
Abstract
To review the effects of Otago exercise program (performed individually or in group) on several physical and psychosocial outcomes for community-dwelling and institutionalized older adults. Fourteen articles met the inclusion criteria. Three electronic databases and reference lists of identified studies were searched. Eligibility criteria included clinical trials of the Otago exercise program conducted among older adults. Two studies were conducted in institutions, 2 in groups. None of the studies reviewed reported the post-intervention result of the Otago exercise program on depression or any other psychological construct. Otago exercise program was effective in reducing falls, improving balance, strength, mobility, and health-related quality of life within the community and in institutions. Available evidence suggests group performance may be better than individual programs. The Otago exercise program is an important and effective exercise strategy which can be administered in groups or individualized to both community-dwelling and institution-resident older adults. Future reviews, especially, systematic reviews with meta-analysis should be performed.
The effectiveness of the Otago Exercise Program on fall intervention
This review would provide evidence based data on the effectiveness of the Otago Exercise Program on physical and psychosocial functions among older adults in the community and institutions.
Health care professionals and researchers would have available to them information on variables that have been explored using the Otago Exercise Program. It would also help policy makers in formulating policies for older adults to ensure healthy/active aging.
Introduction
Globally, falls and their consequences continue to be significant public health challenges for the older adult population, caregivers and health care providers.1-3 Approximately one-third of older adults fall at least once every year as a result of intrinsic and extrinsic risk factors. 4 The risk of falls can increase due to an interaction of multiple factors related to aging such as depression, reduced muscle strength, balance, and gait changes.5,6 Fall is a common cause of injury, morbidity and mortality that affects all older adults whether resident in institutions or in the community.7-10 It can lead to increased dependency, institutionalization, fear of falling, high economic cost, prolonged activity restriction and associated problems such as fear of falling with its negative impact on quality of life.11-13 Fear of falling (FOF) is a common consequence of falls and has been associated with limitation and/or reduction in the performance of activities of daily living, mobility, physical capability, mental health, balancing activities, quality of life, and also with increased institutionalization among older adults.14,15 Approximately half of those who fall develop fear of falling. 16 According to Cox and Williams, 17 fear of falling may occur in older adults, regardless of their history of falls. Over the years, FOF has been identified as a substantial health issue for older adults both physically as well as psychologically. 18
Previous studies have reported varying prevalence rates of falls among older adults: 60.3% in Egypt, 19 50.8% in United Arab Emirates, 13 34.7% in Ecuador, 20 27.8% in Nigeria, 14 27.6% in Brazil, 21 24.98% in India. 22 Recurring falls in the older adult population may result in serious health problems. Depression, fear of falling and other psychological problems are common consequences of recurrent falls. 23 Reports from recent Nigerian studies showed that there is a high prevalence of fear of falling among assisted-living and community-dwelling older adults respectively.15,24
Since falls pose a great concern for the older adults, the need to address it and provide an intervention becomes imperative. Exercise is considered an obvious preference as a fall prevention intervention.25,26 Over time, individually tailored fall prevention exercise programmes have become more common than general programmes. One example of an individually tailored exercise programme is the Otago Exercise Programme. 27
The Otago exercise program (OEP) is a well designed and tested falls prevention program that targets strength and balance deficits and can lead to a reduction in falls by about one-third. 28 This comprises 30 min of leg muscle strengthening and balance retraining exercises, progressing in difficulty, to be performed at home at least 3 times per week, and a walking plan for up to 30 min at a moderate pace to be undertaken at least 2 times per week. Otago exercise program has been shown to be effective in reducing fear of falling, falls and fall-related injuries. The Otago exercise program has been shown to be effective in improving balance, functional mobility, physical performance, functional capacity, lower limbs muscle strength, functional independence, health-related quality of life and reduced risk of falling in older adults.29-32 Otago exercise program reduced risk of falling, improved physical performance, functional capacity, and health-related quality of life in older adults receiving home care. Two previously published reviews,33,34 revealed the effectiveness of the OEP on the outcomes studied but none of the reviews included any article from Africa or low income populations. There has also not been any comprehensive review that studied the effect of OEP on both physical (falls, physical activity, physical function, balance, strength, mobility) and psychosocial (quality of life, depression, fear of falling) outcomes together either among community-dwelling or institutionalized older adults. Research interest on falls prevention intervention began in the 1970s in developed countries. The available studies were also among community-dwelling older adults with apparently few studies published in this area among institutionalized older adults, a group that has been reported to be more adversely affected by falls and fear of falling than their community-dwelling counterparts. 35 This study was therefore aimed at determining what is known about the effects of OEP on physical and psychosocial functions among community-dwelling and institutionalized older adults, in literature.
