
Abstract
This study objective to verify the existence of gaps in the dynamics and performance of fulfillment of the deinstitutionalization of psychiatric care in the Czech Republic (CZ) and the Slovak Republic (SR) in the period between 2010 and 2020. The introduction of this the study is a search for expert knowledge in the field of deinstitutionalization of psychiatric care. The study uses the method of multi-criteria comparison of TOPSIS variants and a cluster analysis. The results 22 variants range from (ci 0.6716-0.2571) and confirm that there are large differences between CZ and SR in performance gaps (fulfillment) of deinstitutionalization goals. The SR variants are clearly better than the CZ variants, although during the years studied, the CZ variants are improving, and the size of the gap compared to the SR variants is decreasing. In the first year of the evaluated period (2010), the performance gap was 56% and in the last year (2020), the performance gap was only 31%. The conclusion of the study confirms that the measures associated with the deinstitutionalization of psychiatric care are linked to the time they were introduced and the overall implementation period of the reform.
Deinstitutionalization is a prerequisite for modern psychiatric care reform and has a specific course and effect in each state. The experience gained with deinstitutionalization in one state cannot simply be implemented in another state. For this reason, a comparative international assessment of deinstitutionalization uses simple analyses of aggregated indicators. Unlike other medical disciplines, research in the field of deinstitutionalization and reforming of psychiatric care does not use the capabilities of the Multi-criteria Decision Analysis methods (MCDA) for the assessment.
The research presents an original conception of the analysis of the dynamics and differences in the performance of deinstitutionalization of psychiatric care in 2 close states—the Czech Republic and the Slovak Republic. The research verifies the possibilities of the TOPSIS Technique, with the help of which it detects gaps in the course of deinstitutionalization’s implementation.
The research has shown that it is possible to compare the achievement of the goals set for deinstitutionalization in the context of the length of implementation, and subsequently indicate the factors disrupting it (eg, the COVID-19 pandemic). Research has also confirmed that MCDA techniques can be used for international comparison, which can be understandably interpreted for practice and improve the decision-making at the political level.
Introduction
Mental health, in particular its deficits, has come to the forefront of political interest over the last 20 years. The main reason is the rapidly growing burden that mental illness and poor mental health place on societies. According to The European Mental Health Action Plan 2013-2020, mental disorders are one of the main public health problems in the European region, affecting up to 25% of the population. The number of people in need of intensive psychiatric and psychological care is growing in the Czech Republic and the Slovak Republic as well. This is documented by national statistics (Institute of Health Information and Statistics of the Czech Republic—IHIS CZ; National Health Information Centre of Slovakia) as well as international comparisons.1-3
Modern, comprehensive, and affordable mental health care is a pillar of the reform and development national concepts of numerous economically and socially developed countries. In their reforms, governments respond to the topical needs of the current population and the findings of modern medicine and social work. Most European countries now have mental health policies and legislation, and many are making progress by introducing community-based services to their mental health care systems. However, experience shows that the capacity, quality, and professional provision of mental health care services vary greatly across countries and regions in Europe. The development and progress of the reform of this care at the level of individual states is influenced by many specific internal and external factors of an economic and social nature4-7
The first stage of mental health care reform usually focuses on the deinstitutionalization of psychiatric care and the development of community-based services, and this brings high demands on public and private spending, among other things. As stated by the WHO, 3 some European countries, including the Czech Republic and the Slovak Republic, have their health care systems built on large psychiatric hospitals and psychiatric care is strongly institutionalized.
Deinstitutionalization of psychiatric care is a process requiring numerous interconnected and often complex changes in society. Especially in a society that has been stereotypically accepting an isolated approach to mental health care for many years. Deinstitutionalization must therefore be understood only as the transformation of a sub-segment of the psychiatric care system. Its primary goal is to shift the focus from long-term institutional care to community-based care. However, it should be noted that the needs for care and treatment in psychiatry are very diverse both in terms of diagnosis and the age and general health of the patient. Thus, long-term hospitalization still has its medical justification. 6
Continuous and partial evaluations of the deinstitutionalization process, including critical and multi-criteria perspectives, represent a prerequisite for the success of the reform or the psychiatric care strategies. The evaluation of deinstitutionalization is important from the perspective of both the government and the citizens. This is because the results of the evaluation enable the government to apply appropriate regulatory, allocation, and institutional measures more effectively and flexibly and thus better respond to ongoing changes.8,9
According to the results of a study performed by Khan et al, 10 Multi-criteria Decision Analysis methods (MCDA) are often used to analyze health care issues. The choice of a particular method is determined by the nature and complexity of the health care issue. Popular methods include the TOPSIS Technique. However, MCDA methods have not yet been used to assess psychiatric reforms or deinstitutionalization in this area.
