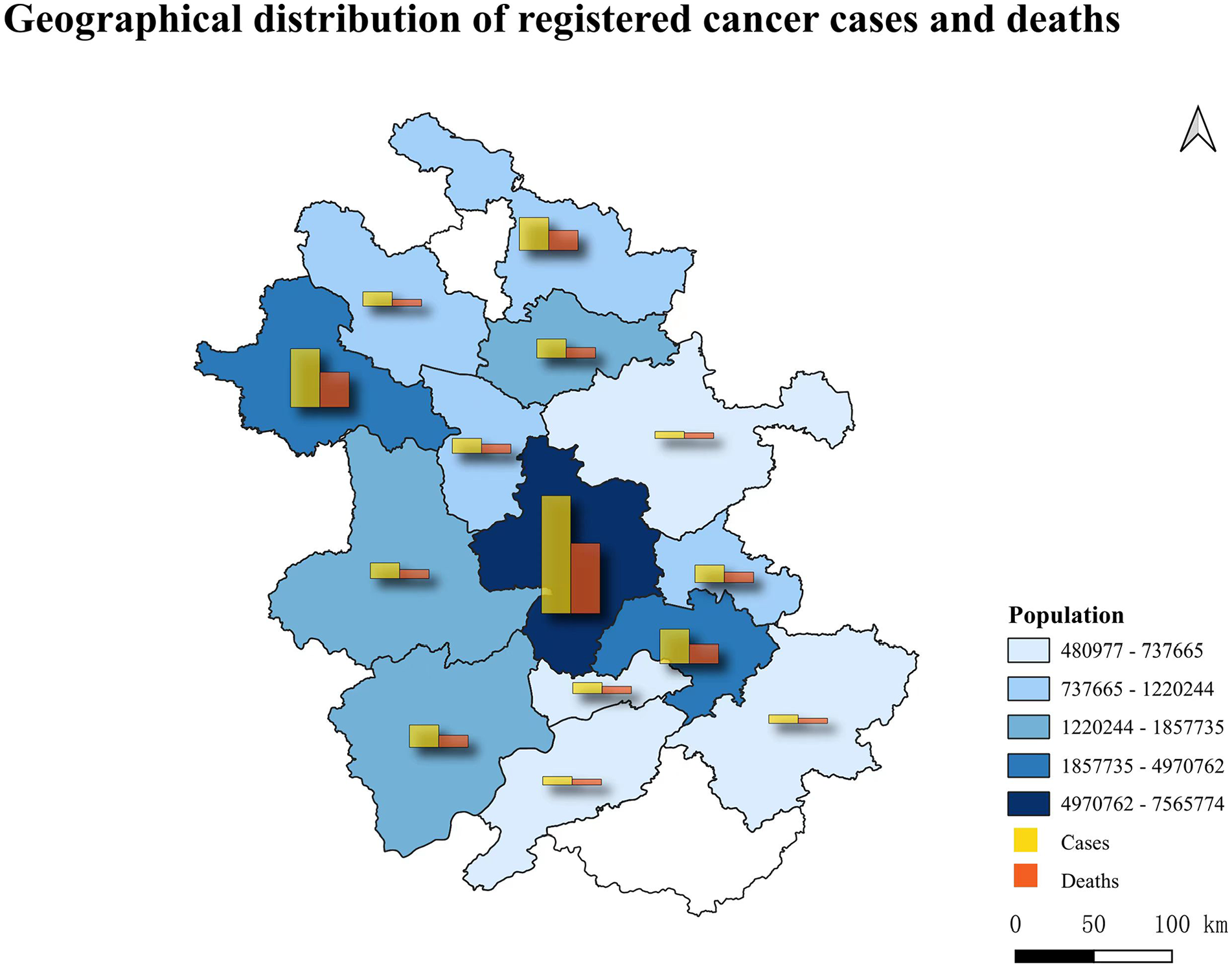
Geographical distribution of the population-based cancer registries in Anhui Province, China.
