
Abstract
The composition of influenza vaccines is updated annually. To ensure vaccine safety, the coverage and adverse events following immunization (AEFI) of 6 manufacturers of trivalent inactivated influenza vaccine (TIV3) need to be evaluated. In January 2022, we analyzed data from more than 1.59 million children in the Childhood Vaccination Information Management System and the AEFI Surveillance Information Management System and evaluated influenza vaccines for children aged 6 to 35 months in Guangzhou from 2016/17 to 2019/20 Vaccination rates and AEFI reporting rates. From 2016/17 to 2019/20, the 1-dose influenza vaccination rate was 25.0% (range: 20.7%-30.2%), and the 2-dose (full course) influenza vaccination rate was 21.6% (range: 17.7%-26.4%). The full vaccination coverage rate has trended down since 2017/2018 (2017/18: 26.0%; 2018/19: 8.3; 2019/20: 17.7%). Fifty-two cases (13.1/100 000) and 24 cases (6.9/100 000) received AEFI reports for 1 dose and 2 doses, respectively, mainly due to fever ≥38.6°C (39 cases for 1 dose, 9.8/100 000; 15 cases for 2 dose, 4.3/100 000) and allergic rash (9 cases with 1 dose, 2.3/100 000; 5 cases with 2 doses, 1.4/100 000). Patients who received A and F manufacturers were more likely to report side effects. The safety of influenza vaccines from 6 manufacturers is good, and it is necessary to improve the recommended information on influenza vaccines to dispel people’s concerns and increase the vaccination rate.
Influenza vaccine coverage among children is low in most countries. Most of the reasons are that the children’s parents and doctors are worried about the effectiveness of the influenza vaccine and the serious adverse events, and their willingness to vaccinate is not high.
We monitored the vaccine safety of 6 manufacturers, and the results showed that the vaccine safety of 6 manufacturers was good. We hope that by publishing these results, people’s concerns will be reassured, the vaccination rate will be increased, and the goal of influenza control will be achieved.
Provide a basis for policy formulation and increase the coverage of influenza vaccination; it is suggested that when the government purchases vaccines, it should avoid those seriously affected by AEFI.
Introduction
Influenza is a respiratory infectious disease caused by the influenza virus, which is contagious and infects all age groups. 1 It is estimated that 291 243 to 645 832 people worldwide die from seasonal influenza-associated respiratory diseases every year. 2 Acute lower respiratory infection (ALRI) is one of the leading causes of childhood morbidity and mortality worldwide. In 2018, there were approximately 10 million cases of influenza virus-associated ALRI in children under 5 years old, approximately 870 000 patients with influenza-associated ALRI were hospitalized, and 15 000 died of influenza-associated ALRI in the hospital. 3 A study on the influenza virus infection rate in children during the 2018 to 2019 epidemic season in northern China found that the overall infection rate of seasonal influenza in children (31%) and the infection rate of the A (H3N2) subtype (17%) were significantly higher than the adult infection rate (21%, 10%). 4 Influenza has become a serious public health problem. Vaccination is an effective and cost-effective way to prevent influenza. 5 However, those with higher income levels are concerned about the number of adverse events and do not want their children to be vaccinated against influenza. 6 To address people’s concerns, in January 2022, we evaluated the vaccination rate and AEFI of TIV3 from 6 manufacturers in Guangzhou, China. Through the results of adverse events after immunization with vaccines from different manufacturers, we dispelled people’s concerns about vaccine adverse reactions and improved vaccine willingness; it also provides a basis for policy formulation and improving influenza vaccination coverage; it is recommended that the government avoid purchasing vaccines that are seriously affected by AEFI.
Materials and Methods
Study Design and Participants
This was a retrospective study. We analyzed the records of more than 1.59 million children in each influenza vaccination season (1 October-30 June) from 2016/17 to 2019/20. During each influenza vaccination season, children aged 6 to 35 months were included for analysis. Vaccination and AEFI data were obtained from the Guangzhou Vaccination Information Management System and the China AEFI Surveillance Information Management System, respectively. The data involve 11 districts in Guangzhou, including Baiyun (urban-rural integration area), Conghua (urban-rural integration area), Huadu (urban-rural integration area), Haizhu (central area), Huangpu (urban-rural integration area), Liwan (central area), Nansha (urban-rural integration area), Panyu (urban-rural integration area), Tianhe (central area), Zengcheng (urban-rural integration area), and Yuexiu (central area); a total of 742 314 doses of vaccines were administered (1 dose: 396 018 people, 2 doses: 346 296 Humans), and 76 doses of AEFI occurred (1 dose: 52 people, 2 doses: 24 people). The flow chart of the study is shown in Figure 1.