The aim of the article is to detect and compare of gaps in the dynamics and performance of fulfilment of the selected criteria for the deinstitutionalization of psychiatric care in the Czech Republic (CZ) and the Slovak Republic (SR) using the TOPSIS Technique for the period between 2010 and 2020.
The article’s structure consists of 5 parts. The first is the introduction, which mainly describes the motivation of the research. The second part deals with the basic assumptions of the issue of deinstitutionalization of psychiatric care and complements the motivation of the research outlined before. The third part describes the research methodology. It includes the aim of the research, research topics and questions as well as the characteristics of selected criteria and a description of the TOPSIS Technique. The fourth part presents the results of the calculations and their analysis. The fifth part, the conclusion and discussion, summarizes the findings achieved.
Theoretical Backgrounds
The model of care for people with mental illness based on large psychiatric institutions, which was prevailing for many years, is now gradually receding. Deinstitutionalization is a necessary process in any modern reform of psychiatric care. The idea of deinstitutionalization is based on a gradual diversion from the institutional model of care. It reinforces 3 principles that improve the quality of care and human rights: (i) prioritizing adequate community-based services over hospitalization in a psychiatric hospital, (ii) releasing long-term hospitalized patients that are sufficiently prepared for such change into community conditions, and (iii) the introduction and ensuring of sustainability of the system of community mental health care services.11,12
Many countries have been tackling strong institutionalization and long-term isolated care for people with mental illness since the second half of the 20th century. Based on data from 161 countries, Hudson 13 states that the deinstitutionalization of psychiatric care has been happening since the 1950s, being a trend shaped by various socio-cultural conditions and competing ideologies. Key issues that need to be expertly addressed include the scope, motivation, political and financial dimensions, and implications in areas such as homelessness, nursing care, and the criminalization of the mentally ill.
Deinstitutionalization usually requires building new organizational structures for mental health care, integrating psychiatric patients into the general health care systems, creating a large community network of mental health centers, and adopting more positive public attitudes toward mental illness and treatment as well as legislative measures to improve civil rights of these patients.14,15
In the Czech Republic and the Slovak Republic, as in many other European countries (Germany, Poland, Austria, Denmark, France, and others), the reform of psychiatric care was not systematically implemented until the 21st century. In the Czech Republic, this has been the case since 2014, based on the Strategy for the Reform of Psychiatric Care for 2014 to 2023. 16 In the Slovak Republic, the implementation was based on the National Mental Health Plan from 2002. Nevertheless, it was put into practice with a delay in 2006. 17
According to the WHO, 3 in 2020, 91% (n = 42) of European states had public policy for mental health and 70% (n = 32) of states had specific legislation governing mental health. Globally, government spending and sufficient professional human resources appear to be the most important prerequisites for meeting the goals of mental health care reform. Both assumptions, especially expenditures, cannot be precisely defined even at the level of a given state, and an international comparison would be highly misleading. However, the WHO uses national respondents to make an expert estimate of the share of government mental health expenditure per capita expressed as percentage. In European countries, mental health expenditure averaged at 3.6% of total health expenditure in 2020. The largest part of these expenditures is spent by the state on “Mental hospitals” and also on “Community mental health services.” The lowest expenditures are spent by the states on the issue of “Mental health prevention and promotion” and “Mental health supports at primary care level.”
The deinstitutionalization of psychiatric care always has a specific course and states face numerous individual problems in its implementation, as shown in the study by Haug and Rössler 14 comparing deinstitutionalization in Germany, Austria, Switzerland, and Luxembourg. The study showed that, although these countries are similar in many socio-economic factors, their processes of deinstitutionalization faced different issues. This led to the point when deinstitutionalization objectives have still not been satisfactorily met in these countries.
It is generally accepted that assessing the success of deinstitutionalization is very difficult, and this also applies to drawing a clear position on the objectives and speed of the deinstitutionalization process. The experience gained with deinstitutionalization in one state cannot simply be implemented in another state, and the reasons are socio-economic rather than medical or social. It also seems short-sighted to emphasize the criteria aimed at the robustness of the institutional background in assessing deinstitutionalization and leave the criteria of performance and quality of the care system in question neglected. 6
Methodology
This study has the nature of an original comparative analysis, uses multi-criteria techniques to define gaps and differences in the implementation of public policies in the field of psychiatric care reform aimed at deinstitutionalization.