Data Quality Control
Data quality was assessed following the guidelines outlined in the “Guideline for Chinese Cancer Registration” 7 and “Cancer Incidence in Five Continents Volume IX” 8 issued by the International Agency for Research on Cancer/International Association of Cancer Registration (IARC/IACR). Data validity was assessed by calculating the percentage of cases morphologically verified (MV%) and death certificate-only cases (DCO%). Meanwhile, the completeness of data was assessed by the mortality to incidence (M/I) ratio.
Statistical Analysis
The data for this study were obtained from 2013 to 2021 Anhui Cancer Registry Annual Reports and entered into a Microsoft Excel database. Statistical analysis was performed using Joinpoint Regression Software version 4.9.0.0 (SEER*Stat, Bethesda, MD, USA). 9 The age-standardized rates per 100 000 by world standard population (Segi’s population) of incidence and mortality were calculated, and further stratification of the rates by gender, region (urban/rural), age, and cancer types was performed. Temporal trends during the study period were measured using the Joinpoint model to calculate the Annual Percentage Changes (APC) and Average Annual Percentage Changes (AAPC). APC values greater than zero indicated an upward trend, while values lower than zero indicated a downward trend. A P < .05 was considered statistically significant.
Results
Data Quality
This study estimated a total of 1 620 231 new cases of cancer, of which 973 997 were males and 646 235 were females. Additionally, approximately 980 229 cancer deaths due to cancer were reported in Anhui Province during the study period. The MV%, DCO%, and M/I were 62.13%, 0.92%, and 0.59, respectively.
Cancer Incidence and Mortality
During the study period, the age-standardized incidence rate by the world Segi’s population (ASIRW) was 197.48 per 100 000 and was further stratified by gender and region. The ASIRW was higher in males (239.34 per 100 000) than in females (157.13 per 100 000) and it was also higher in rural areas (203.98 per 100 000) than in urban areas (189.93 per 100 000). The male ASIRW showed a downward trend (AAPC = 2.4%, P < .05), while the female ASIRW increased with an AAPC of 2.1%. Meanwhile, the male-female incidence ratio decreased from 1.79 in 2010 to 1.26 in 2018. The incidence rate in urban areas decreased from 194.90 per 100 000 in 2010 to 175.73 per 100 000 in 2018, with an AAPC of −2.4%, while the incidence trend in rural areas was relatively stable. The urban-rural incidence ratio decreased from 1.09 in 2010 to 0.90 in 2018 (Table 1).
The Number and Age-Standardized Rate of Cancer in Anhui, China From 2010 to 2018.

Note. ASR = age-standardized rate per 100 000 by world standard population (Segi’s population); AAPC = the average annual percent change; APC = the annual percent change.
Indicate that the AAPC or APC is significantly different from zero at the alpha = .05 level.
The age-standardized mortality rate by the world Segi’s population (ASMRW) during the study period was 115.32 per 100 000 and was further stratified by gender and region. The ASMRW was higher in males (156.70 per 100 000) than in females (75.51 per 100 000) and higher in rural areas (122.18 per 100 000) than in urban areas (109.21 per 100 000). The mortality trends of both men and women were relatively stable, with women showing a slight upward trend. The male-female mortality ratio decreased from 2.15 in 2010 to 1.98 in 2018. The ASMRW in urban areas showed a significant downward trend, with an average annual decline of 3.4%, while the mortality rate in rural areas showed an upward trend. The urban-rural mortality ratio decreased from 1.33 in 2010 to 0.87 in 2018 (Table 1).
