
Abstract
Sleep is an essential physiological function for everyone. Limited evidence existed on the associations between multi-factor sleep patterns and cognition among older adults in rural areas. Aimed to assess that, We conducted a cross-sectional study on the living habits and cognitive status in rural areas of Qingdao and 1167 participants aged 65 to 96 years answered the questionnaire. The result showed that poor sleep quality, high sleep disturbance, daytime dysfunction, and hypnotic drug-dominated sleep patterns were related to the cognitive function, and there was no obviously associations between good sleep duration and cognition. In order to solve the sleep problems and preserve cognitive function, support and protection of physical and mental health should be the priority of government policies in helping older adults’ group in rural areas.
Poor sleep quality in older adults is common and plays an important role in accelerating cognitive aging.
We summarized the current status of multi-factor sleep patterns and cognitive function among older adults in rural China, and adds a perspective of sleep patterns to the relationship between sleep and cognition.
Our findings provide scientific basis for older adults’ healthy care and guide the society pay more attention to the sleep problem of older adults. Improving sleep quality, supporting and protecting physical and mental health should be the priority of government policies in helping the rural older adults’ groups.
With the aggravation of the aging problem, older adults’ health problems are also gaining importance. By 2050, the proportion of the global population aged 60 years and above is expected to grow up to 2 billion from 900 million in 2016. 1 The World Alzheimer’s Disease Report 2010 estimated that the economic burden of dementia would exceed that of cancer, heart disease, and stroke combined as the global population ages. 2 Age-related cognitive decline, including dementia, is likely to worsen because of China’s large population and its rapid aging. 3 China has a large rural population, approximately 510 million, according to the seventh census in 2020. 4 Due to external conditions, the rural population has a lower standard of living, lesser education, and lower occupational levels than the urban population. Studies have shown that better cognitive performance in late stages of life is related to high education level and occupational status. In addition, rural lifestyle may increase the risk of cognitive decline in older adults, which may affect their quality of life.5-7 Therefore, the cognitive function of rural older adults requires more attention. However, there is no effective medicine to treat the disease; thus, identifying potential risk factors for altering dementia and cognitive decline is crucial for their prevention.
Sleep is an essential physiological function for everyone, which facilitates many functions, from tissue repair to brain metabolite clearance. 8 Sleep insufficiency has long been known to cause poor attention spans and impair the ability to perform tasks. 9 Recent epidemiological studies have shown that good sleep plays an important role in slowing cognitive aging. Unfortunately, poor sleep quality in older adults is common: up to 50% of older adults have habitual sleep problems. 10 Studies have shown that sleep deprivation could inhibit the clearance rate of amyloid-β in the brain, the accumulation of which increases the risk of cognitive impairmentt.11,12 Studies have also indicated that memory is consolidated in the hippocampus during slow-wave sleep. 13 However, most existing studies have separately explored the relationship between a single dimension of sleep and cognitive function.14-17 Moreover, only a few studies have combined individual dimensions and considered them as a whole to evaluate the relation between sleep and health. 18 We aimed to perform multivariate statistical methods to establish multi-factor sleep patterns (SPs) and to explore the connection between different SPs and cognitive function, thus we conducted a cross-sectional survey and used exploratory factor analysis (EFA) to investigate the relationship, which could provide insights for future clinical studies.