The research methodology was chosen in connection with the article’s objective, which is the definition and comparison of gaps in the dynamics and performance of the fulfilment of selected criteria of deinstitutionalization of psychiatric care in the Czech Republic (CZ) and Slovak Republic (SR) using the TOPSIS Technique for the period 2010 to 2020.
The fulfilment of the objective follows 2 research topics RT I. and RT II., including 5 research questions RQ1-RQ5.
The first research topic (RT I.) deals with issues of dynamics and the relationships among the selected criteria of deinstitutionalization during the evaluated period. The answers to the questions below are being sought:
RQ1: “Are the selected criteria developing in the monitored period in the CZ and the SR with the same dynamics?”
RQ2: “Is there an expected direct/indirect mutual relationship among the criteria?”
The second research topic (RT II.) focuses on the detection of gaps and differences in the performance of deinstitutionalization using the TOPSIS Technique between the CZ variants and the SR variants. The answers to the questions below are being sought:
RQ3: “Is there a clear performance gap between the CZ and SR variants?”
RQ4: “Do the 2018-2020 variants achieve the best results?”
RQ5: “Can the trend of deinstitutionalization of psychiatric care in individual states be deduced from the results of the multicriteria analysis via the TOPSIS Technique?”
Research topics and their questions were formulated based on the assumptions resulting from the published knowledge (policies, analyses, and statistics) in the field of mental health reforms in the Czech Republic and the Slovak Republic as well as the methodology of multi-criteria evaluation. The key stimuli for the above-mentioned issues are given by the evaluated period 2010 to 2020, as deinstitutionalization began to take place differently in the countries studied. The planned deinstitutionalization in the CZ started in the first half of the evaluated period, specifically in 2014. In contrast, the planned deinstitutionalization in the Slovak Republic started as early as in 2002.3,6
Data
The evaluated set contains 22 observations, which are marked as variants in the TOPSIS model (11 variants from the CZ and 11 variants from the SR). Variants are marked successively with numbers 1 to 22, the abbreviation of the state CZ/SR and the year within the observed period 2010 to 2020 (eg, the first variant is marked: 1_CZ2010 and the last variant is marked 22_SR2020). Each variant contains 5 criteria (C1-C5) and their values correspond to a given year, so a total of 110 variables were assessed.
The criteria for deinstitutionalization of psychiatric care were selected regarding the defined objectives of psychiatric care (mental health) reforms in the Czech Republic and the Slovak Republic. In both reforms, deinstitutionalization mainly concerns the reduction of inpatient care, the expansion of outpatient care, and the improvement of the quality of care provided. The choice of criteria was also influenced by the fact that these criteria are used in other research projects addressing the deinstitutionalization of psychiatric care.8,13-15,18
For the reasons described above, the relative values of the 5 criteria C1-C5 were recalculated per 1000 citizens of the given state in the given year (2010-2020) as of 31 December. For the multi-criteria evaluation according to the TOPSIS Technique, the weight (w) was calculated for each criterion. This was performed according to the Fuller method of pairwise comparison with the participation of experts from the academic and professional sphere, and the maximization/minimization characteristic was determined for each criterion.
Criterion C1 Number of outpatient care patients (w = 0.21, max.). This is a criterion that expresses the number of patients treated in psychiatric outpatient clinics (see C5) in a given year.
Criterion C2 Number of completed hospitalizations (w = 0.14, max.). This is a criterion that expresses how many patients completed inpatient treatment in hospitals/medical institutions in a given year. Discontinuation of treatment is performed based on the decision of both the doctor and the patient. The reason for termination may also be the transfer of the patient to another department of the hospital care (eg, internal, neurological), to outpatient care, but also the death of the patient.
Criterion C3 Number of hospital beds (w = 0.15, min.). These are the numbers of beds in hospitals (special wards) and medical institutions.
Criterion C4 Number of physicians (w = 0.27, max.). This is a criterion expressing the recalculated number of physicians (psychiatrists) for full-time equivalents in hospitals and outpatient psychiatric care facilities (most doctors work part-time in hospitals/medical institutions and part-time in outpatient clinics).