Age-Specific Incidence of Cancer
The age-specific incidence of cancer was relatively low among individuals under 45 years of age, with a significant increase thereafter. The age-specific incidence peaked at 1561.97 per 100 000 in the group aged 80 to 84 years, while the highest number of cases was reported in the group aged 65 to 69 years (218 515 cases). Furthermore, the age-specific incidence was stratified by gender and region, revealing lower incidence among males than females in individuals aged 15 to 54 years but the opposite trend in those over 55 years old. The gender difference increased gradually in the groups aged 55+ years old. In addition, the age-specific incidence in rural areas was higher than that in urban areas in most age groups before 55 years old, while the opposite was true for individuals over 55 years old (Figure 2).

Age-specific rates of incidence for all cancers in Anhui during 2010 to 2018.
Age-Specific Mortality of Cancer
The age-specific mortality of cancer was low among individuals under 45 years old before increasing rapidly. The age-specific mortality peaked at a value of 1552.27 per 100 000 among individuals aged 85 years old and above, while the highest number of deaths occurred in the group aged 75 to 79 years (148 085 cases). Of all cancer-related deaths, over 66.4% were reported among individuals aged over 65 years old. The results showed that the age-specific mortality in males was higher than that in females in all age groups with the male-female mortality ratio gradually increasing with age. In contrast, the age-specific mortality in rural areas was higher than that in urban areas, excluding individuals aged 5 to 9 years old. More details of the age-specific mortality of cancer are summarized in Figure 3.

Age-specific rates of mortality for all cancers in Anhui during 2010 to 2018.
Temporal Trend Analysis of Top 10 Cancer Incidence
The temporal trends analysis of incidence for the top 10 cancer was presented in greater details in Table 2. Among the top 10 most common cancer types, lung cancer and breast cancer were the most frequently occurring in males and females, respectively. Additionally, lung cancer was the most common cancer in both urban areas and rural areas. The top three to six common cancer types were cancers of digestive tract, including gastric, liver, colorectal, and esophageal cancers. The ASIRWs for breast, cervical, and thyroid cancers increased significantly (all P < .05), with thyroid cancer having the fastest increase with an AAPC of 26.4%. However, the ASIRWs for gastric and esophageal cancers decreased significantly (all P < .05).
Trends of Age-Standardized Rates of Incidence for Selected Cancers in Anhui During 2010 to 2018.

Indicate that the AAPC is significantly different from zero at the alpha = .05 level.
In males, the ASIRW for thyroid cancer increased significantly with an AAPC of 25.0% (P < .05), while the ASIRWs for gastric and esophageal cancers decreased significantly (all P < .05). In females, the temporal trend analyses showed significant increases in the ASIRWs for breast, thyroid, cervical, uterus, and brain cancers (all P < .05), while the ASIRWs for gastric and esophageal cancers decreased significantly (all P < .05). However, there were no significant changes for lung, colorectal, and liver cancers in females was stable over the years.
In urban areas, the ASIRWs for thyroid, cervical and prostate cancers increased significantly (all P < .05), while the ASIRWs for lung, gastric, liver, and esophageal cancers decreased significantly (all P < .05). Conversely, there were no significant changes in the ASIRWs for breast and colorectal cancers among those living in urban areas. In rural areas, the ASIRWs for breast, colorectal, cervical, thyroid, brain, and uterus cancers significantly increased (all P < .05), while the ASIRWs for gastric and esophageal cancers decreased significantly (all P < .05). Conversely, the ASIRWs for lung and liver cancers in rural areas were stable over the years.
Temporal Trend Analysis of Top 10 Cancer Mortality
Details on the temporal trends and the Joinpoint analysis of the top 10 cancer mortality were summarized in Table 3. Among the top 10 cancers, lung cancer was the leading cause of cancer-related deaths in the province. The ASMRWs for breast and cervical cancers increased significantly (all P < .05), while other top 10 cancers did not experience significant changes.
Trends of Age-Standardized Rates of Mortality for Selected Cancers in Anhui During 2010 to 2018.

Indicate that the AAPC is significantly different from zero at the alpha = .05 level.