Methods
Search Strategy
According to Arksey and O’Malley, 36 scoping reviews “aim to map rapidly the key concepts underpinning a research area and the main sources and types of evidence available.” Arksey and O’Malley 36 developed a 5-stage framework for conducting a scoping review, expanded by Levac et al 37 which maintains a methodical course of transparency, in order to ensure reproduction of the search strategy and increasing the reliability of the study findings. 38 Consistent with this framework, we (1) identified the research questions, (2) identified the relevant studies, (3) selected the studies, (4) charted the data, and (5) collated, summarized, and reported the results obtained.
Step 1: Posing the initial research question
A considerable number of literatures that related to the outcomes of interest were extensively covered, through mapping the following initial research questions which guided the search: What is known from available literature about the effects of OEP on physical and psychosocial functions among community-dwelling and institutionalized older adults?
Step 2: Identifying the relevant research studies
For electronic searching, articles were identified by searching abstracts, titles and key words using appropriate MeSH terms or key words related to “Otago Exercise Program” (otago exercise), “older adults” (older, elderly, elder, senior), “effects” (impact, influence), “physical” (fall, balance, strength, physical activity, physical function, mobility), “psychosocial” (anxiety, depression, quality of life, fear of falling), “community” (community-dwelling), “institution” (long-term care, assisted living facility, nursing home, institutionalized). In order to broaden our search and ensure that we did not miss any relevant article, we did not restrict our searches to any publication date. The search was however, restricted to peer-reviewed English-language articles available online in order to avoid the cost of language translations. PEDro, PubMed, and Cochrane databases were used for the search. Furthermore, a manual search of the reference lists of identified articles was conducted and Google Scholar was searched to identify additional relevant articles within grey literature. The literature search was concluded in 6 months, ending in November 2020.
Step 3: Selecting the Studies
Using the title, abstract, keyword search, we identified 1069 articles (Cochrane = 352; PubMed = 574; PEDro = 143). Google Scholar yielded no additional relevant article. Six articles were also identified by a manual search of the reference lists of relevant studies. All the searches yielded a total of 1075 articles. Several articles were removed from the search as they were duplicated in all the databases. We manually removed 776 duplicates, resulting in 299 articles remaining. A critical re-evaluation of the available identified