Flowchart of the samples in this study.
TIV3 Vaccination Procedures and Manufacturers
Six manufacturers were supplying the TIV3 vaccine from 2016/17 to 2019/20: Dalian Aleph Biomedical Co., Ltd. (Manufacturer A), Shanghai Institute of Biological Products Co., Ltd. (Manufacturer B), Sinovac Biotech Co., Ltd. (Manufacturer C), Hualan Bioengineering Co., Ltd. (Manufacturer D), Changchun Institute of Biological Products Co., Ltd. (Manufacturer E), and Shenzhen Sanofi Pasteur Biological Products Co., Ltd. (Manufacturer F). TIV3 vaccine components contain a strain of A (H3N2) subtype, A (H1N1) subtype and B strain, suitable for infants aged 6 to 35 months, 0.25 ml dosage form, containing 7.5 hemagglutinin for each component µg, in 2 doses with an interval of ≥4 weeks. Recipients can voluntarily receive any influenza vaccine with no prior recommendation. 7
AEFI Monitoring System
AEFI classification
According to the report scope of the «National Surveillance Program for Suspected Abnormal Vaccination Reaction» (Disease Control [2010] No.94), 8 the safety of influenza vaccines is divided into 5 categories: adverse reactions, vaccine quality accidents, vaccination accidents, coupling reactions, and psychogenic response. Adverse reactions are divided into general reactions and abnormal reactions. A general reaction refers to a reaction that only causes short-term physiological dysfunction of the body, mainly heat, redness, swelling, and hardening at the inoculation site; an abnormal reaction refers to a reaction that causes damage to human tissues, organs, and functions. Vaccine quality accident: Due to the unqualified quality of the vaccine, the recipient’s tissues, organs, and bodily functions are damaged after vaccination. Vaccination accident: Due to the violation of vaccination work specifications, immunization procedures, vaccine use guidelines, and vaccination schemes during the implementation of vaccination, the tissues, organs, and functions of the recipients are damaged. Coincidental disease: the recipient is in the incubation period or prodromal period of a certain disease at the time of vaccination, and the disease happens by chance after vaccination. Psychogenic reaction: the individual or group reaction that occurs due to the psychological factors of the recipient during the implementation of vaccination or after vaccination.
AEFI Investigation and Diagnosis
Suspected reports of abnormal vaccination reactions are subject to localized management. Medical institutions and vaccination units shall fill out the case report card for suspected abnormal vaccination reactions within 48 h of discovering suspected abnormal vaccination reactions and report to the county-level disease prevention and control institution where the recipient is located. Organize the investigation within 48 h after the report and conduct a direct network report through the national vaccination information management system within 3 days after the investigation begins.
Statistical Analysis
The data were collected using Microsoft Excel files, and IBM SPSS Statistics 27.0 statistical software was used for data analysis to calculate the vaccination rate. The results were displayed as a 95% confidence interval (CI) to calculate the incidence of AEFI. The influenza vaccination rate (%) is the number of people vaccinated against influenza/total population of the age group × 100. The denominator refers to the total population of children (6-35 months), which is obtained from the 2016 to 2019 annual report of legal infectious diseases in Guangzhou; the numerator refers to the number of children (6-35 months) who have been vaccinated. The AEFI reported incidence rate (100 000 doses) is the number of AEFI reported cases/number of influenza vaccinations × per 100 000 doses. For all analyses, chi-square analysis was applied, and data were considered statistically significant when a P value was less than 0.05.
