
Abstract
The aim of this meta-analysis was to comprehensively evaluate the effectiveness of Diagnosis-related group (DRG) based payment on inpatient quality of care. A comprehensive literature search was conducted in PubMed, EMBASE, Cochrane Central Register of Controlled Trials and Web of Science from their inception to December 30, 2022. Included studies reported associations between DRGs-based payment and length of stay (LOS), re-admission within 30 days and mortality. Two reviewers screened the studies independently, extracted data of interest and assessed the risk of bias of eligible studies. Stata 13.0 was used in the meta-analysis. A total of 29 studies with 36 214 219 enrolled patients were analyzed. Meta-analysis showed that DRG-based payment was effective in LOS decrease (pooled effect: SMD = −0.25, 95% CI = −0.37 to −0.12, Z = 3.81, P < .001), but showed no significant overall effect in re-admission within 30 days (RR = 0.79, 95% CI = 0.62-1.01, Z = 1.89, P = .058) and mortality (RR = 0.91, 95% CI = 0.72-1.15, Z = 0.82, P = .411). DRG-based payment demonstrated statistically significant superiority over cost-based payment in terms of LOS reduction. However, owing to limitations in the quantity and quality of the included studies, an adequately powered study is necessary to consolidate these findings.
In an effort to minimize healthcare costs, diagnosis-related group (DRG) based payment has been widely applied for inpatient care worldwide. However, its effect on inpatient healthcare quality is inconsistent. Although a systematic review showed that DRG-based payment mildly improved the efficiency of healthcare by reducing the length of stay (LOS), its effects on quality of healthcare were mixed.
This study is significant since it employed an extensive search of electronic databases and included a reasonable number of studies using a relatively wide spectrum of DRG-based payment programs. The effect of DRG-based payment for healthcare quality and LOS was comprehensively analyzed.
The present meta-analysis was conducted to assess comprehensively the effectiveness of DRG-based payment on quality of inpatient care. The authors anticipate that the results of this review will be of value in facilitating shared decision-making and generating better practice guidelines for the implementation of DRG-based reimbursement system.
Introduction
The funds committed to health have been rising in recent years globally. Predictions report that spending will increase from US$7.9 trillion in 2017 to $11.0 trillion in 2030. 1 Between 2000 and 2015, the annual growth rate of healthcare spending was 4.0% while the global economy growth rate was 2.8%. 2 Hospital services expenses account for one of the largest shares of total healthcare expenses in all countries, regardless of their income level.3,4 Published findings report that the vast majority share of global medical supply and demand is increasingly coming from the Asia-Pacific region. 5 Additionally, low-income and middle-income countries are undergoing a sustainability crisis because of underlying health spending patterns. 6 However, decreasing out-of-pocket payments (OOP) can be effective in improving health expenditure per capita. 7 The provider payment method is an important measure to allocate healthcare resources. Therefore, coupled with the influence behaviors of both providers and receivers and to achieve goals of the health system, substantial efficiency gains could be made by reforming the hospital payment mechanisms. 8
Diagnosis-related groups (DRGs) based payment systems are a kind of hospital payment mechanism, along with fee for service, global budgets, capitation payments and a combination thereof. DRGs are defined as groups of patients that have similar clinical traits, such as age, gender, severity, complications and comorbidities, and resource consumptions, who incur comparable expenses.4,9 Therefore, many treated individual patients that are classified into the same DRG are medically and economically similar. In 1983, DRG-based payment was first introduced as a new prospective case-based reimbursement system for medical care in the US. Since then, a range of DRG-based systems have been widely applied for inpatient care worldwide in an effort to reduce healthcare costs, such as in Europe and fast-developing countries in Asia and sub-Saharan Africa. 