Criterion C5 Number of outpatient care facilities (w = 0.23, max.). This is a criterion expressing the number of psychiatric outpatient clinics that provided services in a given year in a given state. These are outpatient psychiatry clinics, child and adolescent psychiatry clinics, geriatric psychiatry clinics, addictive diseases clinics, and sexology clinics.
The data entries were obtained from special statistical yearbooks for individual years (2010-2020), which are published by the Institute of Health Information and Accounting of the Czech Republic—IHIS CZ; National Health Information Centre of Slovakia—NHIC SK). The basic characteristics of the data set (criteria C1-C5) for the studied 11-year period (2010-2020) are displayed in Table 1. For each criterion, the table shows (for the evaluated group and partially for the CZ and the SR): means, standard deviations (SD), and limit values (max. and min.), including the year in which the data entries were recorded.
Descriptive Statistics of the Criteria, Period 2010 to 2020.

Table 1 shows interesting differences and similarities between countries (CZ and SR), which can be observed in the monitored criteria (C1-C5) in the studied period, regarding the year when they reached the maximum/minimum value of the criterion. Furthermore, the table shows that CZ achieves higher average values compared to SR in criteria C3 (number of beds), C4 (number of physicians), and C5 (number of outpatient care facilities). On the contrary, compared to the CZ, the SR achieves higher average values in criteria C1 (number of outpatient care patients) and C2 (number of completed hospitalizations).
Methods: The TOPSIS Technique
To verify the research questions set within the RT I. in connection to the objective of the research, the classical methods were applied. In this case it was the correlation analysis according to the Pearson coefficient as the most suitable one. To verify the research questions within RT II. in connection to the objective of the research, a 2-phase analysis was performed. In the first phase, the indicators of 22 variants are calculated according to the TOPSIS Technique. Subsequently, the values of the indicators are compared using statistical techniques and cluster analysis. The key method of this research is thus the TOPSIS Technique.
The TOPSIS Technique (Technique for Order Preference by Similarity to Ideal Solution) belongs to the basic techniques of multi-criteria evaluation of possible variants in the decision-making process (MCDM, Multi-Criteria Decision-Making Methods). The TOPSIS Technique is based on the selection of the variant that is closest to the so-called optimal variant. The optimal or ideal variant is the one characterized by a vector of the best criterion values while being the furthest one from the so-called basal variant characterized as a vector of the worst criterion values. The TOPSIS Technique allows a complete arrangement of the set of all variants, and it is designed for selecting the best variant. 19
The specific procedure to calculate the ci indicator can be described via the following 5 steps:
1. The original criterion values yij are transformed to values rij according to the following formula:

2. This is followed by the calculation of the elements of the weighted criterion matrix W = (wij) as wij = vjrij, where vj is the weight of the j criterion.
3. From the elements of the criterion matrix W, the optimal variant is determined with the criterion values (H1, H2, . . ., Hk) and the basal variant is determined as well (D1, D2, . . . Dk), where Hj = maxi (wij) and Dj = mini (wij).
4. The next step includes the calculation of the distance of the variants from the optimal and the basal variant according to the following formulas:


5. The calculation of the ci indicator follows. This is the relative distance of the variants from the basal variant:

The resulting value of the ci indicator is from the interval <0,1>, where the value 0 is for the basal variant and the value 1 is for the ideal variant. The overall arrangement of variants can be obtained according to the decreasing values of the ci indicator.20,21
Results
The results are structured gradually, according to RT and RQ.