Result
Influenza Vaccination in Children
Overall trends in influenza vaccination coverage
As shown in Table 1, the influenza vaccination rate showed a downward trend year by year, with the highest rate of full (2 doses) vaccination in 2016/17 being 26.4% (95% CI: 26.3%-26.7%), followed by 26.0% (95% CI: 25.9%-26.4%) in 2017/18, 18.3% (95% CI: 18.2%-18.5%) in 2018/19 and 17.7% (95% CI: 17.5%-17.9%) in 2019/20 (Table 1). Both vaccination rates were >17.7%, but compared with 2017/18, the number of vaccinations in 2018/19 to 2019/20 decreased by 27.8% and 12.94%, respectively. Between 2016/17 and 2019/20, manufacturer F was on the market in Guangzhou the longest, with 1-dose and 2-dose vaccination rates of 10.0% (95% CI: 9.9%-10.2%) and 8.7% (95% CI: 8.6%-8.8%), respectively. The annual influenza vaccination rate was significantly higher than that of other manufacturers (P < 0.05), and the number of people who chose to be vaccinated with the F vaccine was 2 to 5 times that of A-E manufacturers. Manufacturer A was the latest on the market, and the vaccination rates of 1-dose and 2-dose were 2.2% (95% CI: 2.1%-2.4%) and 1.7% (95% CI: 1.6%-1.9%), respectively. The number of people vaccinated with only the F vaccine was 21.7% (1 dose) and 19.0% (2 doses) (P < 0.05).
Influenza Vaccination Coverage Among Children Aged 6 to 35 months in the Guangzhou, 2016/17 to 2019/20.

Influenza Vaccination Coverage by Sex and Age