articles (titles and abstracts) revealed substantial numbers of articles that were not relevant. The relevance of papers without abstracts was ascertained from the title and key words. Full-texts of the remaining articles (number = 45) were obtained and further screened for eligibility. Keeping in mind the eligibility criteria, 14 articles considered relevant to this study topic were included. Figure 1 below is a PRISMA flowchart illustrating the process of selection of articles for this study.
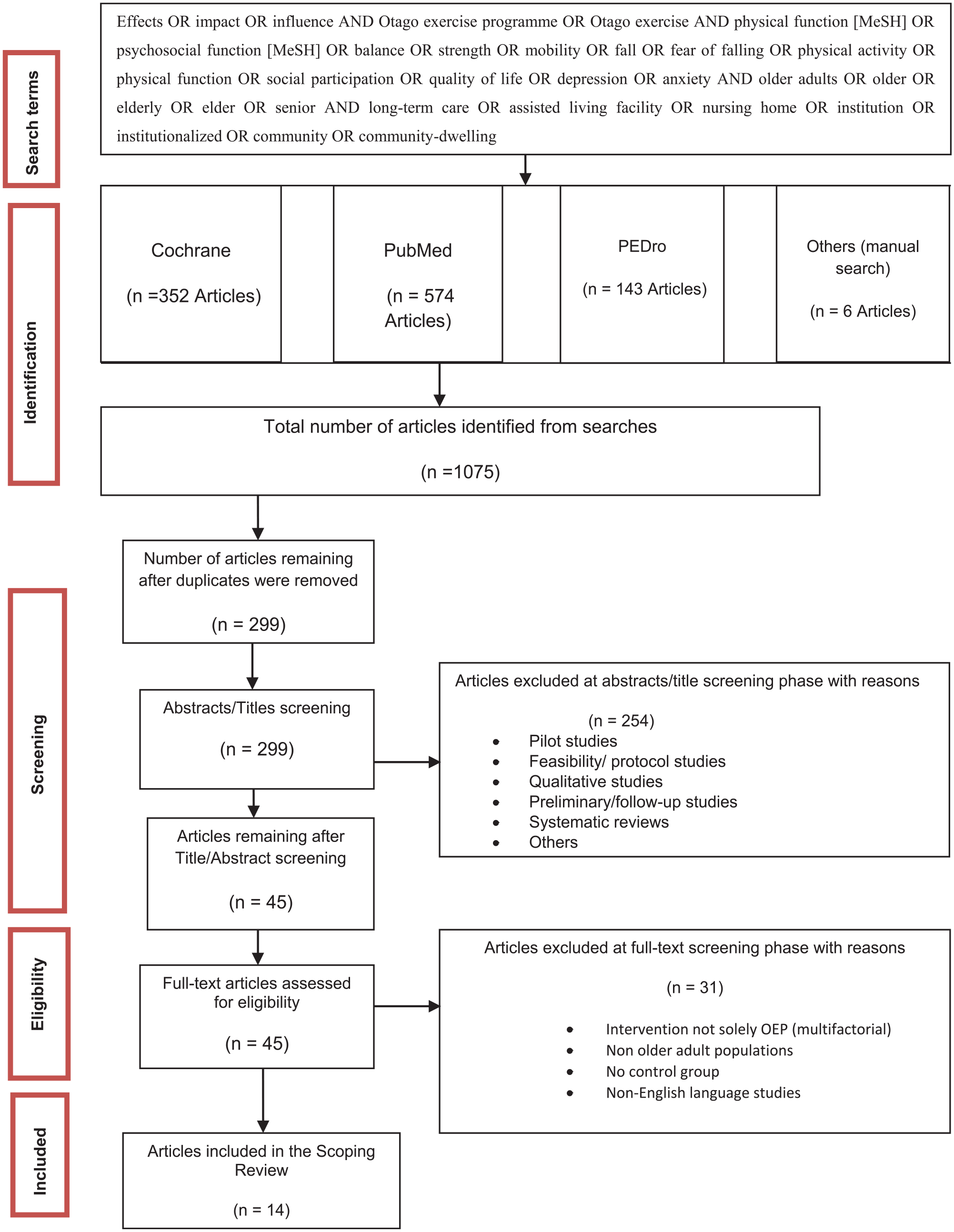
PRISMA diagram of the search strategy and study selection processes.
The following eligibility criteria were chosen in order to ensure that the selected articles studied only the variables under review.
Inclusion criteria: Original research articles; published in English language in a peer review journal; OEP was the central topic of the paper; the research was concerned with older adults. We also included studies where OEP was compared with no intervention or a placebo control intervention.
Exclusion criteria: We excluded articles that did not discuss OEP and/or older adults. Studies that included people who were not solely older adults were excluded.39-42We also excluded studies in which OEP was part of a multifactorial program or not solely the intervention such that participants received other interventions41,43-45; or studies in which OEP was in comparison with another exercise intervention. 46 We excluded feasibility/protocol/pilot studies; non-experimental studies; case report studies, follow-up studies. Two studies47,48 were 12- and 24-month follow-up studies of another randomized controlled trial, 49 and so were excluded while retaining the initial study. Systematic reviews; non-English language studies; duplicates, other scoping reviews, translational studies of implementation, dissertations, theses and conference papers were also excluded.
Restricting our searches to only English language and scientific articles is a limitation of our search, which may have diminished the scope of this review. However, the strength of this search is the fact that we did not restrict our searches to any publication year in order to ensure that we did not miss relevant article. We did not also restrict this review to studies that must have a comparison with a control group performing the original OEP (Table 1).
The Inclusion and Exclusion Criteria in a PICOS Format.

Step 4: Charting the data and collation
Summaries of each article were developed as it relates to the author, study location, year of publication, intervention type/study design, study population, sample size, aims of the study, overview of methods, outcome measures, and results (Table 2).
Meta-data of Included Studies.

Step 5: Collating, summarizing, and reporting the results
The final stage collates, summarizes and reports findings.