Methods
Data Source and Participants
A cross-sectional study was conducted in co-operation with the Licha Health Center of Jiaozhou town, Qingdao City, from April 2019 to August 2019. The Licha Health Centre staff helped in organizing the investigation and communicating with villagers. Random cluster sampling method was used. The inclusion criteria were as follows: (1) age over 65 years, (2) Local residence of minimum 6 months or more, and (3) ability to communicate normally. The exclusion criteria were as follows: (1) presence of severe liver, kidney, and heart diseases and limited mobility; (2) presence of dementia or Alzheimer’s disease; (3) difficulty in communication or inability to complete the questionnaire; (4) presence of sensory disabilities (deafness, blindness) or severe hearing impairment; and (5) long-term use of antidepressants drugs. We used questionnaires that included general surveys questions on cognitive function and sleep quality. Before the investigation, the researchers from our department conducted a unified training. All the research participants were surveyed through face-to-face interviews in the presence of local medical staff. Our study was approved by the Ethics Committee for Medical Research at Qingdao Municipal Centre for Disease Control and Prevention (spaq-2016-125). Prior to the start of the project, all participants signed an informed consent form after being explained about the main experimental content, advantages, and disadvantages of the project and were informed that they could withdraw at any time. All questionnaires were coded, and all analysis was based on the code. This study promises that all participants’ information is only used for scientific research and was not/will not be disclosed to the public.
General Condition
The general survey included sex (male assigned 1, female assigned 2), age, education (illiterate, primary, and secondary and more, assigned 1, 2, and 3, respectively), marital status (single, married, and divorced or widowed, assigned 1, 2, and 3, respectively), smoking status, alcohol consumption, income, living condition (living with a member, alone, with spouse, children or other people, assigned 1, 2, 3, 4, respectively), chronic disease, and body mass index (BMI). Smoking status and alcohol consumption were defined in the terms of the presence or absence of the behavior (assigned 1 and 2, respectively). The participants were also questioned for the presence and type of chronic disease, if any. (no, 1, 2, ≥3).19,20
Based on the eligibility criteria, a total of 1167 participants aged 65 to 96 years, 44.5% of whom were male, were included (Supplemental Figure 1). Among the participants, 45.5% were illiterate, and 19.1% had a secondary or high school education or above.
Cognitive Function Appraisal via Mini-Mental State Scale (MMSE)
Cognitive function was evaluated using the MMSE scale, one of the most influential and popular cognitive impairment screening scale tools in the world. 21 It is a brief general cognitive screening instrument consisting of 22 questions. The scale includes 5 cognitive fields, including orientation, registration, attention and calculation, recall ability, and language ability, with full marks of 10, 3, 5, 3, and 9, respectively. MMSE scores ranged from 0 to 30, with higher scores associated with better cognitive function.
Pittsburgh Sleep Quality Index (PSQI)
The index is a self-report questionnaire developed by Buysse et al in 1989. 22 This is a standard questionnaire with 18 questions divided into 7 parts. The first component concerns mental quality of sleep and consists of one question (Question 6). The second part is related to delayed sleep, which is the first part of Questions 2 and 5a based on the score of the measurement. The third part is about sleep duration, consisting of one question (Question 4). The fourth part is about the efficiency and effectiveness of sleep; the score is calculated as total hours of sleep divided by the time spent in bed, multiplied by 100. The fifth part is related to sleep disorders and is obtained by calculating the average score of Questions 5b-j. The sixth component is associated with the consumption of sleep medication and comprises of one question (Question 7). The seventh component is related to the daytime dysfunction, which is the average score of 2 questions (the mean score of Questions 8 and 9). Each question is scored from 0 to 3 for each component, and the maximum score is 3. The 7 components provide the total score of the questionnaire, which range from 0 to 21 points. The higher the score, the lower the quality of sleep. Scores higher than 5 indicate poor sleep quality.
