
Abstract
Male homosexual behavior dominates the mode of HIV infection among students in China. This study aims to identify factors associated with HIV risk behaviors among male students who have sex with men (student MSM) aged 15 to 19 in China. The online sampling used the standard respondent-driven sampling (RDS) method, with recruitment support from community-based organizations (CBOs) in Tianjin and Guangzhou. Multivariate logistic regression models were performed to identify factors associated with multiple HIV risk behaviors. A total of 449 subjects were recruited in this study, including 206 in Tianjin and 243 in Guangzhou. The presence of multiple HIV risk behaviors among student MSM, in many cases, was found to positively correlate with parental or friends’ awareness of their same-sex sexual behavior or sexual orientation, with some geographical differences. The prevalence of HIV risk behaviors among student MSM aged 15 to 19 was high and associated with the disclosure of their sexual orientation or their sex with males to parents and friends. These findings highlight the importance of addressing social support in HIV prevention among student MSM when delivering HIV-related education or services.
In China, newly reported HIV cases among students came mainly through male homosexual behavior.
This research found that student MSM who disclosed their sexual orientation or their sex with males to parents or friends were more likely to engage in multiple HIV risk behaviors than those who did not.
Our findings highlight the role of social support in influencing the risky sexual behaviors of student MSM. When developing a curriculum for HIV prevention education or sexuality education, and when developing youth sexual health services, the influence of peer relations and parental relationships needs to be considered. Future research should further explore how to positively engage parents or peers to foster safe sex behavior among student MSM.
Introduction
Globally, the proportion of adolescents and young people among people living with HIV shows an increased trend. 1 In China, the number of newly diagnosed HIV cases among youth aged 15 to 24 increased from 9373 in 2010 to 15 790 in 2019. 2 In the recent 5 years annual reported new HIV infections among students in China have remained at above 3000 cases. 3 More than 80% of newly reported HIV cases among students were men who have sex with men (MSM). 4 Adolescent MSM (AMSM) are at high risk of HIV infection. The risk perception among adolescents is usually low, coupled with sexual curiosity, which may lead to high-risk behaviors. According to a study conducted in 8 cities among MSM in China, compared with the incidence of HIV infection among young MSM aged 21 to 25 years, the incidence in MSM aged 18 to 20 is relatively high. 5
The characteristics of HIV-related behaviors among student MSM in China have not been thoroughly studied. In 2018, an online survey was conducted among MSM aged 15 to 19 in 2 cities in China, to measure HIV-related sexual risks and practices to better plan prevention programs and services. 6 The results of this survey show that the risks of HIV infection among MSM aged 15 to 19 are extremely high. 6 This study is a secondary analysis based on the survey, however with a focus on student MSM in particular. As student MSM provide a unique and critical window of opportunity for delivering standardized and centralized health interventions, we need to take the opportunity to prioritize sexual and reproductive health education among young students, especially student MSM among them, via campaigns and interventions on preventing HIV and sexually transmitted diseases (STDs), with concerted efforts of health and education departments. 3
Methods
Study Design, Population
This cross-sectional study was carried out in 2018 using online standard respondent-driven sampling (RDS) methods.7,8 The inclusion criteria of participants were: (1) male, (2) aged 15 to 19, (3) having had oral or anal sex with men in the past 12 months, and (4) living in Tianjin or Guangzhou.
A total of 546 (Tianjin: 258, Guangzhou: 288) participants meet the inclusion criteria. 6 As this secondary analysis focused on respondents who reported being students, 449 eligible subjects were included in the data analysis.
Study Site
Considering the difficulties of AMSM recruitment, this study was conducted in Tianjin and Guangzhou, both program sites of the China Comprehensive AIDS Response Program and where community-based organizations (CBOs) are well established.