Results
The critical appraisal of included articles was utilized in this review to assess the methodological quality using the mixed methods appraisal tool (MMAT). 50 All the studies had low risk of bias. Seven studies utilized an appropriately performed randomization,29,31,49,51-54 while 2 of the studies did not perform an appropriate randomization.30,32 They simply mentioned “using simple randomization.” The remaining 5 studies did not employ randomization. Twelve studies had their participants’ characteristics comparable at baseline; Park and Chang 55 and Patel and Pachpute 23 had only one group and so could not make comparisons. Eleven studies had a complete data, while the remaining 3 had attrition rates exceeding the recommended accepted rate or had less than 70% of participants completing the study.51,54,56 Eight studies blinded the administrators to the intervention.29,31,32,49,51,53,54,57 The remaining 6 studies made no mention of the blinding process. There was clear representativeness of adherence to intervention protocol in 6 studies.23,29,31,49,51,58
Table 2 below summarizes the meta-data of all the included studies concerning study design, population, aims/objectives, methodology, outcome measures, results, strengths/limitations.
Location of the Studies
This scoping review yielded 14 articles that were published in 12 countries: Canada (2 studies), Norway (2 studies), Australia (1 study), India (1 study), Indonesia (1 study), Iran (1 study), Korea (1 study), Malaysia (1 study), Portugal (1 study), Serbia (1 study), Sweden (1 study), West Auckland (1 study). Approximately 71.4% of the reviewed articles were from Asia and Europe. There was a significant absence of literature from Africa.
Study Design
The study designs utilized by the 14 reviewed articles were: randomized controlled trials (8 studies), pre and post- test design (3 studies), clinical trials (1 study), quasi-experimental study- pre- and post- test design using a control group (1 study) and non-randomized experimental study using a control group (1 study).
Population
Participants were aged 65 years and above. The mean age of the total participants was 79.38 ± 5.85 years. While one trial recruited females only, 57 the remaining 13 studies recruited a total of 1643 older adults with about 69.6% female (2 studies did not specify the percentage of gender), with a sample size range of 8 to 344. Majority of the trials included ambulant participants (with or without aid), who were not receiving any other form of physiotherapy. Participants needed to be able to walk independently with or without support at least 3 m, because the OEP has a walking component. Only 2 studies recruited only individuals who lived in an institutional setting.30,31 One study assessed the effect of OEP on specific conditions. 55
Types of Outcome Measures
Outcomes of interest were physical and psychosocial functions which include: Health-related Quality of life, measurements of physical performance, fall self-efficacy, activity level, handgrip strength, adherence to the exercise, functional independence, gait, strength, rate of falls, fall risk, balance, and functional mobility. Majority (60%) of the articles reviewed aimed at determining balance (71.4%), lower extremity strength (57.1%), and mobility (71.4%). All the studies that assessed mobility utilized Timed-Up-and Go test, while 50% of the studies that assessed balance utilized the Berg Balance Scale (BBS).
Duration of Intervention
The duration of intervention in the articles reviewed was 6 weeks to 12 months: 6 weeks (n = 2); 8 weeks (n = 2); 12 weeks (n = 5); 6 months (n = 4); 12 months (n = 1).
Aims
The studies reviewed explored the effectiveness of the OEP on outcome measures such as balance, strength, gait, functional mobility, health-related quality of life, falls efficacy, falls, fear of falling, etc. among older adults. A study estimated the cost-effectiveness of the OEP from a healthcare system perspective. 59
Methodology/Intervention Adopted
The interventions adopted by the studies included in this review were OEP in its original and modified forms. Previous reviews used the OEP either in its original form only 33 or modified form only. 34
Main Findings of Most of the Included Studies
Most of the included studies reported that: (1) The OEP is significantly effective in increasing strength of lower limb and improving in balance, physical performance measures, functional mobility, gait, reduced the rate of subsequent falls and functional independence, indicating that it could help in slowing of disability progression. (2) The OEP improves functional abilities, social participation, and self-efficacy, reducing the risk of falling and enhancing health. (3) The OEP improved functional capacity as well as the score for activities of daily living and quality of life. (4) The OEP also prevents deterioration in upper limb strength and improves grip strength. (5) OEP performed as group training is more effective for improving functional balance, muscle strength and physical health, but not fall efficacy and mental health than when performed as home training. (6) The OEP improved fall efficacy but some studies found no effect on falls self-efficacy. (7) Majority (12) of the 14 reviewed studies were conducted in the community, while only 2 were conducted in an institution. (8) Only 2 of the reviewed studies were performed in groups; one in each of community and institution.
Table 3 below illustrates the themes from the findings of the reviewed studies
Summary of the Result-Themes and Number of Studies.