Statistical Analysis
Dataset was established using Epidata 3.1 with double entry. Principal component analysis was used to extract factors as SPs. The orthogonal rotation method with maximum variance was selected to rotate the initial factor load, and the influence of each variable obtained by this on the extracted principal components was interpret-able. The percentage of data variation was explained by combining eigenvalues greater than 1. The common factor number was determined by using the index of the scree plot and the interpret-ability of the results. The factor load represents the correlation between the SP variable and the extracted SP. And the larger the absolute value, the greater the contribution of the factor to the SP. The factor with an absolute value of factor load of 0.50 was the main factor affecting the model. The sample size was divided into 3 groups according to each SP factor’s score. T1, T2, and T3 were the low, moderate, and high adherence groups corresponding to 389, 390, and 388 people, respectively. The cut-off scores for T1, T2, and T3 of SP 1 were −1.260 to −0.516, −0.516 to −0.125, and −0.125 to 3.833; the cut-off scores for T1, T2, and T3 of SP 2 were −1.730 to −0.578, −0.578 to 0.156, and 0.156 to 5.289, respectively. The association between general condition, SPs, and cognition variables was verified using the Kruskal–Wallis H test. Three models were established to estimate the change in cognitive function for the 2 factors by multiple logistic regression analysis. And the analysis was performed to estimate the odds ratio (OR) and its 95% confidence interval (95% CI) for each cognitive file according to the tertile of each factor score, and the lowest tertile was used as the reference category. Model 1 was an unadjusted model. Model 2 was adjusted for sex and age. Model 3 was additionally adjusted for other conditions (including education, marital status, smoking status, alcohol consumption, BMI, income, living condition, and chronic disease). A 2-sided P-value < .05 was considered statistically significant. All data were statistically analyzed by using SPSS 26.0.
Results
Association Between the General Condition and Cognitive Function
The correlation analysis results of the general condition and total MMSE score are shown in Table 1. For the convenience of statistical analysis, participants were divided into quartiles according to the MMSE total score, denoted as Q1, Q2, Q3, and Q4. There were statistical differences between the quartiles of MMSE total score and sex, age, marital status, smoking status, alcohol consumption, income, and living condition (P < .05). The quartiles of MMSE total score were negatively associated with sex, age, marital status, and smoking status (P < .05). The quartiles were found to be positively associated with the education level and income (P < .05). There were also statistically significant differences between sleep disturbance, the total score of PSQI, and MMSE scores (P = .009, P < .01, respectively). The high MMSE scores were associated with high PSQI scores and sleep disturbance.
Univariate Analysis Between General Condition and Cognition.

Note: BMI = body mass index.
P < .05.
Factor Analysis for SPs
The scree plot showed that 2 main factors could be extracted for EFA (Supplemental Figure 2). Two factors were identified and were defined as SP 1 and 2. SP 1 was characterized by high sleep latency, short sleep duration, and low sleep efficiency, while SP 2 was characterized by poor subjective sleep quality, high sleep disturbance, daytime dysfunction, and consumption of hypnotic drugs (Supplemental Table 1). According to the distinction of sleep dimensions, SP 1 mainly focused on the length of sleep time, and SP 2 focused on other events that affected sleep quality. Therefore, we defined SP 1 as “Sleep duration” and SP 2 as “Other sleep qualities.” This meant that the higher the correlation with SP 1, the shorter the sleep time. The higher the correlation with SP 2, the more factors affect sleep quality. The 2 factors explained 57.4% of the total variation in the response variables.
The Relationship Between General Condition and Two SPs
No statistically significant differences were observed between sex, education, smoking status, BMI, income, living conditions, and SPs (Table 2). There was statistical significance between age and SP 2 (P = .019), and there was a difference between the T3 and T2 groups (P < .05). SP 1 was statistically significant for marital status (P = .008) and alcohol consumption (P = .018), and SP 2 was statistically significant for chronic disease (P = .004).
Association Between the General Condition and SPs.

Note: BMI = body mass index.
Q1 compared with Q2, P < .05; bQ2 compared with Q3, P < .05; cQ1 compared with Q3, P < .05.
P < .05.
The Association Between Cognitive Function and SPs
Table 3 shows the significant differences in the MSME total score, registration, recall and language ability of SP 2 (P = .006, .001, .033, and .019, respectively), whereas no statistical difference was found between SP 1 and cognitive function. It showed significant differences between the T1 and T2 groups of SP 2 in MSME total score, recall, and language ability (P < .05). There were statistically significant differences between the T2 and T3 groups in registration and recall ability (P < .05). The registration ability had statistically significant differences in the T1 and T3 groups (P < .05).