As shown in Table 2, boys (1 dose: 23.8% [23.7%-23.9%]; 2 doses: 26.7% [26.6%-26.8%]) and girls (1 dose: 21.0% [20.8%-21.1%]; 2 doses: 22.2% [22.1%-22.3%]) had a difference in vaccination rate (P < 0.05), but boys and girls who chose to vaccinate any manufacturer had similar vaccination rates. The vaccination rate of manufacturer F was significantly higher than that of the other manufacturers (P < 0.05), and there were differences between the 2 groups (P < 0.05). There were significant differences in the vaccination rates of different manufacturers and age groups (P < 0.05).
Gender and Age Wise Vaccine Coverage Among Children by Different Manufacturers in Guangzhou Between 2016/17 and 2019/20.

Note.*6m~: Refers to children aged 6 months to 11 months
1~: Refers to children aged 12 months to 23 months
2~: Refers to children aged 24 months to 35 months
Influenza Vaccination Coverage by Region
There was a significant difference in influenza vaccination rates between the central area and the urban-rural integrated area (P < 0.05), and the vaccination rate of children in the urban-rural integrated area was significantly higher than that of children in the central area (Figure 2). For example, Huadu District, Baiyun District, and Zengcheng District in the urban-rural integration area are significantly higher than Liwan and Yuexiu in the central area. Except for Liwan and Panyu, the vaccination rate of F manufacturers in other regions is the highest.
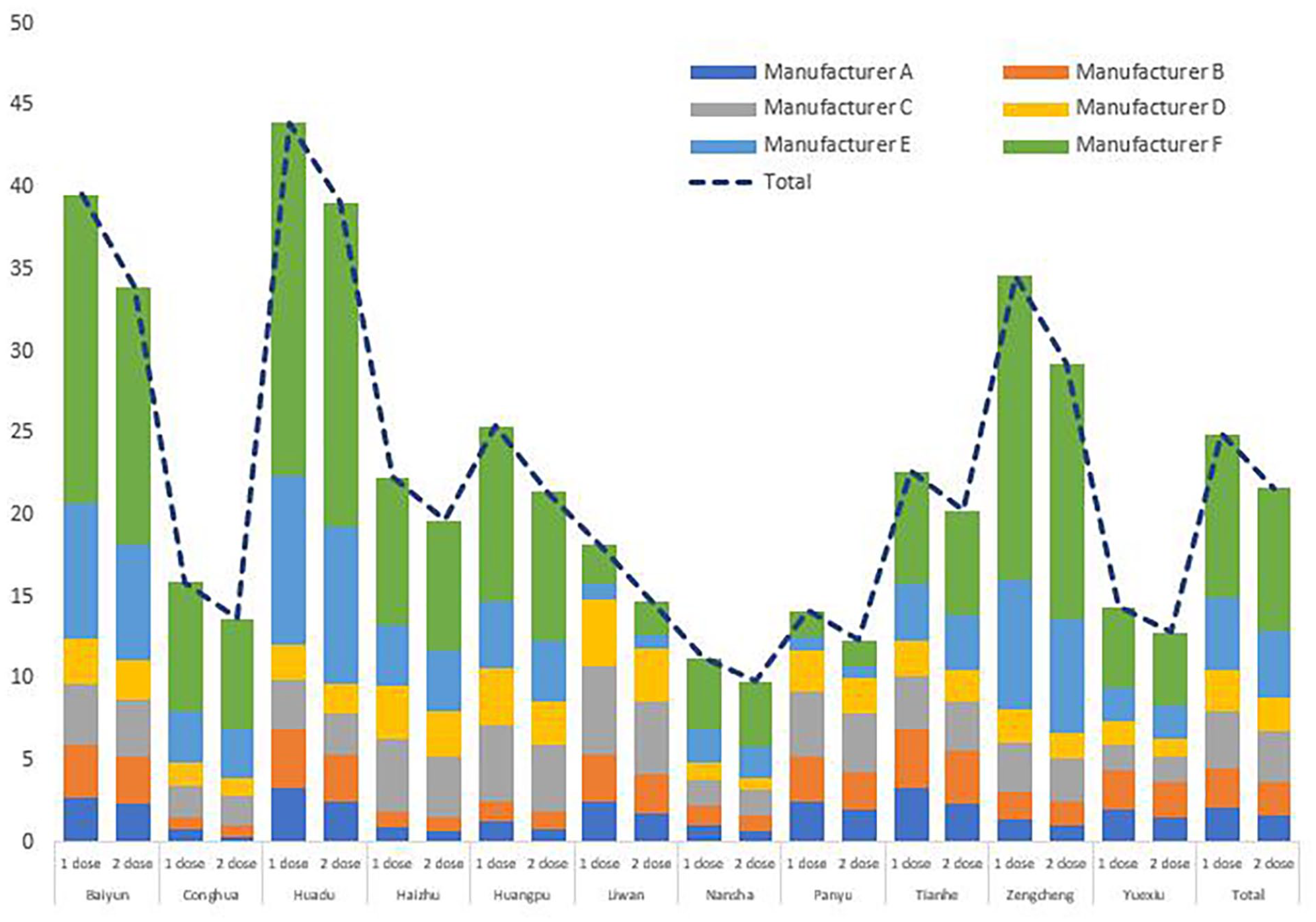
Regional distribution of influenza vaccination coverage of different manufacturers in Guangzhou from 2016/17 to 2019/20.
AEFI Report
AEFI classification
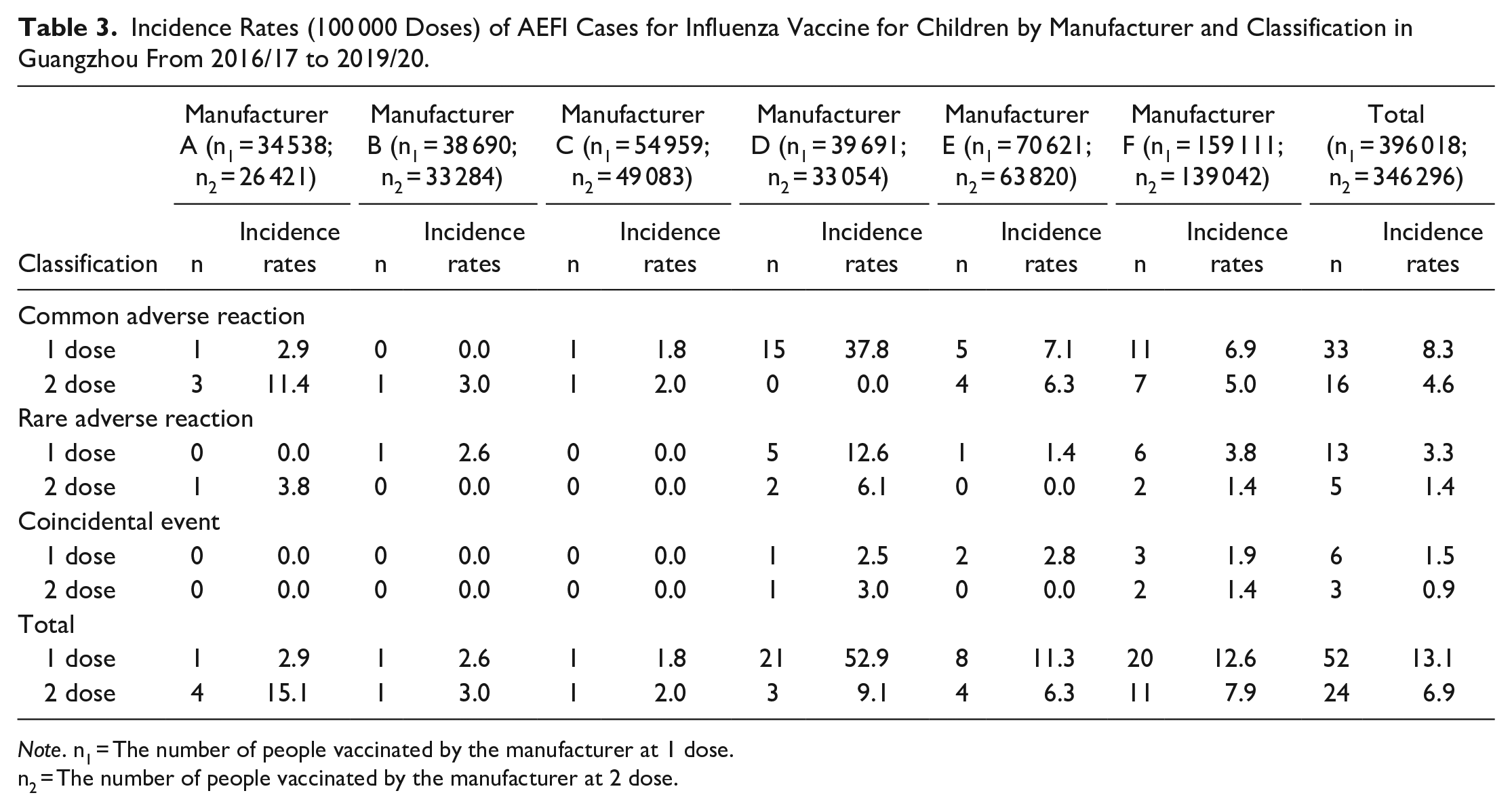