Dynamics and Relationships of Criteria of Psychiatric Care Deinstitutionalization
Selected criteria for deinstitutionalization of psychiatric care were analyzed using the average growth coefficient
The graph in Figure 1 shows that the dynamics of the criteria in the period studied are not always the same in the countries being compared. For criterion C1 expressing the number of patients receiving care on an outpatient basis, the dynamics in CZ is increasing (
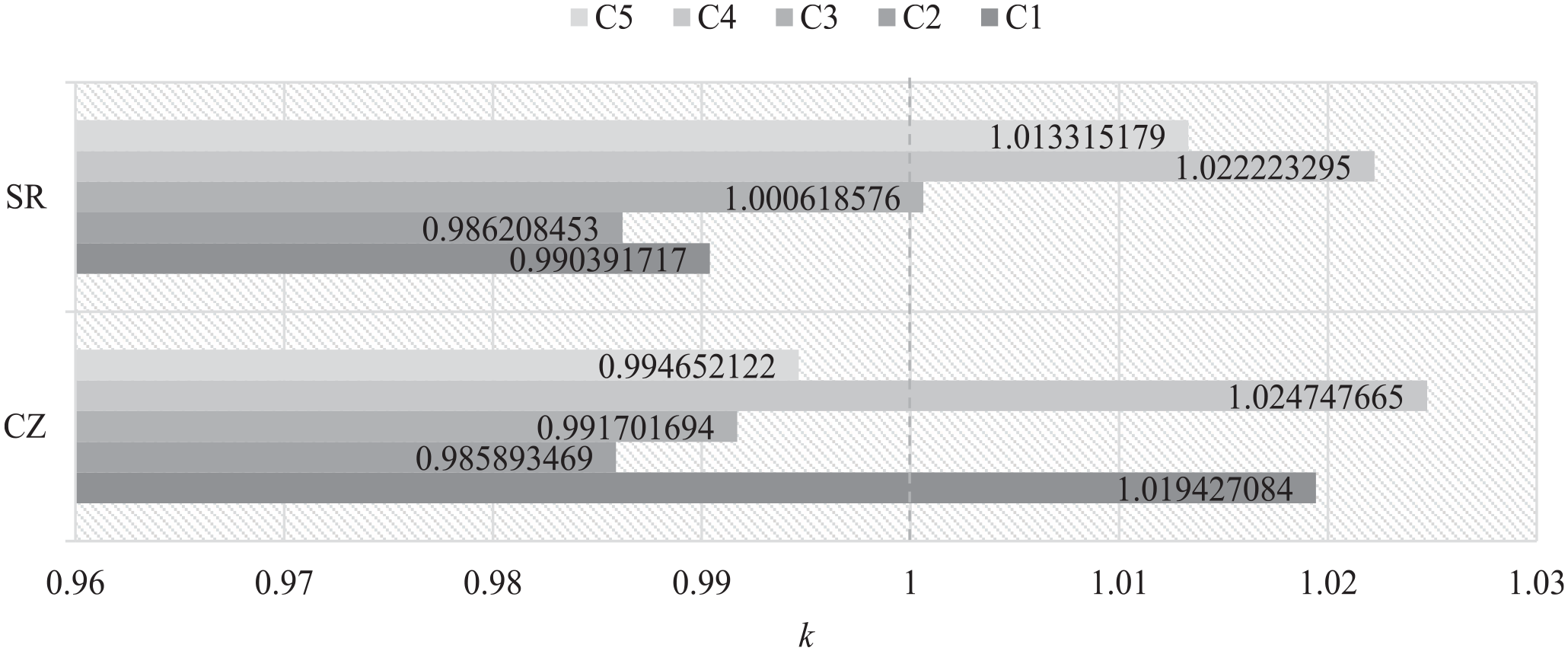
Growth coefficients of criteria C1-C5, period 2010to 2 020.
The direction of growth was disrupted in 2020, especially for criteria C2 in CZ and for criteria C1 and C2 in in SR.
The relationship between the criteria is monitored using the correlation coefficient r. In general, the correlation expresses the relative degree of the relationship in the mutual development of 2 time series yt and xt. The values of the correlation coefficient r are from the interval <−1; 1>. Values approaching the value −1 express that both monitored time series have completely opposite directions in their time development. Values of r approaching 1 show that the time series develop almost identically in terms of the same directions of their motions.
The correlation relationship calculated according to the Pearson correlation coefficient between the criteria C1-C5 (Table 2) is analyzed in the set including all the years and both countries, that is, 22 entries for each criterion (n = 22).
Pearson Correlation Matrix.

Correlation is significant at the .01 level (2-tailed).
Expected as well as unexpected positive/negative correlations were indicated between the criteria. The expected positive correlations include:
as the number of patients treated in outpatient clinics (C1) increases, the number of completed hospitalizations in hospitals and medical institutions (C2) increases as well and vice versa;
as the number of beds in hospitals and medical institutions (C3) increases, the number of physicians (C4) increases as well and vice versa;
as the number of physicians (C4) increases, the number of psychiatric outpatient clinics (C5) increases as well and vice versa.
An unexpected positive correlation is the following one:
as the number of beds in hospitals and medical institutions increases (C3), the number of psychiatric outpatient clinics (C5) increases as well and vice versa.
The expected negative correlations include:
as the number of patients treated in outpatient clinics (C1) decreases, the number of beds in hospitals and medical institutions (C3) increases and vice versa;
as the number of completed hospitalizations in hospitals and medical institutions (C2) decreases, the number of beds in hospitals and medical institutions (C3) increases and vice versa.