The ASMRWs for leukemias in males and female cancers, including breast, cervical and ovarian cancers, showed significant upward trends (all P < .05). Among those living in urban areas, the ASMRWs for cervical and ovarian cancers increased significantly (all P < .05), while the ASMRWs for lung, gastric, liver, and esophageal cancers decreased significantly (all P < .05). In rural areas, the ASMRWs for breast, cervical cancers, and leukemia increased significantly (all P < .05), while the ASMRWs for other cancer types were stable in rural areas during the study period.
Discussion
This study presents, for the first time, a comprehensive analysis of cancer trends in Anhui from 2010 to 2018 by utilizing population-based cancer registries data. The findings provide an up-to-date overview of the current cancer burden and offer valuable insights for informing evidence-based cancer prevention and control policies in the region.
During the period of 2010 to 2018, the burden of cancer incidence and mortality witnessed a rapid increase in the province, exhibiting significant heterogeneities. In comparison to the updated national cancer data, 10 the provincial level experienced a slightly higher disease burden (ASIRW: 197.48 per 100 000, ASMRW: 115.32 per 100 000) than the national level (ASIRW: 186.39 per 100 000, ASMRW: 105.84 per 100 000). Furthermore, when compared to developed regions like Shanghai (ASIRW: 211.27 per 100 000, ASMRW:105.44 per 100 000) and Guangdong (ASIRW: 201.34 per 100 000, ASMRW: 102.44 per 100 000), the province exhibited lower cancer incidence rates but higher mortality rates.11,12 It is worth noting that cancer incidence and mortality were higher among males and rural areas than females and urban areas, respectively. Moreover, there was an increase in the cancer burden for women and rural residents, while men and city residents experienced a decline. These disparities can be attributed to variations in living habits, healthcare level, physiology, and socioeconomic development. 3 Finally, the findings reveal that lung cancer was the most common cancer among males, breast cancer was predominant in females, and lung cancer was also identified as the leading cause of cancer-related deaths for both genders, in line with national data. 10
Over the past few decades, lung cancer has remained the most prevalent form of cancer and the leading cause of cancer-related deaths worldwide, irrespective of gender. 1 This pattern is also observed in Anhui Province, where it has contributed significantly to the overall disease burden.10,13 Within the province, tobacco use is the primary factor contributing to roughly 2.5 times higher incidence and mortality rates of lung cancer in men compared to women. 14 The United States provides a successful model for lung cancer prevention and control, that is replicable. 15 By implementing smoke-free environments and undertaking low-dose computed tomography (LDCT) screening for individuals at high risk, the US has managed to achieve a decline in lung cancer incidence and mortality rates. 16 This achievement serves as an inspiration when confronted with similar challenges.
The top 3 to 6 common cancers are gastric, liver, colorectal, and esophageal cancers in Anhui Province, which are infection-related and poverty-related cancers. These cancers are associated with unhealthy lifestyles, such as alcohol consumption, 17 pickled foods, 18 eating hot food, 19 and chronic infectious agents. 20 In order to address this public health concern, the Huaihe Valley Cancer Early Diagnosis and Treatment Program has been providing screening services for upper gastrointestinal and liver cancers in Anhui Province since 2007. The study observed a slight decrease in the incidence of these cancers. In the future, it is recommended to implement universal cancer screening services and promote healthy lifestyle choices among the general public as an efficient solution.
Additionally, there has been a rapid growth in the disease burden of cancers associated with the westernization of lifestyle, specifically colorectal and breast cancers, which are commonly linked to the increasing prevalence of overweight and obesity in the population. 21 The prevalence of overweight and obesity has been increasing significantly among the Chinese population. 22 In the coming decade, greater efforts should be focused on promoting a balanced diet and physical activity in order to control the rising incidence of colorectal and breast cancers.