As shown in Table 3, among the 742 314 participants who received childhood influenza vaccine immunization, 76 AEFI reports were received, including 52 cases (13.1/100 000) in 1 dose and 24 cases (6.9/100 000) in 2 doses. No vaccine quality events, vaccine events, or psychological reactions were found. The incidence of general reactions in any dose was significantly higher than that of abnormal reactions and coupled reactions (P < 0.05). Manufacturer F had the highest vaccination rate, but manufacturer D had a significantly higher incidence of AEFI than manufacturer F (P < 0.05); it is noteworthy that manufacturer A had the lowest vaccination rate and the highest incidence of AEFI at 2 doses (15.1/100 000).
Incidence Rates (100 000 Doses) of AEFI Cases for Influenza Vaccine for Children by Manufacturer and Classification in Guangzhou From 2016/17 to 2019/20.
Note. n1 = The number of people vaccinated by the manufacturer at 1 dose.
n2 = The number of people vaccinated by the manufacturer at 2 dose.
Gender, Age, and Time of Occurrence of AEFI
As shown in Table 4, AEFI was reported in 40 boys (1 dose: 27, 6.8/100 000, 2 doses: 13, 3.8/100 000) and 36 girls (1 dose: 25, 6.3/100 000, 2 doses: 11, 3.2/100 000). When boys and girls received 1 dose of the manufacturer D vaccine, the incidence of AEFI (boys: 13, 32.8/100 000, girls: 8, 20.2/100 000) was significantly higher than that of other manufacturers (P < 0.05). When 2 doses of the manufacturer A vaccine were administered, the incidence of AEFI (3, 11.4/100 000) was significantly higher than that of other manufacturers.