The unexpected negative correlations include:
as the number of completed hospitalizations in hospitals and medical institutions (C2) decreases, the number of physicians (C4) increases and vice versa;
as the number of completed hospitalizations in hospitals and medical institutions (C2) decreases, the number of outpatient clinics (C5) increases and vice versa;
as the number of patients treated in outpatient clinics (C1) decreases, the number of physicians (C4) increases and vice versa;
as the number of patients treated in outpatient clinics (C1) decreases, the number of outpatient clinics (C5) increases and vice versa.
Results of Multicriteria Analysis via the TOPSIS Technique
Based on the TOPSIS Technique calculation, the values of each variant were obtained, and the order determined. The places 1-11 are occupied by the variants of the SR, and the places 12-22 are occupied by the CZ variants (see Table 3). Based on this fact, it can be stated that the deinstitutionalization of psychiatric care in the context of the selected criteria developed differently in countries studied during the observed period.
Order of Variants According to the TOPSIS Technique.
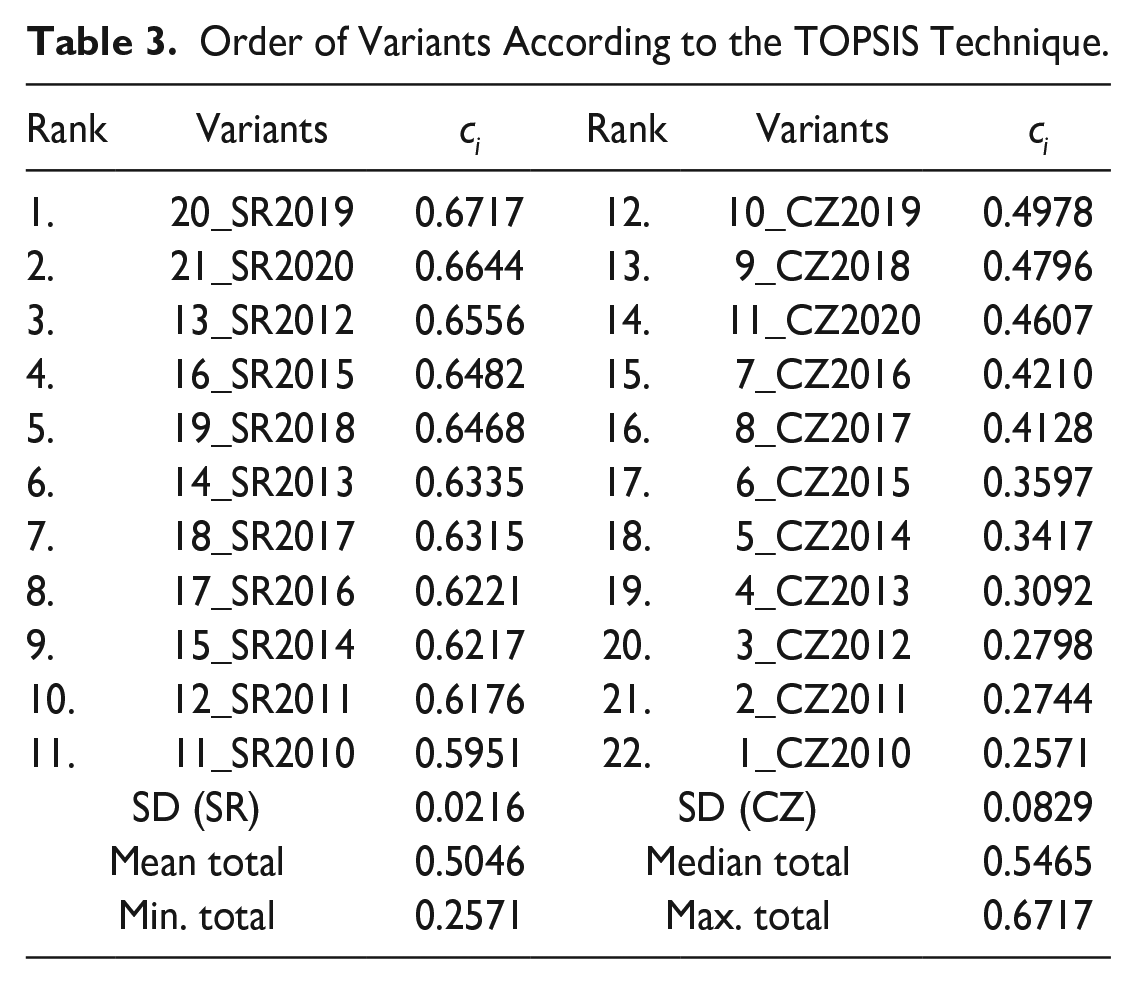
For the SR variants, it is not possible to unambiguously confirm the assumption that the variants from the second half of the observed period (2018-2020) have a better ranking. However, in the case of the CZ variant, this assumption was confirmed. In terms of the average value and median of ci for the whole set, the values of the CZ variants are all below the average and the median. On the contrary, the ci indicators of the SR variants are all above the average and the median of the set being evaluated. Thus, the results indicate a significant performance gap between the CZ and the SR.