Otago exercise program and falls
Falls and fall-related injuries are a leading cause of morbidity and mortality among older adults. The OEP is the most widespread fall prevention program, 34 and has been proven to reduce falls by 35%. 28
Dadgari et al 52 reported that in the experimental group, the mean of fall incidence declined from 1.58 to 1.26 from pre to post intervention assessment, showing that the Otago exercise program significantly reduced the incidence of falls.
Findings from Kiik et al 30 showed that the Otago training significantly reduced the risk of falling among the studied older adults (P = .041). The risk of falls in the intervention group decreased from 14.26 to 12.05 s and increased from 12.94 to 13.26 s in the control group.
Otago exercise program and fear of falling
Self efficacy is the self-belief or capability to create a plan and implement it. 46 In studies by Bjerk et al 29 and Kyrdalen et al, 51 fear of falling was assessed by Falls Efficacy Scale International (FES-I) which measures fear when performing 16 daily activities. The participants had a mean FES-I score of 30.7. These studies found no effect on falls self-efficacy. This may be due to the shorter duration of the intervention being an insufficient period of time to make any observable psychological changes. However, Park and Chang 55 revealed that the OEP improved fall efficacy of stroke patients significantly.
Otago exercise program and quality of life
Falls and fall-related injuries have consequent impacts on the quality of life of both fallers and their families. Health-related quality of life in several studies was measured using the Short-Form 36 Health Survey (SF-36). The SF-36 summary score is comprised of a physical component summary and a mental component summary. The scores range from 0 to 100. Bjerk et al 29 and Kyrdalen et al 51 reported that the OEP improved physical health-related quality of life in all physical subscales of SF-36 in the intervention group compared with the control group. However, there was a significant decline in the mental health subscale of SF-36. OEP seems effective in improving physical health; but, may not significantly increase the mental health status. Recent study by Kiik et al 30 among older adults with chronic disease however revealed that the mental health status scores in the intervention group increased from 43.24 to 49.42 (P = .002), whereas the physical health status showed no significant increase (P = .556). Park and Chang 55 utilized the EQ-5D to measure quality of life, and their result showed that the OEP improved quality of life though not significantly. It seems therefore that the presence of chronic diseases or use of varying instruments may determine how quality of life was rated by older adults on OEP.
Otago exercise program and balance
The OEP is a falls prevention program which addresses the risk factors of poor balance and lower limb weakness with an individually prescribed, home-based strength and balance exercise program. 27 The BBS was utilized by a greater number of studies to measure balance. The berg balance scale evaluates 14 tasks that are related to stability in sitting, standing, turning around, walking on an even surface, walking on steps and balance while changing body position. It has been found to be excellent, internally consistent and to have a high degree relative inter-rater reliability in a population of nursing home residents. 60
- Bjerk et al 29 : Per-protocol analyses showed significant improvements in BBS scores in the intervention group compared with the control group.
- Liew et al 32 : Significant improvements were observed in balance in the OEP group. BBS score increased from 48.0 (7.0) at baseline to 49.6 (6.4) at 3 months to 51.5 (5.1) at 6 months
- Kocic et al 31 : The BBS scores increased from 42.7 ± 8.4 (45.0) at baseline, to 47.0 ± 6.7 (48.0) at 3 months to 48.0 ± 6.6 (49.0) at 6 months
- Dadgari et al 52 : BBS results present significant differences between control and experimental groups when comparing the post-intervention results (x 2 = 21.31, df = 2, P-value = .025).
- Kyrdalen et al 51 : Following the intervention, BBS improved significantly more for the group training group than for the home training group (P = .014). The OEP performed as group training is more effective for improving functional balance than when performed as home training.
- Patel and Pachpute 23 measured balance using Tinetti Performance Oriented Mobility Assessment, and reported a significant difference pre- and post- intervention with mean and standard deviation of 20.42 ± 3.28 versus 21.54 ± 3.44 (P-value = .000).
Otago exercise program and strength
For muscle strength assessment, the sit-to-stand test was used in most of the studies. This involves a standard chair with no arms and a seat height of approximately 43 cm. The participants were asked to fold their arms across their chest and to stand up and from the chair. If successful, participants were asked to stand up and sit down 5 times as quickly as possible. They were timed from the initial sitting position to the final standing position at the end of the fifth stand.
- Bjerk et al 29 : Per-protocol analyses showed significant improvements in the sit-to-stand scores in the intervention group compared with the control group.
- Kyrdalen et al 51 : the OEP performed as group training is more effective for improving muscle strength than when performed as home training.