Tianjin Municipality is located in northern China, with a population of about 13 million. In Tianjin, about 650 new infections were diagnosed in 2020, most of which were infected through male homosexual behaviors. 9 Guangzhou City, the capital of Guangdong Province in southern China, has a population of about 18 million. The HIV prevalence among MSM in Guangzhou is high. 10
Study Procedures
Due to the hidden nature and vulnerability of AMSM and the popularity of online social networks among this age group in China, this study used a web-based peer-to-peer probability-based sampling technique using WeChat, a Chinese multi-purpose messaging, social media, and mobile payment app, based on which an online program was designed, accessible via quick response (QR) code, and rolled out by CBOs in the 2 cities. The initial seed selection was crucial for RDS sampling. In this survey, persons with large social networks were selected as the initial seeds. Respondents were then requested to provide informed consent, and complete the online questionnaire, after which they were given an 8-digit password for an online payment of 30 CNY (~4.36 USD) via Alipay, administered by the survey software manager. A self-administered online structured questionnaire was used to collect each participant’s sociodemographic information, including socio-demographic characteristics (including age, education level), sex behaviors (condom use during sex, multiple sex partners, group sex, drug use before anal sex, buying sex, selling sex), and social support (homosexual orientation or behavior disclosure to friends, parents).
After completing the questionnaire, the respondent received up to 5 coupons with unique QR codes which were used to recruit eligible peers into the survey. Respondents received an additional incentive of 30 CNY (~4.36 USD) for each person they recruited who enrolled and completed the survey, delivered to the respondents in the same manner. The detailed method of sampling, survey, and data collection is published elsewhere. 6
Statistical Analysis
Sampling weights estimated in RDS Analysis software were applied to univariate and multivariate logistic regression analyses. Logistic regression was performed to identify factors (education level, friends’ awareness, parental awareness, and HIV education) associated with multiple HIV risk behaviors (inconsistent condom usage, multiple partners, group sex, drug use before anal sex, buying sex, and selling sex). A univariate logistic regression analysis was first performed. All variables were selected into the final multivariate logistic regression model to calculate adjusted odds ratios (aOR). The SAS software (version 9.4, SAS Institute, Cary, NC) was used for data analysis.
Ethics Statement
Informed consent was obtained before the investigation. The study has been approved by the Ethics Committee of the National Center for AIDS/STD Control and Prevention, Chinese Center for Disease Control and Prevention (Project No: X170623465).
Results
Demographic, Social Support, and Sexual Behavior Characteristics of Respondents
A total of 449 subjects were recruited for this study, including 206 in Tianjin and 243 in Guangzhou (Table 1). Most student MSM recruited in Tianjin and Guangzhou were 19 years old, and 17 years old, respectively (P < .001). The majority of respondents in Tianjin have a college level of or above (55.6%), while the majority of respondents in Guangzhou were in senior and technical secondary school (P < .001).
Demographic, Social Support, and Sexual Behavior Characteristics of Respondents in Tianjin and Guangzhou (N = 449).

In terms of social support, there is a low level of parental awareness of their sexual orientation (Guangzhou: 30.2%, Tianjin: 13.9%, P < .01). Moreover, the weighted proportion of friends’ awareness was relatively higher than parental awareness, with 44.8% in Guangzhou and 58.9% in Tianjin.
Regarding HIV prevention education and sexual behavior, the proportion of respondents in Tianjin who had ever received HIV prevention education; had consistent condom use; chose to have a single sex partner; had group sex; or who bought or sold sex were lower than those in Guangzhou. The differences were statistically significant (P < .05).
Factors Associated With Multiple HIV Risk Behaviors
In Tianjin, respondents whose parents knew about their sexual orientation were more likely to have inconsistent condom use (aOR = 3.08, 95% CI: 1.01-9.37), engage in group sex (aOR = 7.38, 95% CI: 2.40-22.68), and selling sex (aOR = 16.57, 95% CI: 4.33-63.47) (Table 2). Respondents whose friends knew about their same-sex sexual behavior were significantly associated with selling sex (aOR = 11.40, 95% CI: 1.63-79.86). Furthermore, those who received HIV education were associated with increased odds of group sex (aOR = 4.85, 95% CI: 1.52-15.46).
Factors Associated With Multiple HIV Risky Behaviors Among Respondents in Tianjin and Guangzhou (N = 449).