10 Internationally, a total of 25 countries have implemented similar case-mix models.10,11 Under this kind of payment system, a hospital receives a fixed payment for each medicare patient, regardless of the actual cost for treating that patient. This will foster the transparency of hospital performance and resource consumption by standardizing reimbursement, and result in greater efficiency through decreasing avoidable services and improving productivity.12-14 Furthermore, the DRG-based system increases transparency, allowing comparisons across hospitals with respect to quality and efficiency, based on morbidity measured by the case-mix index of the hospital, and prospectively determines the patient OOP payments for inpatient care, which would limit burdening patients with costs. Previous studies on the payment system have revealed that DRG-based payment may slightly improve the efficiency and contain costs, without considerable negative impacts on quality of healthcare under close monitoring.8,15 Some evidence has indicated that even though DRG-based payment may slightly increase the efficiency, the equity and quality of healthcare are compromised, especially for patients exempted from this payment scheme.16,17 A systematic review also showed that DRG-based payment slightly improved the efficiency of healthcare by reducing the length of stay (LOS), but its effect on quality of healthcare was unclear. 18 Although the meta-analysis by Meng et al assessed the effectiveness of DRG-based payment on LOS and re-admission rates in inpatients, other quality of care related outcomes were not considered. 19
The substantial improvement in technological capacity in hospitals and the rapid development of the International Classification of Diseases (ICD) system has enabled the DRG-based payment system to be applied globally. Nevertheless, its effect on quality of healthcare and efficacy remains unclear. Prior relevant systematic review either only summarized the progress of DRG-based payment without examining its effect on medical care 20 or did not focus on DRG-based payment specifically. As a result, the number of relevant research is very limited. Therefore, the present meta-analysis was conducted to evaluate the effectiveness of DRGs-based payment on quality of inpatient care comprehensively. It is anticipated that the results of this review will be of value in facilitating shared decision-making and generating better practice guidelines for the implementation of DRG-based reimbursement systems.
Methods
Registration
This meta-analysis is registered on the International Prospective Register of Systematic Reviews (PROSPERO: CRD42020205465) and is compliant with the PRISMA (Preferred Reporting Items for Systematic Review and Meta-analysis) extension statement for network meta-analysis checklists. 21
Search Strategy
Two researchers independently searched PubMed, EMBASE, Web of Science, the Cochrane Central Register of Controlled Trials (CENTRAL), NHS Economic Evaluation, Global Health and Health Policy Reference Center from their inception to December 30, 2022 using the following keywords for DRG search: “diagnosis-related group*,” “DRGs,” “diagnosis related group*” and “case mix.” Keywords “GHM,” “DBC,” “HRG,” “LKF” were used for other patient classification-based payment systems. The complete search strategy is illustrated in Additional File 1: Appendix 1. Additionally, the search was supplemented by referring to the reference list of reviews to identify relevant reviews and any potentially eligible studies. There were no restrictions in terms of publication status or publication date.
Eligibility Criteria
Studies that met the following criteria were included. (1) Type of participants: Inpatients of all genders and age groups, with all kinds of diseases, with no restriction on type of clinical procedure. (2) Type of design: Study designs approved by the Cochrane Effective Practice and Organization of Care Group (EPOC): interrupted time series study (ITS), randomized controlled trials (RCTs), non-randomized controlled trials (non-RCTs), controlled before-after study (CBA), uncontrolled before-after study (BA), etc. (3) Type of interventions: Payment systems based on DRGs or other similar patient classification (ie, DBC, HRGs, LKF) that can be applied at institutional, regional, or individual level, in tertiary, secondary or primary care settings to reimburse inpatient services. Studies about the Japanese diagnosis procedure combination system (DPC), which was a mixed reimbursement system part prospective, part cost-based and had a flat-rate fee per diem based on diagnosis categories were excluded. 22 (4) Type of comparisons: Patients treated under cost-based payment. Pre-specified criteria for cost-based payment were defined as follows: (a) retrospective payment; (b) cost-based reimbursement of hospitals; (c) per service as the unit of payment. (5) Type of outcomes: Outcomes of interest included quality of health care (including re-admission within 30 days, in-hospital mortality, all-cause mortality, 30-day mortality, etc.) and efficiency (eg, LOS).
Studies that did not provide specific data, such as study protocols, conference proceedings or abstracts and commentaries were excluded.
Study Selection
The literature search records were managed using EndNote X7. In accordance with selection criteria, the 2 reviewers screened titles and abstracts of all articles identified for inclusion independently, following exclusion of duplicates. Studies having the potential to be included in the study and overlapping studies were subjected to full-text evaluation. Any disagreement between the 2 reviewers was resolved by discussion. In the case of lack of agreement, the final decision was provided by a third reviewer.