It should be noted that the ASIRWs for breast, cervical and thyroid cancers in females increased significantly. Meanwhile, the ASMRWs for breast, cervical and ovarian cancers in females also showed upward trends. This highlights the urgent need to prioritize females in the development of cancer control programs. For example, human papillomavirus (HPV) infection is the most important risk factor for the occurrence of cervical cancer, 23 which can effectively be prevented through HPV vaccine. 24 The World Health Organization (WHO) reported that 80% of coverage of the target population with Pap screening and an organized network for adequate diagnosis and treatment would allow a 60% to 90% reduction in cervical cancer. 25 Therefore, the implementation of HPV vaccination, early screening, accurate diagnosis, and effective treatments can help reduce the incidence and mortality of cervical cancer.
Finally, cancer incidence and mortality rates were higher in rural areas than those in urban areas in Anhui Province. The heterogeneity may be primarily attributable to differences in exposures to carcinogens, lifestyle, and different health resources. In 2016, the Chinese government has issued an ambitious blueprint for “healthy China 2030” aimed at improving the nation’s health. 26 The implementation of this blueprint may help reduce the disparity in cancer burden between urban and rural areas by providing better access to healthcare services. 27
The current study had several limitations. The study had limited coverage of the cancer registry areas, potentially resulting in deviations in the cancer trend analysis. Additionally, there is a lack of available information on factors such as survival time, cancer staging, exposure, etc. Moreover, the quality of cancer registry data still needs to be improved.
Conclusion
During the study period, Anhui Province exhibited a cancer spectrum similar to the national cancer data, indicating a shift toward a more “westernized” cancer spectrum. There was an evident increase in the disease burden of cancer in this region. It is imperative to focus on the female population and rural areas, as they experienced a greater rise in cancer incidence and mortality rates. Moreover, lung cancer and gastrointestinal cancer, particularly colorectal cancer, displayed an increasing trend in both incidence and mortality rates during the study period. Therefore, prevention and intervention strategies for colorectal cancer should be prioritized in this region.
In conclusion, Anhui Province still faces significant challenges in effectively preventing and controlling cancer. Addressing these challenges necessitates a comprehensive public health response that includes early screening, diagnosis, and treatment of common cancers in high-risk populations and areas. Additionally, promoting a healthier lifestyle through health education initiatives for the broader public is essential.
Research Data
sj-xls-1-inq-10.1177_00469580231195311 – Supplemental material for The Increasing Burden of Cancer Among Women and in Rural Areas: A Retrospective Population-Based Study
sj-xls-1-inq-10.1177_00469580231195311 for The Increasing Burden of Cancer Among Women and in Rural Areas: A Retrospective Population-Based Study by Dan Dai, Lingfeng Xu, Shuowen Fang, Zhenqiu Zha, Huadong Wang, Zhirong Liu and Manman Lu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xls-2-inq-10.1177_00469580231195311 – Supplemental material for The Increasing Burden of Cancer Among Women and in Rural Areas: A Retrospective Population-Based Study
Supplemental material, sj-xls-2-inq-10.1177_00469580231195311 for The Increasing Burden of Cancer Among Women and in Rural Areas: A Retrospective Population-Based Study by Dan Dai, Lingfeng Xu, Shuowen Fang, Zhenqiu Zha, Huadong Wang, Zhirong Liu and Manman Lu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors are grateful to all the staffs of cancer registries in Anhui province for their support and excellent work. The authors take full responsibility for data analysis and result interpretation of this article. Zhirong Liu and Manman Lu: Conceptualization, Methodology; Dan Dai and Lingfeng Xu: Writing-Original draft preparation; Shuowen Fang and Lingfeng Xu: Software and Data curation; Huadong Wang Supervision; Zhenqiu Zha: Writing- Reviewing and Editing. All persons who have made substantial contributions to the work reported in the manuscript, including those who provided editing and writing assistance. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was also funded by the National Natural Science Foundation of China [grant number 71804002].
Ethics Committee Approval
Ethical approval was sought and obtained from Anhui Medical University Biomedical Ethics Committee (approval date: March 1, 2018 [serves as the Ethics Approval Reference Number]).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.