Incidence Rates (per 100 000 Doses) of AEFI Cases for Influenza Vaccine for Children by Manufacturer and Gender, Age, and Time of Occurrence Distribution in Guangzhou From 2016/17 to 2019/20.

Note. %*: number of adverse events (n)/total number of adverse events (76 cases) × 100;
Incidence rates*: number of adverse events (n)/number of vaccinations by the manufacturer (1 dose/2 dose) × 100 000.
n1 = The number of people vaccinated by the manufacturer at 1 dose.
n2 = The number of people vaccinated by the manufacturer at 2 dose.
The highest incidence of AEFI in the 1-year-old group was 36 cases (1 dose: 24, 6.1/100 000, 2 doses: 12, 3.5/100 000). The incidence rate of 1-dose manufacturer D vaccine in the 1-year-old group (14 cases, 35.3/100 000) was significantly higher than that of other manufacturers. In the 2-year-old group, the incidence of AEFI in manufacturers D and F were significantly higher than in other manufacturers. It is worth noting that manufacturer A had the lowest vaccination rate, but the incidence of 2-dose AEFI in the 1-year-old group (3 cases, 11.4/100 000) was significantly higher than that of other manufacturers.
A total of 85.53% of AEFIs occurred at 0 day, and the incidence rate was (1 dose: 43, 10.9/100 000, 2 dose: 22, 6.4/100 000) (Table 4). Manufacturer D vaccine had the highest incidence rate of 1 dose (19 cases, 47.9/100 000); A vaccine had the highest incidence rate of 2 doses (3 cases, 11.4/100 000).
Clinical Impairment of AEFI
The most common general reaction was fever, with 85.71% having a fever ≥38.6°C (1 dose: 9, 9.8/100 000, 2 doses: 15, 4.3/100 000). The top 3 in the incidence of 1 dose were the D vaccine (19 cases, 47.9/100 000), F manufacturer (13 cases, 8.2/100 000), and E manufacturer (5 cases, 7.1/100 000). The 2 dose incidence rate was highest with vaccine A (3 cases, 11.4/100 000), followed by 8 cases (5.8/100 000) with manufacturer F and 3 cases (4.7/100 000) with manufacturer E (Table 5).
Incidence Rates (per 100 000 Doses) of AEFI Cases for Influenza Vaccine for Children by Manufacturer and Diagnosis in Guangzhou From 2016/17 to 2019/20.

Note. %*: number of adverse events (n)/total number of adverse events (76 cases) × 100;
Incidence rates *: number of adverse events (n)/number of vaccinations by the manufacturer (1 dose/2 dose) × 100 000.
n1 = The number of people vaccinated by the manufacturer at 1 dose.
n2 = The number of people vaccinated by the manufacturer at 2 dose.
Rare adverse reactions are mainly allergic rash (1 dose: 9, 2.3/100 000, 2 doses: 5, 1.4/100 000): 1 dose of manufacturer D vaccine (2 cases, 5.0/100 000) and F manufacturer (5 cases, 3.11/100 000) the incidence rate was significantly higher than other manufacturers; the incidence rate of 2-dose manufacturer D vaccine (2 cases, 6.1/100 000) and A manufacturer (1 case, 3.8/100 000) was significantly higher to other manufacturers. Angioedema and febrile convulsions are relatively rare. Angioedema occurred in 2 cases in 1 dose, 1 case each in manufacturer D (2.5/100 000) and manufacturer F (0.6/100 000); febrile convulsions only occurred in 1 dose in Manufacturer D (2 cases, 5.0/100 000) (Table 5).
Results of AEFI
A total of 96.05% (73 cases) of children with AEFI were cured or improved, and 3.95% (3 cases) needed treatment.