Data Extraction
Using a standardized data form, 2 reviewers independently retrieved data of the following baseline characteristics and outcome data of interest: first author name, year of publication, country, setting, diagnosis, outcome measures, sample size, mean age, method of estimation, payment and details of policy category for each country.
Risk of Bias of Individual Studies
The 2 reviewers independently assessed the risk of bias of the included studies. Risk of bias was assessed using the method described in EPOC.23,24 Then, the individual studies were classified as having a high risk of bias, low risk of bias or unclear. Furthermore, The Newcastle-Ottawa Scale (NOS) including selection, comparability and outcome quality parameters was used to assess the methodological quality of Cohort studies. 25 The quality of the included studies was evaluated separately for each item in the quality assessment table. If it was consistent, it received one point. If it was inconsistent, not sure and did not mention, it received zero points. The highest score of the NOS scale was 9. Any NOS score below 6 was rated as low quality, and NOS scores greater than 6 as high quality. Any variation in opinion between reviewers was resolved by discussion.
Statistical Analyses
Standardized mean difference (SMD) with 95% confidence interval (CI) was used to indicate the merger effect of outcomes presented as continuous variables. The cut-off point for statistical significance was P ≤ .05. Relative risks (RRs) and 95% CIs were used for dichotomous outcomes using the Mantel-Haenszel statistical method. Relative difference change with 95% CI was used for ITS outcomes, which were represented as changes along two dimensions: step change (the immediate effect of DRG-based payment) and change in slope (change with time that reflects the long-term effect of DRG-based payment). 26 The formula used to convert from absolute to relative difference change is included in Additional File 1: Appendix 2. Heterogeneity between results was assessed using the I 2 statistics and the Higgins I 2 test.27,28 A random effect model was used, if heterogeneity was statistically significant (ie, P < .05 or I 2 > 50%). Otherwise, a fixed effect model was used, and meta-regression and subgroup analyses were employed to measure heterogeneity. Subgroup analysis was conducted for the primary outcome between different study designs. Stata 13.0 (Stata Corporation, College Station, Texas, USA Stata) was used for all statistical analyses.