In the CZ variants the trend is significantly consistently growing and in the SR variants the trend is less noticeable, and since 2012 fluctuations or stagnation of ci values can be observed. The difference between the best and the worst CZ variant is 94%. The difference between the best and the worst SR variant is 13%. In both countries, the best ci values were reached in 2019. The performance gap in the best year (2019) was 26%. In the first year of the evaluated period (2010), the performance gap was 56%. In the last studied year (2020), the performance gap was 31%.
The trend of deinstitutionalization in both countries can be deduced from the results of the TOPSIS calculations. If ci of the CZ and SR variants are evaluated partially, then during the observed period (2010-2020) the trend in both countries is different; for the CZ the trend is increasing and gradual, and for the SR the trend is slightly increasing and fluctuating. This is also confirmed by cluster analysis of ci for the variants and the analysis of their means.
Comparison of ci values of 22 variants using cluster analysis is captured by the dendrogram in Figure 2. The horizontal axis above the dendrogram describes the relative distance of clusters on a scale of 0 to 25, which has no factual meaning, only showing which variants are closer to each other than the others.

Dendrogram.
The dendrogram indicates 4 clusters (CLU1-CLU4):
The CLU_1 cluster includes 6 variants (CZ_2010, CZ_2011, CZ_2012, CZ_2013, CZ_2014, CZ_2015);
Cluster CLU_2 includes 5 variants (CZ_2016, CZ_2017, CZ_2018, CZ_2019, CZ_2020);
Cluster CLU_3 includes 6 variants (SR_2010, SR_2011, SR_2013, SR_2014, SR_2016, SR_2017);
Cluster CLU_4 includes 5 variants (SR_2012, SR_2015, SR_2018, SR_2019, SR_2020).
Discussion
The results of the multi-criteria analysis via the TOPSIS Technique confirm that the measures associated with the deinstitutionalization of psychiatric care are linked to the time they were introduced and the overall implementation period of the reform. Therefore, it is necessary to mention that the selected states followed a different timing and initiation of health policy in the field of mental health within the implementation of deinstitutionalization, but they also considered their specific economic and social conditions. Additionally, in the case of the Czech Republic and the Slovak Republic, the processes of psychiatric deinstitutionalization and their results are influenced not only by political decisions, but also by the ability of politicians and executives to achieve the planned goals of a given public policy. Endogenous factors include the degree of robustness and spatial availability of medical facilities, the number of medical staff, and the amount of public and private expenditures allocated to the provision of mental health care. 23 The numerous exogenous factors influencig the process of deinstitutionalization include the health status of the population, economic productivity and development, as well as the unexpected widespread health and social crisis situations (COVID-19, migration, energy crisis, etc.).
A multi-criteria evaluation of the development of deinstitutionalization on the example of selected 5 criteria also shows that the results achieved are useful for both public policy makers and the professional public. 24 The TOPSIS Technique is therefore a suitable tool for the initial detection of possible performance gaps and critical points during the time-consuming process of change or fulfilment of a strategic goal. The role of economists, as stated by Fuchs, 25 is to provide valuable inputs to health policy and health service research. The results of the calculation according to the TOPSIS Technique are limited by the selected period, when individual years are considered variants. The weights of the criteria determined according to Fuller’s method are the limit of results, because it is always possible to use other alternative methods. However, each research is always limited not only by a certain degree of simplification of reality, but also by its methodology, the choice of criteria, and the time. Selected criteria in a multi-criteria evaluation may therefore lead to a discussion related to their representativeness, level of detail, relevance, or suitability.