Discussion
As vaccination remains the most effective means of preventing and controlling influenza, vaccinating young children not only provides personal protection but also affects community transmission.9,10 The vaccination rate from 2016/17 to 2019/20 (1 dose: 25.0% [95% CI: 24.8%-25.2%], 2 doses 21.6% [95% CI: 21.4%-21.8%]) showed a downward trend compared with 2017/18. From 2018/18 to 2019/20, the number of 2-dose vaccinations decreased by 27.8% and 12.94%, respectively. The influenza vaccination rate of children in Guangzhou, China is low, lower than 59.3% of children in the United States, 11 and the vaccination rate of preschool children in Northern Ireland is stable at more than 50%. 12 Vaccination policy is considered to be the main factor affecting the vaccination rate. Except for some areas, influenza vaccines in most areas of China are nonimmunization program vaccines. The implementation of voluntary and self-funded vaccination 7 has brought great difficulties to influenza control. The results showed that during the flu season from 2016/17 to 2019/20, the annual influenza vaccination rate of manufacturer F was significantly higher than that of other manufacturers (P < 0.05), and the number of people who chose to be vaccinated with the F vaccine was 2 to 5 times that of manufacturer A-E times, except for Liwan and Panyu. The vaccination rate of manufacturer F in different regions is significantly higher than that of other manufacturers. Manufacturer F has been on the market in Guangzhou for the longest time, is familiar to the public, and has become the first choice of vaccine for many parents. When encountering manufacturer F, there is a shortage of vaccines, and parents of children prefer to wait for availability or not to get vaccinated. For unfamiliar vaccines, parents are worried about the side effects of the vaccines and are not willing to get vaccinated. This is also one of the reasons for the low vaccination rate of influenza in Guangzhou.
Due to the different levels of education and health knowledge in Guangzhou, there are regional differences in the vaccination rate. The vaccination rate of children in the urban-rural fringe area was significantly higher than that in the central area. For example, Huadu District, Baiyun District, and Zengcheng District in the urban-rural integration area are significantly higher than Liwan and Yuexiu in the central area (P < 0.05). Regarding regional differences, we held an expert seminar and found that the central area is densely populated with governments, hospitals, schools, and financial institutions. Most parents are highly educated, have a wide range of knowledge, and have their own opinions. They are worried about the side effects of unfamiliar vaccines. They are prone to vaccine hesitation, while in urban‒rural areas, there are more farmers, floating populations and small traders, and parents with lower education levels are willing to follow the doctor’s advice. Therefore, the education level of parents may have a positive impact on vaccination willingness. This is consistent with the research results of Zeng et al. 13 We found that vaccination choice was determined by the parents. Therefore, childrens health needs to understand the status quo of children’s parents acquiring influenza-related knowledge. 14 Zhu et al. 15 analyzed the influenza cognition of 669 children’s parents in 12 kindergartens in Xi’an and found that 62.48% of the parents did not vaccinate their children with influenza vaccine, and 34.38% of parents did not know whether to vaccinate their children against influenza. In addition, the recommendations of medical staff can effectively increase the influenza vaccination rate, but the vaccination rate of Chinese medical staff is also very low, only 29.09%, and the low vaccination rate in the population may be consistent with the low vaccination rate among medical staff. 16 This study evaluates the vaccination status of 6 manufacturers’ vaccines and the results of AEFI reports. It aims to inform doctors that the side effects of vaccines are relatively mild, so they can rest assured to vaccinate themselves and recommend them to their parents. Establishing and maintaining high vaccination rates for vaccine-preventable diseases is an ongoing challenge. 17