In the case that more than 2 studies were present in each subgroup, the analyses were based on the following factors: age (mixed age: studies enrolled all ages vs older age: studies enrolled ≥65 years only) and length of implementation of DRG (<2 vs ≥2 years). The interaction test of subgroup effects was calculated and Pinteraction was reported. Pinteraction <.05 suggested significant subgroup effects.
Results
Study Section
The initial search yielded 7711 potentially relevant references; removal of duplicate articles left 6056 articles. Based on the inclusion and exclusion criteria and screening by title and abstract, 113 records were selected for further screening by reading of the full text. Finally, 29 studies were included in this meta-analysis (Figure 1).
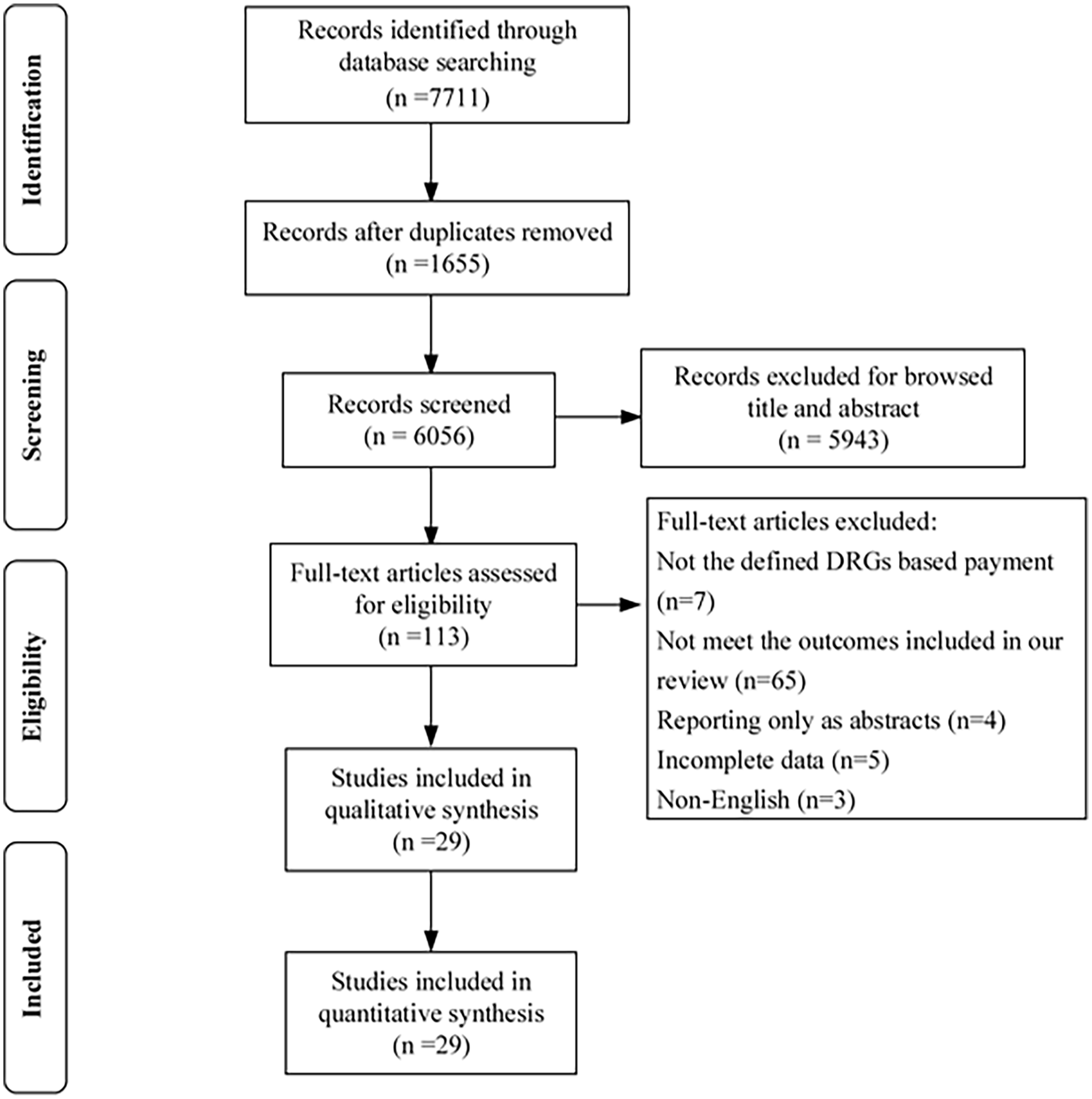
Flow diagram.
Study Characteristics
Fifteen cohort studies,29-43 nine CBA studies,44-52 and 5 ITS studies53-57 with a total of 36 214 219 patients were published between 1988 and 2019. Five studies (17.2%) focused on pneumonia, 5 (17.2%) on appendicitis and 3 (10.3%) on psychosis. The age of the participants ranged from 5 to 77 years and they were mainly from the United States, China, Korea, and Switzerland. DRG-based systems varied in implementation condition included, details of implementation and implementation time, such as starting year and study period. Seventeen studies reported full adoption of DRG, in terms of implementation condition and the median study period was 30 months. Among different countries, DRGs were implemented for different disease groups, with varying levels of complexity and substantial differences in reimbursement rates or prices. In total, 26 trials (89.7%) reported length of stay, 10 trials (34.5%) reported 30-day re-admission and 5 trials (17.2%) reported in-hospital mortality. More specific details on each trial are shown in Table 1.
Characteristics of Included Studies.

Note. CON = control; DRG = diagnosis-related groups; NA = not available; LOS = length of stay; AT = adenotonsillectomy; T = tonsillectomy.