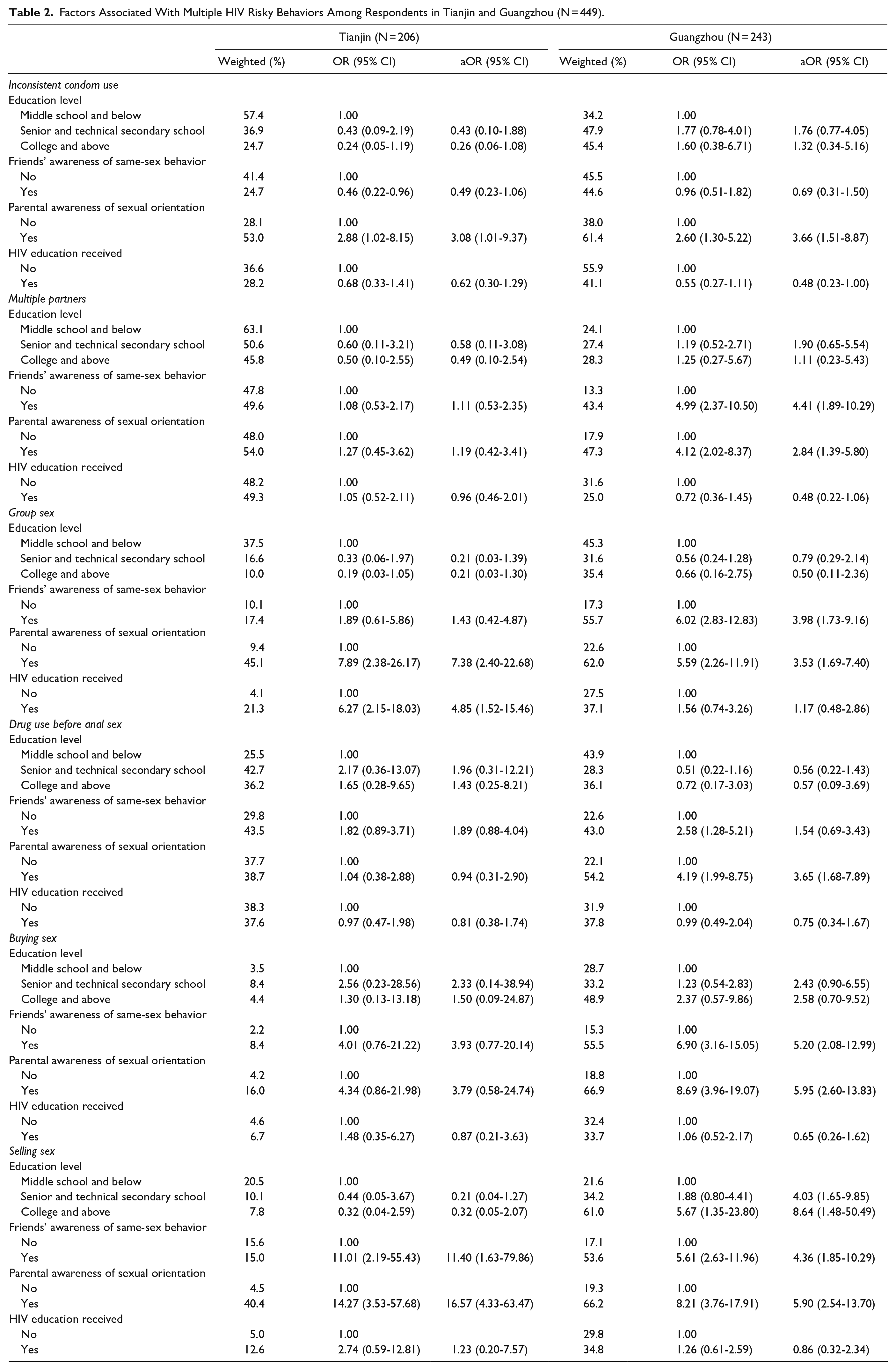
In Guangzhou, respondents whose parents knew about their sexual orientation were more likely to have inconsistent condom use (aOR = 3.66, 95% CI: 1.51-8.87), multiple sex partners (aOR = 2.84, 95% CI: 1.39-5.80), engage in group sex (aOR: 3.53, 95% CI: 1.69-7.40), drug use before anal sex (aOR = 3.65, 95% CI: 1.68-7.89), buying sex (aOR = 5.95, 95% CI: 2.60-13.83), and selling sex (aOR = 5.90, 95% CI: 2.54-13.70). Respondents whose friends knew about their same-sex sexual behavior were significantly associated with multiple sex partners (aOR = 4.41, 95% CI: 1.89-10.29), engage in group sex (aOR = 3.98, 95% CI: 1.73-9.16), buying sex (aOR = 5.20, 95% CI: 2.08-12.99), and selling sex (aOR = 4.36, 95% CI: 1.82-10.29). Furthermore, respondents with senior and technical secondary school educational levels were associated with increased odds of selling sex (aOR = 4.03, 95% CI: 1.65-9.85). In addition, respondents with college and above educational level were more likely to sell sex (aOR = 8.64, 95% CI: 1.48-50.49).