- Kocic et al 31 : the lower limb strength improved from 12.0 ± 2.6 (12.0) at baseline, to 10.7 ± 2.5 (11.0) at 3 months, to 9.5 ± 2.1 (10.0) at 6 months (P < .001). The OEP was shown as effective in improving lower limbs muscle strength indicating that it could help in slowing of disability progression.
- Liew et al 32 : Significant improvements were observed in grip strength in the OEP group. The OEP also prevents deterioration in upper limb strength. Left-hand grip strength increased from 14.0 (7.9) at baseline to 14.7 (6.5) at 3 months, to 13.7 (6.9) at 6 months. Right-hand grip strength improved from 15.8 (6.9) at baseline, to 17.0 (7.0) at 3 months, to 15.8 (6.9) at 6 months. Five Times Sit to Stand test scored 17.4 (10.6) at baseline, 16.4 (9.8) at 3 months, and 15.0 (11.8) at 6 months.
- Patel and Pachpute 23 : the Chair Stand Test shows pre and post intervention significant difference in mean and standard deviation of 1.133 ± 0.345 versus 1.346 ± 0.485 (P-value = .01).
Otago exercise program in institutions
The OEP has been shown to be an effective strategy in prevention of functional decline of community-dwelling older people, while there is dearth of evidence to ascertain which exercise program is most appropriate for institutionalized older adults. 61
- Kocic et al 31 : Significant improvement has been observed in the 30 s sit to stand test, BBS, timed up and go test. This could suggest that the OEP might be effective in improving balance, functional mobility, lower limbs muscle strength as well as level of functional independence in nursing home residents older than 65 years.
- Kiik et al 30 : OEP significantly improves the health status and reduces the risk of falling among older adults with chronic illness (P = .041). The risk of falls after the OEP intervention group decreased from 14.26 to 12.05 s. OEP improved the health status (P = .011) from 42.40 into 47.10, with the mental health status scores increasing from 43.24 to 49.42 (P = .002), though the physical health status showed no significant increase (P = .556). The exercise can be recommended for older adults with chronic illness in social elderly institutions and communities.
Otago exercise program in the community
Substantial evidence on falls prevention among community dwelling older adults abounds. 62 The OEP has been shown to be an effective strategy in prevention of functional decline of community-dwelling older adults. Majority (85.7%) of the reviewed studies were conducted in the community.
Otago exercise program in group
OEP has been reported to be effective in community dwelling older adults, but in only few studies it was assessed as group-based OEP.31,51
- Kyrdalen et al 51 : The OEP performed as group training is more effective for improving functional balance, muscle strength and physical health, but not fall efficacy and mental health than when performed as home training. The results were significantly better for both Berg Balance Scale and timed up and go test in group-based than in home-based OEP.
- Kocic et al 31 : Significant improvement has been observed in the 30 s sit to stand test, Berg Balance Scale, timed up and go test. This could suggest that the OEP might be effective in improving balance, functional mobility, lower limbs muscle strength as well as level of functional independence in nursing home residents older than 65 years.
Otago exercise program and functional mobility
Majority of the included studies utilized the time-up-and-go-test to measure functional mobility. The timed up and go test involves rising from a chair, walking 3 m, turning around, walking back to the chair and sitting down. The participants are instructed to complete the task at their usual pace. The time is taken when the participants rise from an armchair until they sit down again. The participants are allowed to use their usual walking aids. Each participant is given 3 trials and the average result of 3 trials was used. Scores ≥12 indicate high risk of falls, whereas scores <12 denote a low risk of falling. 63 Longer completion times are associated with impaired mobility and fall risk; completion times of 13.5 sor longer indicate high fall risk. 54
- Kocic et al 31 : The OEP was shown as effective in improving functional mobility indicating that it could help in slowing of disability progression. The timed up and go test improved from 18.9 ± 6.9 (17.1) at baseline, to 17.2 ± 7.1 (15.4) at 3 months, to 16.2 ± 7.5 (13.9) at 6 months (P < .001).
- Liew et al 32 : Timed Up and Go test improved from 16.5 (12.2) at baseline, to 14.8 (7.5) at 3 months, to 14.1 (8.7) at 6 months
- Liu-Ambrose et al 53 : Timed Up and Go Test improved from 14.2 ± 4.6 at baseline, to 13.6 ± 4.3 at 6 months.