Quality Assessment
All the 9 CBA studies were assessed to have high risk of bias in random sequence generation and allocation concealment. Two studies did not include sufficient information on baseline characteristics and outcome measurements. All studies showed low risks of bias in protection against contamination and outcome assessment. Differences were not explicitly reported between those that completed the intervention compared with those who did not in 3 studies and because of disparities in drop rates between the intervention and control groups, they were assessed as unclear risk of attrition bias. Two studies were assigned unclear risk of reporting bias. Among the ITS studies, one was assessed to be at high risk of bias that outcomes maybe affected by another policy of a restructuring of peer review organizations to monitor quality of care, combined with DRG-based payment. Among the cohort studies, 2 studies scored 6, 5 studies scored 7, and 8 studies scored 8. In the NOS scale for assessing the bias risk of a cohort study, there is the item “the results of follow up were long enough.” In this study, this item scored less than 40%. The remaining items scored more than 80%. Details of the risk of bias of the included studies can be found in Additional File 1: Appendix 3.
Meta-analysis
DRG and LOS
Seventeen of the examined studies, namely 12 cohort and 5 CBA studies. evaluated changes in LOS after DRG-based payment (Figure 2). A random model was applied to these studies, which showed that DRG-based payment was effective for decreasing LOS (pooled effect: SMD = −0.25, 95% CI = −0.37 to −0.12, Z = 3.81, P < .001) when compared with cost-based payment. DRG-based payment was associated with a drop in LOS in cohort studies (SMD = −0.25, 95% CI = −0.38 to −0.11, Z = 3.59, P < .001). Evidence of a subgroup effect was discovered, in which the association of DRG-based payment and LOS existed in the length of implementation of DRG less than 2 years but not for 2 years or more (SMD: −0.15, 95% CI −0.56 to −0.27 in the length of implementation of DRG 2 years or more; SMD: −0.05, 95% CI −0.05 to −0.05 in the length of implementation of DRG less than 2 years; Pinteraction<.001). However, no differences in age were identified in the subgroup analysis (Pinteraction = .093). The meta-analysis of CBA studies did not show a significant decrease in LOS after the implementation of DRG-based payment (SMD = −0.19, 95% CI = −0.72 to 0.33, Z = 0.72, P = .474). Five ITS studies showed that DRG-based payment was associated with a significant drop in LOS (RDC = -10.76, 95% CI = −18.54 to −2.98, Z = 2.71, P = .007) (Supplemental Figure 1). No suggestions of subgroup effects were discovered in DRG length of implementation (Pinteraction = 0.262) (Supplemental Tables 1 and 2-Appendix 4). Finally, LOS of inpatients with appendectomy was found to decrease after the implementation of DRG-based payment (Supplemental Figure 2).

Meta-analysis for the effect estimate of DRG based payment on LOS.
DRG and Readmission
Seven cohort studies reported the association between DRG-based payment and re-admission within 30 days. As seen in Figure 3, meta-analysis showed no significant overall effect in readmission within 30 days after the implementation of DRG-based payment (RR = 0.79, 95% CI = 0.62-1.01, Z = 1.89, P = .058). The meta-analysis of 3 studies did not reveal a significant increase in re-admission rates of inpatients with a main diagnosis of either community-acquired pneumonia, acute heart failure or exacerbation of COPD diseases after the implementation of DRG-based payment (Supplemental Figure 3). No significant subgroup effects were discovered for all subgroup factors (length of implementation of DRG: Pinteraction = .616; age: Pinteraction = .248) (Supplemental Tables 1 and 2- Appendix 4).

Meta-analysis for the effect estimate of DRG based payment on readmission rates.
DRG and Mortality
Only 3 cohort studies reported the association between DRG based payment and in-hospital mortality. Nevertheless, meta-analysis showed no significant overall effect in mortality after the implementation of DRG-based payment (RR = 0.91, 95% CI = 0.72-1.15, Z = 0.82, P = .411) (Figure 4).

Meta-analysis for the effect estimate of DRG based payment on mortality rates.
Discussion
This meta-analysis evaluated the available reports on the implementation of DRG-based payment in inpatient quality of healthcare. Integrating the currently available data, the present study showed a significant decrease of LOS for the patients after the implementation of DRG-based payment. However, no compelling evidence for negative consequences was hereby identified in terms of re-admissions or in-hospital mortality, even though some literature raises the possibility of detrimental effects on these outcomes under some circumstances.