Association Between the Mini-Mental State Examination Scores and SPs.
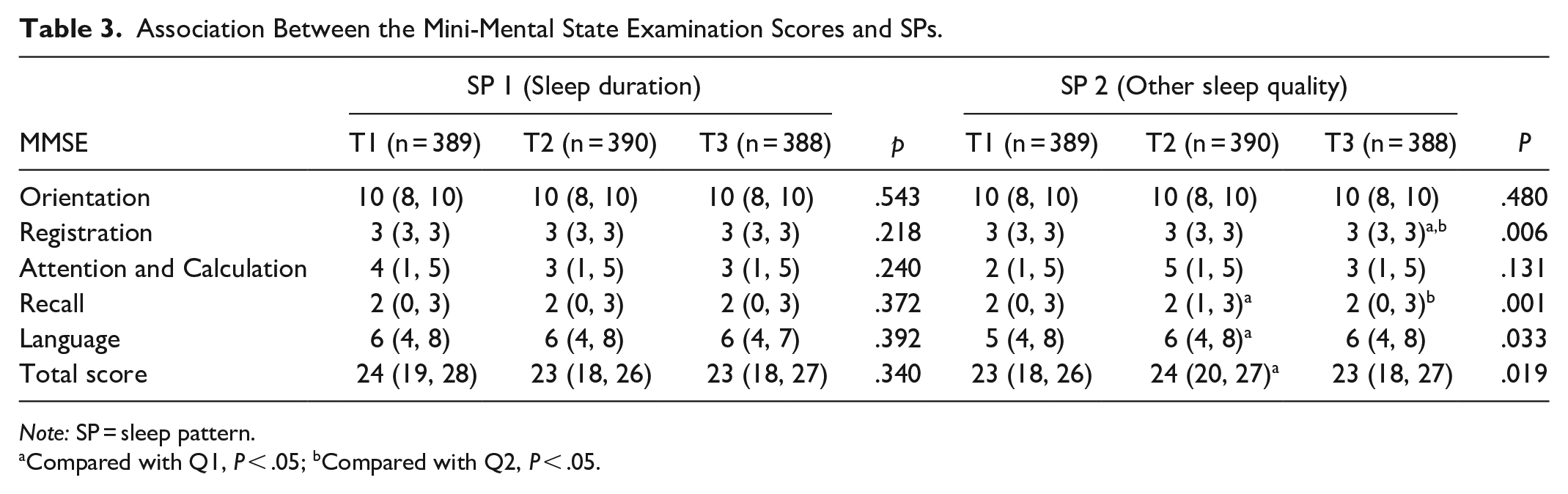
Note: SP = sleep pattern.
Compared with Q1, P < .05; bCompared with Q2, P < .05.
Associations Between SPs and Cognitive Function by Multiple Logistic Regression Analysis
Compared to the participants in the T1 group of SP 2, after adjusting for the covariates (sex and age), those in the T2 group had significantly increased recall (OR: 1.22; 95% CI: 1.08-1.36) and language ability (OR: 1.09; 95% CI: 1.02-1.16), as well as the MMSE total score (OR: 1.03; 95% CI: 1.01-1.06), and T3 group had significantly decreased registration (OR: 0.75; 95% CI: 0.61, 0.92). In addition, the T2 group of SP 1 had an 11.0% decrease in recall ability (OR: 0.89; 95% CI: 0.79-0.99). There was no association between SP 1 and the other outcomes (Table 4). After adjusting to Model 3, no statistical significance among all the variables was observed.
Multiple Logistic Regression Analysis Results Between Cognition and SPs.

Note: SP = sleep pattern.
Model 1: unadjusted model.
Model 2: adjusted for sex and age.