Deinstitutionalization of psychiatric care is not an easy topic. On the contrary, Novella 26 draws attention to the often-conflicting interests of various medical and social disciplines, which complicate this process and obscure the interests of patients. Therefore, in addition to the economic and social needs of providers and patients, deinstitutionalization is confronted mainly with the quality of care, as suggested by Salisbury et al 27 and Broulíková et al. 8 In the future, further research can be expected to respond to the possibilities and benefits of health information technologies (HITs) in the process of reforming and deinstitutionalizing psychiatric care, as assumed by LaMonica et al, 28 but also the impact of migration due to the war in Ukraine and the pandemics. Especially when deinstitutionalization in most countries is a long process with an unclear end, which is not always able to adapt effectively to the rapidly changing conditions of a technologically and economically advanced society. Similarly, Henckes, 29 summarizes the progress of psychiatric care reform in France between 1945 and 2010 and concludes that many mistakes and failures had to be made in order for the reform to be successfully completed.
Conclusion
The research is focused only on that part of the reform of psychiatric care, which addresses the reduction of long-term hospitalizations and the improvement of the availability of outpatient psychiatric care. Research is not focused on the implementation of community programs and the role of social services. This part of the reform of psychiatric care is at an early stage in both surveyed states and is still the subject of expert discussion.
The evaluation of the dynamics and gaps in the performance of deinstitutionalization of psychiatric care in the conditions of the Czech Republic and the Slovak Republic for the period between 2010 and 2020 was examined via a simplified model including 5 selected criteria. The research focused on 2 research topics and 5 research questions.
The first research topic (RT I.) evaluated the dynamics and mutual relationships of selected criteria of deinstitutionalization within the evaluated period (2010-2020). Using the average growth coefficient, it was analyzed whether the selected criteria developed the same way in the observed period in the CZ and the SR (see RQ1). A comparison showed of the dynamics of the criteria (Figure 1) that the dynamics of the monitored criteria is comparable for only 2 criteria, namely the number of completed hospitalizations and the number of physicians. Conversely, the dynamics are not the same for the number of outpatients, the number of beds, and the number of outpatient clinics. Also, the average relative values of the evaluated criteria show the different robustness of both systems (numbers of beds, physicians, and outpatient clinics) and the performance of these systems (numbers of patients in outpatient clinics and numbers of discharged patients). The relationship between the criteria was examined for the whole set and it can be stated that the differences described above were reflected in the results of correlation analysis, which revealed both expected, logical correlations and unexpected positive, but mainly negative correlations between the criteria (see RQ2).
The second research topic RT II. focused on detecting deinstitutionalisation performance gaps using the TOPSIS Technique and cluster analysis. The results of the multi-criteria evaluation according to the TOPSIS Technique showed that there is a significant performance gap between the CZ and the SR variants (see RQ3). The SR variants are clearly better than the CZ variants, although during the years studied, the CZ variants are improving, and the size of the gap compared to the SR variants is decreasing. In the first year of the evaluated period (2010), the performance gap was 56% and in the last year (2020), the performance gap was 31%. Both countries achieved the best results in 2019 and their performance decreased in 2020. The most likely explanation for the decreasing results in 2020 is the COVID-19 pandemic, when outpatient care was curtailed and inpatient care was strengthened. Slovakia achieved the best results in 2019, 2020, and 2012. The Czech Republic achieved the best results in 2019, 2018, and 2020. For these reasons, it can be stated that the best results were achieved at the end of the studied period only in the CZ, (see RQ4). The question of whether the trend of deinstitutionalization of psychiatric care in individual states can be derived from the results of the multi-criteria analysis via the TOPSIS model can be answered affirmatively (see RQ5). The dendrogram grouped the resulting values of variants into 4 clusters, 2 clusters representing CZ variants and 2 clusters of SR variants. In the case of the CZ clusters, the gradually improving trend of deinstitutionalization performance is clearly visible. In the case of Slovak clusters, variants from different years are mixed, which indicates a fluctuating (inconsistent) yet improving trend in deinstitutionalization performance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by project project TAČR ÉTA No. TL05000160, Economy-user potential of distance forms of social-health care of neurological and mental diseases; SGS No. SP2023/033, Evaluation of socio-economic factors of mental health of the population in the Czech Republic, Faculty of Economics, VSB – Technical University of Ostrava.
Ethics
Our study did not require approval by the ethics board because the subject of the solution and research does not include specific persons and the protected interests of other subjects. All methods were carried out in accordance with relevant guidelines and regulations.