A total of 742 314 children were vaccinated against influenza in Guangzhou, and 76 AEFI reports were received, including 52 cases (13.1/100 000) with 1 dose and 24 cases (6.9/100 000) with 2 doses. The general response was mainly fever ≥38.5°C (1 dose: 9, 9.8/100 000, 2 doses: 15, 4.3/100 000), consistent with the results of Chinese Wenti. 18 One-dose manufacturer D had the highest incidence (19 cases, 47.9/100 000). The incidence rate (3 cases, 11.4/100 000) of 2-dose manufacturer A was the highest. Rare adverse reactions including allergic rash (1 dose: 9, 2.3/100 000, 2 doses: 5, 1.4/100 000): 1 dose of manufacturer D vaccine (2 cases, 5.0/100 000) and F manufacturer (5 cases, 3.11/100 000) the incidence rate was significantly higher than other manufacturers (P < 0.05); the incidence rate of 2-dose manufacturer D vaccine (2 cases, 6.1/100 000) and A manufacturer (1 case, 3.8/100 000) was significantly higher to other manufacturers (P < 0.05). Angioedema and febrile seizures are less common. The cure or improvement rate was 96.05% (73 cases), consistent with the results of Australia and New Zealand.19,20 The results showed that the highest incidence of AEFI in the 1-year-old group was 36 cases (1 dose: 24, 6.1/100 000, 2 doses: 12, 3.5/100 000). The incidence of AEFI in the 2-year-old group dropped to 29 cases (1 dose: 17, 4.3/100 000, 2 doses: 12, 3.5/100 000). As children age, their immune systems become more mature, and the incidence of adverse reactions gradually decreases. In addition, 85.53% of AEFIs occurred on Day 0, and 92.86% of children developed allergic rash within 1 day. This result suggests that doctors and parents should pay special attention to children’s performance on the day of vaccination. The AEFI incidence rate of the A-F manufacturer was between 1.8 and 52.9/100 000 for 1 dose and 2.0 and 15.1/100 000 for 2 doses. Manufacturer D had the highest AEFI (1 dose: 21, 52.9/100 000, 2 doses: 3, 9.1/100 000), and manufacturer C had the lowest AEFI (1 dose: 1, 1.8/100 000, 2 doses: 1, 2.0/100 000). There were significant differences among the different manufacturers (P < 0.05), which is consistent with the report of Ren et al. 21 Manufacturer D fever and allergic rash occurred most frequently, so it is best to choose other flu vaccines when other vaccine options are available.
In summary, the AEFI response to the influenza vaccine for children in Guangzhou was mild, and the influenza vaccines from 6 manufacturers all had good safety. The results of this study show that the influenza vaccination rate in Guangzhou is low, and the full vaccination rate from 2016/17 to 2019/20 was 21.6%, which is far lower than the 75% recommended by the US Centers for Disease Control and Prevention (CDC). 22 To establish an effective immune barrier in the population to control the influenza epidemic, it is necessary to increase and maintain the influenza vaccination rate at a relatively high level. The main challenge in the future will be to promote correct attitudes and good practices. It is important to ensure continued efforts to provide comprehensive information on the benefits and safety of vaccination and increase uptake. A consistent approach across the country may reduce confusion among providers and parents about the importance of influenza vaccination for children. If the influenza vaccine could be included in the National Immunization Program (NIP) for all young children, 23 this might also help to promote higher intake.
Study Limitations
This study was passive monitoring, and limitations included individual underreporting, biased reporting, and inconsistent quality and completeness of reporting.
Conclusion
The safety of influenza vaccines from 6 manufacturers is good, and it is necessary to improve the recommended information on influenza vaccines to dispel people’s concerns and increase the vaccination rate.
Footnotes
Acknowledgements
We are grateful to all doctors in Guangzhou who reported the influenza network information management system for their contributions.
Author Contributions
Zhi-qun Li: Conceptualization, Methodology, Software, Validation, Formal analysis, Writing-Original Draft, Writing-Review & Editing, Project administration, Supervision, Funding acquisition; Hui-feng Tan: Data curation, Software, Formal analysis, Investigation, Supervision, Project; Zhou-bin Zhang, Qing-long Jing, and Chun-huan Zhang: Project administration, Funding acquisition, Supervision, Project administration, Software; Zi-qi Qin, Li-Hong Ni, and Xue-xia Yun: Software, Validation, Formal analysis, Visualization, Data curation; Jian Chen, Min Cui, Yong Huang, and Wen Wang: Validation, Investigation, Resources; Jian-xiong Xu, Wen-ru Feng, Yan Kang, and Lin Tang: Validation, Investigation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by The key project of medicine discipline of Guangzhou (No.2021-2023-11) and The Medical Research Foundation of Guangdong Province (No.A2022027).
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Guangzhou Center for Disease Control and Prevention.
Consent to Participate
All authors agreed to publish.
Consent for Publication
All authors agreed to publish individual’s data and images.
Data Availability
Vaccination data and AEFI data were obtained from the Guangzhou Children’s Vaccination Information Report Management System and the China AEFI Monitoring Information Management System respectively.
Code Availability
Data were collected with Microsoft Excel files and analyzed with IBM SPSS statistics 27.0 analysis software to calculate the vaccination rate and the incidence of AEFI.