Model 3: adjusted for all variables in model 2 and the other general conditions (including education, marital status, cigarette, alcohol, BMI, income, living condition and chronic disease).
P < .05.
Discussion
This study reports 2 main sleep patterns characterized by EFA among older adults residing in rural areas of Qingdao City, China. In the present study, we have shown that SP 2 was associated with cognitive function, whereas no such association was found in SP 1. The SP 2 contains four dimensions, including poor subjective sleep quality, high sleep disturbance, daytime dysfunction, and consumption of hypnotic drugs. It was speculated that the association between SP2 and the cognitive function of older adults might be through its relation with memory, recall, and language abilities.
The cognitive function of the elderly has an important influence on their quality of life. A large number of studies have analyzed the influencing factors of cognitive decline. 23 This study also found that cognitive function declined physiologically with age. The hormones differences between genders will also induced the different effects on cognitive function. 24 Additionally, the education level of rural women is generally lower than that of men, which also affects their cognitive function to a certain extent. The increase of education level and income can improve the health awareness and nutrient intake level of the elderly, so they show a better cognitive level. 25 At the same time, we also found that smoking and alcohol intake were positively correlated with cognitive scores. This has been reported as well that moderate drinking and smoking were associated with better cognitive performance.26,27 We speculated that this might also be related to the fact that people who smoke and drink usually have higher living standards. In addition to looking at the general situation and lifestyle of older adults, a growing number of studies are trying to explore other factors that influence cognitive function, such as sleep. Many studies have proven the link between sleep quality and cognitive function, and have stated that poor sleep quality is related to cognitive decline.8,9,28 The MMSE score decreased with increased PSQI score, that is, the worse the sleep quality, the worse the cognitive function. The relationship between sleep quality and cognition was found to be similar to previous studies.29-32 One topic of current interest is whether aging slows the connection between sleep and memory. An interesting observation was that sleep deprivation in middle aged might lead to neurobiological damage, which worsened over time. 33 However, most studies focused on the association between sleep duration, sleep latency, and cognition. Our study did not find significant associations between these dimensions and the cognitive function of rural older adults. Establishing sleep patterns through factor analysis may help us better understand the association between sleep quality and cognition.
We used EFA for the first time to perform dimensionality reduction on sleep-related indicators in rural older adults. The 7 items of the PSQI scale were divided into 2 SPs and analyzed with cognitive ability. It was concluded that the SP dominated by factor 2 was related to the cognitive function of older adults. Therefore, we could consider that subjective sleep quality, sleep disturbance, daytime dysfunction, and consumption of hypnotic drugs may be correlated with the cognitive abilities of older adults. A negative association was found between SP 2 and memory ability, suggesting that older adults with poor sleep quality also have poor memory. Moreover, our results found a significant difference between general conditions such as sex and cognition. Therefore, considering these general confounding factors, we conducted a regression analysis on the relationship between the 2 SPs and cognitive function by adjusting confounding factors. When adjusted for age and sex only, recall and language ability, and total cognitive scores were more associated with T2 group of SP 2 than with T1 group, which is the same as the unadjusted model. Meanwhile, the T3 group of SP 2 of registration showed a significant difference compared to T1. The regression analysis results were consistent with that of the Kruskal–Wallis H test. This may mean that the worse the sleep quality, the more presence of other events that affect sleep, and the worse the memory ability. This may be related to sleep disturbance in SP 2. Studies have shown that an increase in night-time awakenings was related to poor memory, suggesting that fragmented sleep, rather than short sleep, may be associated with cognitive function in older adults in small sample studies.34,35 We observed that the relationship between SP 2 factor scores and recall, language ability, and MMSE total score may be U-shaped; however, the correlation analysis did not show a statistical difference. Therefore, further longitudinal studies may be needed to prove the exact trend. Moreover, it was found that chronic diseases were negatively correlated with SP 2, which meant that presence of chronic diseases was associated with worse sleep quality. Some studies have shown that poor sleep quality increases the risk of cardiovascular 36 and metabolic diseases. 