- Dadgari et al 52 : The timed up and go test results present significant differences between control and experimental groups when comparing the post-intervention results of timed up and go test (x 2 = 36.99, df = 2, P-value = .017).
Modified Otago exercise program
Otago exercise program has been utilized in various modified formats such as exclusion of the walking component of the original Otago exercises, 32 exercise in group, kyrdalen, kocic31,51 a “modified” Otago incorporated in a technological system using pressure and inertial sensors, feedback, and Exergames. 58 In a systematic review conducted by Martins et al, 34 all researches utilizing OEP modified formats revealed improvements on balance and functional ability.
Discussion
Scoping review was chosen in this study because our objective was to identify the important physical and psychosocial outcomes existing in literature as it relates to the Otago exercise program among community-dwelling and institutionalized older adults, which is evidently what scoping reviews were mapped out to do. 36
The significant absence of literature from Africa is an issue that warrants attention. According to the World Health Organization, 70% of the aging population live in developing countries where prevalence and incidence of fall are increasing at an alarming rate and injury due to fall is considered as inevitable and high in number. In Africa, a population-based survey from Tanzania revealed that falls accounted for about 35% of reported injuries among older adults. 64
Our review shows the OEP as an effective exercise prevention intervention among specific older adult population—female-only participants 57 and condition—stroke. 55 Previous studies reported that females were associated with a greater prevalence of falls.20,21 Bekibele and Gureje 65 had opined that a fall intervention program must have a particular focus on females and those with chronic pain conditions.
Furthermore, this review revealed that only 2 articles studied institutionalized older adults,30,31 highlighting the limited body of research on this topic, thus suggesting that this population has not been prioritized for research. This calls for serious attention as it has been reported that older adults living in institutions have higher fall prevalence. Evidence reveals that falls are 3 times more frequent in institutionalized older adults than in community-dwellers. 66 Declines in physical functions associated with age are more prevalent among institutionalized older adults than in community-dwelling older people. 67 However, the reason for more emphasis on community-dwelling older adults than their institution resident counterparts could be because of its cost-effectiveness, as also revealed in recent studies. 68 Another reason could be the feasibility of such studies in institutions.
Studies show that exercise can improve balance and reduce fall rates among older adults. 69 This review corroborates these findings as majority of the included studies reported a significant improvement on all the functional outcomes among older adults; improving physical and psychosocial functioning.30,31,51-53,55,57,70-72 However, contradictory results exist on whether the OEP is more effective in improving physical or mental health. While Bjerk et al 29 and Kyrdalen et al 51 reported that the OEP improved physical health-related quality of life in all physical subscales of SF-36 with a significant decline in the mental health subscale; Kiik et al 30 revealed improvement in the mental health status scores in the intervention group with no significant increase in the physical health status. Park and Chang 55 utilized the EQ-5D to measure quality of life, and their result showed that the OEP improved quality of life though not significantly. It seems therefore that the presence of chronic diseases or use of varying instruments may determine how quality of life was rated by older adults on OEP. The Short Form 36 Health Survey (SF-36) is a widely used generic health status questionnaire consisting of 8 domains (physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health), which measures the quality of life of a population. Higher scores in the domains indicated lower levels of limitation while lower scores indicated high levels of limitation. The EuroQol-5 Dimension (EQ-5D) is a well-established generic tool used for measuring health-related quality of life, consisting of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, anxiety/depression). These 2 instruments are generic. However, there are validated tools with acceptable psychometric properties, specific to older adults, for measuring quality of life among this population, such as the Older People’s Quality of Life Questionnaire (OPQOL-35)73-75
Conflicting results exist from previous studies on whether group training is more effective than individual training among older adults at higher risk of falling.76,77 Findings from this review however reveal that group-based Otago exercise program is more effective. This review found that OEP can be successfully and effectively implemented in groups and in institutions, even though there are just very few studies. Only one article studied the effectiveness of the OEP performed in groups among institutionalized older adults. 31 This buttresses the findings in gerontological literature, that the effects of the OEP performed in groups on falls and fall risks among older adults resident in institutions are sparsely researched. 78 Performing the OEP in groups is beneficial to the older adults in both settings as it encourages adherence to the program, cost-effectiveness, and enhances social support/participation/networks. Older adults tend to be more secluded, and engaging in group activities can promote social activities and independence. 79 Leijon et al 80 had opined that group training motivates participants to perform exercise more effectively and has better adherence rates than individual training. Findings from this review could suggest that the OEP might be effective in improving balance, functional mobility and independence, lower limbs muscle strength, quality of life among older adults. It is therefore important for policy makers and governments to see older adults as a resource in order to help shape decisions concerning them; formulating aging policies especially fall intervention policies.