The present meta-analysis results demonstrated that DRG-based payment could reduce the LOS, which is consistent with the policy expectations and is theoretically plausible. 19 Multiple systematic reviews have consistently established that DRG-based payment resulted in a significant reduction in the LOS.15,17,19 LOS results differed when subgroup analysis by length of implementation of DRG was performed, which might be attributed to time lags between DRG-based payment implementation and any subsequent change in the patient outcome. Similarly, prior literature has reported that DRG-based payment initially decreased LOS, but it seemed to stabilize after the initial decrease.58-60 Long LOS is often associated to profit maximization, under hospital reimbursement with a fixed price per case, while long LOS is related to a decrease in average profits under DRG-based payment. Therefore, the implementation of a DRG-based system may have stimulated behavioral changes, which led to more efficient discharge planning. In line with this aspect, decreasing LOS may have a favorable impact on the cost per case, and the efficiency will be increased, leading to higher productivity and profits for a hospital under the DRG-based payment. 39 Additionally, earlier research has demonstrated that inappropriate premature discharges increased under DRG-based payment to reduce costs and pursue excessive hospital profits.50,61-64 Notably, reducing LOS suggests that it may have an adverse impact on quality of healthcare through early discharges and the reduction of service intensity to a level at which necessary services are withheld from patients. 65 However, Jian et al showed that LOS was not reduced after implementation of DRG-based payment. 51 Thommen et al arrived at similar conclusions in their review that LOS remains stable or even tends to increase shortly following implementation of SwissDRG. 37 Therefore, care should be exercised to ensure that the new system does not lead to degradation of medical service quality. 66 Consequently, larger, adequately powered studies that are designed to assess the impact of DRG-based system on LOS are required to confirm this positive finding.
No overall effect on re-admissions after the implementation of DRG-based payment was revealed in this meta-analysis, which is consistent with previous reports, such as those of Epstein et al 67 and Palmer et al. 17 Another study in Korea 36 found that DRG payments decreased the LOS without increasing re-admission rates. Likewise, other studies reported no significant differences in re-admission and mortality following implementation of the system.45,50,58 The evidence may be obscuring a true increase in re-admissions. To maintain healthcare quality, hospitals would naturally increase the number of outpatient visits, which could lead to the unintended results of increasing re-admission rates due to operative complications. Hamada et al 22 reported that the introduction of the DRG-based system increased the rate of re-admissions. On one hand, in response to earlier discharge, physicians that intensified their follow-ups may account for the reduction in re-admission. On the other hand, because readmission within 30 days is suggested as an important indicator of healthcare quality, hospitals in high competition areas strive to decrease re-admission.68,69 Because the eligible studies included were performed in comprehensive medical areas or different medical fields, may be the reason why the results on re-admission rates are inconsistent. 70 Besides, the ways in which the hospital payment reform affects the patients’ quality of health care remain unclear. Further high-quality studies are needed to monitor rigorously and report carefully on the association of DRG-based payment with re-admission.
This review discovered no consistent impact of DRG-based payment on in-hospital mortality in patients. This finding was consistent with the scoping review finding of Brügger and Eichler 15 in their analysis of international experience in 2010, which revealed minimal change in death rates when DRG-based systems were introduced. In contrast, in a review from OECD countries, 71 the introduction of DRG-based systems was associated with slower quality gains with respect to mortality from surgical and medical adverse events. Despite the confirmed benefits of DRG on quality, evidence on the effect of DRG-based system on in-hospital mortality in inpatients was not corroborated in this review, likely because of poor study quality and small sample size. Furthermore, quality outcomes, in terms of mortality and re-admission rates, are useful indicators for DRG-based payment measuring but have been criticized as insufficiently sensitive in the quality of healthcare. 72 In addition, the validity of in-hospital mortality as a quality metric has been called into doubt, as physicians may choose to discharge patients with terminal disease to nursing homes under the implementation of prospective payment system.39,73 Moreover, increasing hospital awareness of cost control through just the DRG-based system and without specific efforts to promote quality, including the level of training received by healthcare professionals and interaction time between patients and physicians, introduces difficulties in quality of medical care enhancement. 52 Therefore, drawing firm conclusions regarding the association of DRG-based payment with in-hospital mortality in inpatients becomes difficult. The number of eligible studies included on mortality analysis was small, and many related reviews did not collect or report this information, making it obvious that more high-quality studies are required before conclusions can be drawn.