Discussion
This study, using the online RDS method among student MSM in two China cities, identifies the characteristics of their HIV risk behaviors and associated factors. As young students move into vocational schools or universities, they are exposed to a less restrictive, more open learning environment, away from family and parents. They are curious about their new life and new environment, happy to be free of family constraints, but they often lack awareness of self-protection. Some start pursuing a more stimulating physical and psychological life or try to experiment with what they think is trendy, ignoring the prevention of physical or emotional harm. As a previous study conducted among student MSM in northern China shows, younger MSM exhibit higher unprotected sexual behaviors, which may have the potential to increase the spread of HIV. 11
In this study, the percentages of MSM whose parents are aware of their same-sex sexual behavior or sexual orientation in Tianjin and Guangzhou (13.9%, 30.2%) are significantly lower than the percentages of friends (58.9%, 44.8%) with this awareness, an indication that student MSM are more willing to share information on their sexual behavior with friends than with their parents. For this reason, training peer educators and engaging them in promoting safer sex among young students will achieve a greater effect than the same efforts with parents. MSM with better self-acceptance are more likely to have multiple sexual partners than those with poor self-acceptance. 12 Some student MSM gradually took “multiple sexual partners” and “open sexual relationships” as “gay circle culture,” thus increasing their own risk of HIV infection. 13 It is therefore particularly important to provide comprehensive sexuality education to help “develop accurate and age-appropriate knowledge, attitudes and skills; positive values, and attitudes and skills that contribute to safe, healthy, positive relationships. 14
Due to the low public acceptance of homosexual behavior, students may be reluctant to “come out.” Moreover, MSM who disclose their sexual orientation may face homosexuality-related stigma, discrimination, and social exclusion.15-17 It is worth noting that a higher percentage of parental awareness is not associated with a higher percentage of friends’ awareness. A possible explanation may be that MSM who had disclosed their sexual orientation to friends feel some emotional relief and therefore feel less inclined to open up to parents.
Student MSM is a priority group in HIV prevention and control in colleges and universities. Differences in basic characteristics and HIV risk behaviors among student MSM aged 15 to 19 in Tianjin and Guangzhou may be attributed to geographical differences in culture and customs between the north and the south. Therefore, HIV prevention campaigns and sexuality education for young students should, first of all, be based on needs assessment, taking into account the general needs of students, needs of key populations as well as regional differences, using targeted education and interventions that reflect the different geographical and population characteristics and local characteristics, to make it more effective.
As student MSM often engage in multiple risk behaviors that put them at risk of HIV infection, sexuality education, including education on how to prevent HIV and STDs, and the connection between recreational drugs and HIV transmission, should start before they engage in such behaviors, preferably as early as in junior middle school. No correlation was found, however, between inconsistent condom use and educational level or whether they ever received HIV prevention education. It may indicate that when addressing adolescent MSM in HIV/STD prevention education, one-size-fits-all knowledge is not enough. The geographical difference in student MSM behaviors should be considered, based on which different content, teaching style, and targeted interventions are provided, all working together to promote behavior change. The need to start early with school interventions on adolescents is reflected in the Implementation plan to curb the spread of HIV (2019-2022) issued by 10 government ministries including the National Health Commission and the Ministry of Education. The Implementation Plan clearly states that “in middle schools and secondary vocational schools, we need to provide education on sexual ethics, sexual responsibility, refusal of unsafe sex, and refusal of drugs, and guide students to establish a healthy attitude toward sex. School clinics and school counselor services can offer physical and psychological counseling services related to sex. 18 Strengthening students’ awareness of HIV risks, sexual ethics, and self-protection skills, prevent or to the greatest extent reduce HIV risk behaviors. At the same time, teachers should be trained in the delivery of sexuality education, and in understanding and responding to the diverse needs of students. Teachers should also be able to provide knowledge and skills on condom use, and on how to avoid unsafe sex when providing sexuality education. In doing so, they need to be fully sensitized about the impact of students’ social relations on their sexual behaviors, to ensure more comprehensive and effective education and interventions. Disconnection of HIV knowledge and behavior will put student MSM at greater risk for HIV infection. 19 Therefore, schools should go further than disseminating prevention knowledge, by strengthening targeted interventions, understanding the disconnection of knowledge and behavior, and building upon the correct knowledge with needed skills for safe sex, and the ability to sustain safe sex practices. For example, using new approaches such as internet-plus interventions and internet-plus testing in helping students recognize behaviors that might put them at risk of HIV/STD infection, make self-assessments of risks for infection to decide if testing is needed, as well as know where and how to find support when needed.