The theoretical and clinical implications of this study is that health care professionals and researchers would have available to them information on variables that have been explored using the Otago Exercise Program. This would further influence their treatment and rehabilitation plans as it regards older adults while ensuring healthy/active aging.
Gaps in the Research/Key Points
This review found no single study of the OEP from Africa. Further studies on the comparative effects of the OEP on physical and psychosocial functions among community and institution older adult residents are needed. Future studies should compare the effects of the OEP between community and institution older adult residents; and between the OEP applied in groups and individualized.
Most studies had their intervention on a shorter duration than the original OEP protocol. Only one study administered the OEP in its original form duration of 12 months. 54 Only 2 studies in this review investigated the effects of the OEP among institutionalized older adult residents.30,31 Some studies also excluded the walking component of the OEP. 32
The studies reviewed explored a good number of the physical and psychosocial function outcomes. From our findings, it is evident that there is no single study on the effects of OEP on depression among older adults, either in the community or in institutions. However, only 2 studies reviewed assessed depression, but only at baseline.52,54 They failed to report the difference in the pre- and post-intervention results/effects. Adherence to the intervention was not assessed in most of the studies. Evidence from literature shows that adherence and success of an exercise strategy mainly depends on the program characteristics and personal factors.
Limitations
The quality of this survey may have been affected by non-inclusion of studies not published in the English language. There was difficulty getting articles that discussed all the outcome measures, and only a few numbers of studies were included, hence making it difficult to discuss the findings and draw definite conclusions adequately. The older adult sampled in the various studies were quite heterogeneous and may limit the generalizability of the results. However, this study is the first scoping review, to the best of the researchers’ knowledge, performed on the effects of the OEP on physical and psychosocial functions among community and institutionalized older adults. Also, the strength of this review lies in the identification of knowledge gap on the effects of the OEP on physical and psychosocial functions among community and institutionalized older adults through an in-depth literature search and the review of the included studies which had a low risk of bias. Future reviews should widen the eligibility criteria to allow for more inclusion of studies. Further larger clinical studies are needed to evaluate the effectiveness of the group-based OEP among older adults especially in institutions. Adherence issues were also observed in some of the studies; it is possible that greater influence on health outcomes could be achieved if the intervention protocol was adhered to. Future studies should also evaluate the effect of the OEP on depression, pre- and post- intervention, especially from the African context, as no single OEP study was found from Africa. Previous studies in Nigeria, Africa’s most populous nation, have reported a high prevalence rate of depression among older adults, 81 and also provided a validated culture-specific tool for measuring depression. 82
Conclusions
The findings from this review support the premise that OEP is an effective fall prevention intervention/strategy. The Otago exercise program performed as group program is more effective in improving lower limb muscle strength, functional balance and mobility than when performed individually. However, the mode of the program should be decided with consideration of the primary aims of the training and the individual’s preferences. This study provides a basis for future research by highlighting the possibilities of different modes of the OEP in improving physical and psychosocial functions among older adults. Further studies should be done to explore the comparative effects of group and individualized OEP in the community and institution on physical and psychosocial functions among older adults. Future and prospective reviews, especially, systematic reviews and meta-analysis should be performed on the variables studied, especially depression.
Footnotes
Acknowledgements
None.
Author Contributions
Ukamaka Gloria Mgbeojedo: conceived and designed the study, screened abstracts for relevancy, determined eligibility and extracted data, involved in the manuscript writing, reviewed the final version of the manuscript. Christopher Olusanjo Akosile: designed the study, involved in the manuscript writing, reviewed the final version of the manuscript. Emmanuel Chiebuka Okoye: screened abstracts for relevancy, involved in the manuscript writing. Kenneth Umezulike Ani: screened abstracts for relevancy, reviewed the final version of the manuscript. Echezona Nelson Ekechukwu: determined eligibility, reviewed the final version of the manuscript. Obinna Chinedu Okezue: determined eligibility, involved in the manuscript writing: Jeneviv Nene John: extracted data, involved in the manuscript writing. Nwobodo Nnaemeka: determined eligibility, reviewed the final version of the manuscript. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declarations
Our study did not require Ethical board approval and informed consent because it was a review of previous studies. It did not involve any human participants directly.