The present study has the following limitations. First, some studies were not included because of limitations in data availability, even though accessible database resources and references were searched for to the best of our ability. Additionally, significant heterogeneity was detected, which may be caused by differences in factors, such as different design of DRG based system, different treatment environment for participants and different study designs used to confirm the outcomes. Despite this, a random effect model was used to pool the results of the captured studies and subgroup analyses were conducted to explore the sources of heterogeneity. Third, the majority of the eligible studies were before-after studies. Because hospital funding reform is rarely implemented as a separate intervention, considerable differences may be the results of temporal trends independent of DRG. Finally, the results of this review may not be robust as they are dependent on the quantity and quality of the literature available currently, which may change in the future. Future higher quality research in this field might modify the presented conclusions.
Nonetheless, the contribution of this study is that it used an extensive search of electronic databases and included a reasonable number of studies using a relatively wide spectrum of DRG-based payment programs. The effect of DRG-based payment for quality of healthcare was also comprehensively analyzed, including 30-day re-admission, in-hospital mortality all-cause mortality and LOS.
Conclusion
The results of this meta-analysis indicated that Diagnosis-related group (DRG) based payment has a positive effect on length of stay but no effect on inpatient mortality and re-admission rates. Current knowledge on the effects of DRG-payment on quality of medical care is primarily based on studies in patients with mixed diagnoses. Furthermore, owing to limitations in the quantity and quality of the included studies, future studies with larger sample size and well-controlled confounding factors are required to confirm the presented findings.
Supplemental Material
sj-doc-5-inq-10.1177_00469580231167011 – Supplemental material for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis
Supplemental material, sj-doc-5-inq-10.1177_00469580231167011 for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis by Ya-jing Chen, Xin-yu Zhang, Jia-qi Yan, Xue-Tang, Meng-cen Qian and Xiao-hua Ying in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-4-inq-10.1177_00469580231167011 – Supplemental material for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-4-inq-10.1177_00469580231167011 for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis by Ya-jing Chen, Xin-yu Zhang, Jia-qi Yan, Xue-Tang, Meng-cen Qian and Xiao-hua Ying in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-1-inq-10.1177_00469580231167011 – Supplemental material for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-inq-10.1177_00469580231167011 for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis by Ya-jing Chen, Xin-yu Zhang, Jia-qi Yan, Xue-Tang, Meng-cen Qian and Xiao-hua Ying in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580231167011 – Supplemental material for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-2-inq-10.1177_00469580231167011 for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis by Ya-jing Chen, Xin-yu Zhang, Jia-qi Yan, Xue-Tang, Meng-cen Qian and Xiao-hua Ying in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-tif-3-inq-10.1177_00469580231167011 – Supplemental material for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis
Supplemental material, sj-tif-3-inq-10.1177_00469580231167011 for Impact of Diagnosis-Related Groups on Inpatient Quality of Health Care: A Systematic Review and Meta-Analysis by Ya-jing Chen, Xin-yu Zhang, Jia-qi Yan, Xue-Tang, Meng-cen Qian and Xiao-hua Ying in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank all members of our study team for their whole-hearted cooperation and the original authors of the included studies for their wonderful work.
Author Contributions
YJC, XYZ, and XHY planed and designed the research; YJC, JQY, and MCQ provided methodological support/advice; YJC and JQY tested the feasibility of the study; YJC, XYZ, JQY, and XT extract data; YJC and XYZ performed the statistical analysis; YJC wrote the manuscript; YJC, ZXY, MCQ, and XHY revised the manuscript; all authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation (NSFC) of China (Grant number 72074051), and National Healthcare Security Research Center of Capital Medical University (Grant number YB2020B01). The views expressed are those of the authors and not necessarily those of the Fudan University. The funders had no role in the study design, data collection, data synthesis, data interpretation or writing of the report.
Available of Data and Materials
The datasets and any other materials of our study are available from corresponding author on request.
Ethics Approval and Consent to Participate
Ethics approval and participants consent are not required because this study is a meta-analysis based on the published studies.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.