37 Population-based studies have shown a significantly high risk of cardiovascular and cerebrovascular diseases (such as atherosclerosis, coronary heart disease, hypertension, and stroke) and metabolic disorders (such as obesity and type 2 diabetes) in people with sleep-disordered breathing or insomnia. 38 Their interaction might also influence the cognitive function of rural older adults. The link between sleep quality and cognition has been supported by a number of scientific studies.39,40 Studies have shown that sleep quality is closely related to daytime function. 41 People who self-reported poor sleep quality also performed poorly during the day. Sleep disorders could lead to changes in cognitive sleep function throughout a person’s life (eg, prompting compensation attempts and/or weakening the connection between sleep and cognition). Sleep deprivation/restriction could lead to protein misfolding, 42 reduced tau phosphorylation, 43 and increased amyloid deposition. 44 People who use hypnotic drugs are generally insomniacs. Patients with insomnia may experience cortical activation, which may further interfere with certain aspects of cognitive performance, as well as the ability to channel energy. 45
Sleep tends to shorten over a person’s lifetime. 46 The previous studies focused mainly on the association between sleep duration and cognition.13,47,48 These studies suggested that sleep duration may be linked to cognitive function through changes in sleep structure, sleep fragmentation, sleep quality, and nervous system conditions.47,49 However, these associations were not observed in the present study, which indicated that increasing the amount of sleep among older adults was unlikely to restore cognitive ability. The reason be due to neurobiological changes in older people, such as nerve atrophy, decreased plasticity, and neuroendocrine changes. Our findings also proved that the association between sleep duration and cognition is not obviously.
However, our study has some limitations. Observational studies have found an association between self-reported sleep duration or quality and cognitive function. However, they could not establish a causal relationship between these factors. Meanwhile, subjective self-report may not correlate well with objective measures of sleep; Misstatements may lead to bias. Although the living habits/lifestyle of the older adults enrolled in our study may differ from those residing in the rural areas of the western countries, our study data can be used as a reference for improving SPs of older adults with same sleep habits to further improve their cognitive ability.
Conclusion
In conclusion, sleep quality and cognitive function were found to be associated in rural older adults in Qingdao City, China. Poor sleep quality, high sleep disturbance, daytime dysfunction, and hypnotic drug-dominated SPs were related to the cognitive function, and there was no obviously associations between good sleep duration and cognition.
To sum it up, our research has practical value and theoretical implications. These findings are helpful for the health policy practice of China in some ways, and guide the society pay more attention to the sleep problem of older adults. Improving sleep quality, supporting and protecting physical and mental health should be the priority of government policies in helping the rural older adults’ groups. Also, our research enriched relevant theoretical research for older adults’ healthy care. For the analytical perspectives and methods, this article analyzed the rural older adults’ based on China’s background.
Moreover, a series of epidemiological studies can be conducted to prove the exact relationship between sleep and cognition in older adults and provide more theoretical basis for improving the quality of life of older adults.
Supplemental Material
sj-doc-1-inq-10.1177_00469580231171820 – Supplemental material for Association Between Sleep and Cognition of Older Adults in Rural Areas: A Cross-Sectional Study
Supplemental material, sj-doc-1-inq-10.1177_00469580231171820 for Association Between Sleep and Cognition of Older Adults in Rural Areas: A Cross-Sectional Study by Wenjia Meng, Tianlin Gao, Yang Zhong and Ling Ge in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Statement
The data has not been previously presented orally or by poster at scientific meetings.
Ethical Approval
Our study was approved by the Ethics Committee for Medical Research (Reference Number: spaq-2016-125). All participants sign an informed consent form. All questionnaires are coded and all analysis is based on the code. All methods were carried out in accordance with relevant guidelines and regulations
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.