Although some national and international studies suggest that tailored sexuality education by parents could increase the likelihood of HIV testing among student MSM, 20 or that communication on sexuality with parents can be a protective factor in safe sex among young adolescents. 21 Our study, on the contrary, shows that when parents or friends know about their same-sex sexual behavior, the likelihood of their engaging in risky behaviors increases. A possible explanation is that after an adolescent MSM discloses to his parents and friends about their same-sex sexual behavior or sexual orientation, they let go of their psychological burden and no longer restrain their behavior and are more likely to have risky sexual behaviors. Additionally, scholars have noted that when gay/bisexual men come out to their parents, they might experience greater levels of stigma and rejection and be cut off from the parental relationship. In turn, they might be more likely to engage in risky behavior as a coping mechanism. Therefore, it is important to consider parents’ positive or negative reactions in future studies. 22 Student MSM may be more likely to have certain psychological problems, which are influenced by childhood family environment to a certain extent, suggesting that family environment plays an important role in the growth of adolescents. 23 Historical reasons can explain the lack of sexuality education for the parent generation. Therefore, it is particularly important to update Chinese parents with fact-based information on sexuality and HIV, so that they can better accept and support their children. As a next step, further study should be conducted on how to address the specific needs of student MSM when providing prevention knowledge and interventions in school, while paying more attention to the impact of social relations on their risk behaviors.
This study shows a relatively high prevalence of HIV risk behaviors among student MSM aged 15 to 19. It suggests that HIV publicity campaigns and education for young students should not only impart knowledge about HIV prevention and treatment in schools, but also combine school education with family education, and focus on sexuality education, sexual ethics, sexual responsibility, and avoiding unsafe sex. Different contents and forms of publicity and education materials and forms of education should be designed for students of different ages, different school periods, and different infection risks. In the meantime, skills should be taught on negotiating with partners for safe sex and communicating with parents and friends to seek social support.
This study has several limitations. First, answers to the questions are retrospective, and recall bias is inevitable. Nonetheless, the information collected can shed light on how to achieve greater effectiveness in the provision of sexuality education and HIV prevention publicity campaigns, education, and intervention for the student MSM population. Second, selection bias may exist when sampling. 24 Third, sample size calculations were not performed before the investigation, which may lead to an insignificant relationship between some variables and outcomes.
Conclusion
The prevalence of HIV risk behaviors among student MSM aged 15 to 19 years is high. Our study demonstrated that disclosure of sexual orientation to friends or parents was positively associated with HIV risk behaviors, Thus, policies facilitating more targeted sexuality education and health services are recommended, not only to address risky behaviors but also to investigate the role of social support from family and friends. Furthermore, the underlying factors related to HIV risk behaviors among student MSM, including the impact of their social networks and social support, should be further studied.
Footnotes
Acknowledgements
We would like to show our gratitude to Zhang Haichao and Cai Lingping of Beijing Kangzhong Health Education and Service Center for the design and management of the online system for this web based survey, and we thank Wang Liqiu, an independent researcher and programme specialist, and Liu Peng of the Chinese Association for STD/AIDS Prevention and Control for their insight and technical advice. Many thanks to Mr. Jacob Wood for manuscript polishing and improvement. We are immensely grateful to UNICEF China and UNICEF East Asia and Pacific Regional Office for their generous funding support and technical advice, and to Professor Lisa G. Johnston of Tulane University, USA, and to the Global AIDS Programme (GAP), United States CDC, China Office for their technical expertise around this subject matter.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by UNICEF China.