
Abstract
The COVID-19 pandemic has transformed undergraduate education into non-face-to-face classes, and a novel methodology is required to aid students in career preparation behavior (CPB). This study aimed to assess the effects of self-rated abilities for health practices (SRAHP) as a psychological attribute and health-promoting lifestyle profile (HPLP) as a behavioral attribute in the dynamics between positive psychological capital (PPC) and CPB among undergraduate students taking non-face-to-face classes. A cross-sectional study was conducted involving 639 undergraduate students taking non-face-to-face classes; data were obtained via online survey in January 2022. A significant positive effect on CPB was observed for PPC (b = 0.261, p < .001) and HPLP (b = 0.674, p < .001). The effect of SRAHP on CPB was not significant; however, it mitigated the PPC–CPB dynamics (b = −.081, p < .05) and strengthened the relationship between HPLP and CPB (b = .250, p < .001). Lastly, the mediating effects after moderation for HPLP and SRAHP were positive, with statistical significance. To aid the students with career preparation in the current undergraduate education environment moving toward a non-face-to-face model, there is a need for resources to increase students’ psychological confidence regarding health management and to promote their health practices.
What do we already know about this topic?
Positive psychological capital among college students affects their career preparation.
How does your research contribute to the field?
Regarding health management, the psychological attributes of health management, self-rated abilities for health practices, and the moderated mediating effect of health promotion behaviors confirmed the need for health management among college students undergoing enhanced online education.
What are your research’s implications regarding theory, practice, or policy?
Systematic health management must be provided by establishing public governance for graduate students taking non-face-to-face classes.
Introduction
The fourth Industrial Revolution predicted the impending online era, which has become a reality in daily life, particularly since the COVID-19 pandemic. Notably, the education paradigm has shifted toward an online model, engendering various changes. 1 As part of the social distancing that began in 2020 due to the COVID-19 pandemic, students were prohibited from attending schools, and classes were transformed from in-person to remote or online formats. 2 The sudden change in educational formats had to be accepted without any preparation, and many schools complained of problems related to lack of equipment and difficulty in class preparation. 3
There were also problems with unrefined systems and the gap in the level of education among students because of classes being conducted online.4-6
Nevertheless, with the prolongation of the pandemic, stronger emphasis was placed on online classes, and problems were resolved at a rapid pace to create a ubiquitous environment based on the efficient Learning Management System (LMS). During this period, lecturers, professors, and students adapted to the new online learning environment and began appreciating the educational outcomes. 7 Moreover, the accumulation of digital learning data as a result of increased online classes has enabled the rapid development of algorithms for performance predictions,8,9 and hybrid education models utilizing online platforms have been recommended.10,11 Hence, online education is a promising way of learning in the future. 12 Even after the pandemic ends, the number of students wanting to leave online classes and go back to “in-person” classes as the official format of education is predicted to be low. 13
Students reported the benefits of online classes in enabling them to use time more efficiently and increasing their independence, as education now transcends spatiotemporal limitations. 14 However, problems have emerged related to reduced physical activities, 15 reduced opportunities to form social relationships, and associated psychological health issues, such as depression and anxiety. 16 As the COVID-19 pandemic persists, the undergraduate education field is striving to advance teaching and learning methods in online formats. However, their support for health management remains fractional and biased toward relieving negative emotions such as anxiety and stress to improve psychological health. 17 Thus, more focus should be placed on the overall health management of undergraduate students. To identify the level of health-promoting lifestyles of undergraduate students, the most universally used indicator is behavioral evaluation, and evaluative processes on current lifestyles should also be included. 18 The concept used in such cases involves the “health promotion lifestyle profile.” It consists of a vast range of lifestyle components, including health responsibility, spiritual growth, physical activity, interpersonal relationships, nutrition, and stress management. 19 These components must be assessed for university students whose learning styles and lifestyle methods rapidly change. However, Becker et al 20 stated that among the variables that predict health-promoting behaviors, self-rated abilities for health practices (SRAHP) must be included, as they indicate one’s belief in implementing health management. Although SRAHP is a powerful variable to predict health-promoting behaviors, it can vary depending on the obstacles faced during the process leading to these behaviors. 21 Therefore, active research on the roles of health management-related psychological and behavioral attributes is required for undergraduate students in the pandemic situation.
Meanwhile, undergraduate students in their early or mid-20s spend much time searching, verifying, and preparing for future careers. Thus, universities provide diverse educational services to maximize students’ educational outcomes and satisfaction. 22 Kotler and Karen 23 defined the area of future design, including support for employment and career, as a category of undergraduate educational services. Numerous universities offer career preparation programs, including special lectures, coaching, and counseling sessions to help with career design.17,24 In the current situation, in which the COVID-19 pandemic prevents face-to-face activities, career uncertainty is one of the factors causing the highest stress in undergraduate students. 25 Park and Jeon 26 reported that this results from reduced confidence because of a lack of preparation. It is therefore necessary to identify the level of career preparation behavior (CPB) in undergraduate students taking online classes, and seek ways to improve their CPB.
Various studies have investigated the factors that reinforce CPB. The level of positive psychological capital (PPC), a positive state of mind that can be developed by an individual, 27 was shown to have a powerful influence on CPB.28,29 Therefore, universities have provided various programs, including psychological support, for students.30,31
A close association has been found between PPC as a psychological attribute and the factors related to health.32,33 However, there is limited research on the role of health-related factors in PPC and CPB among undergraduate students who mainly engage in online learning in daily life. Thus, this study aimed to determine the effects of (SRAHP) as a psychological attribute and the health-promoting lifestyle profile (HPLP) as a behavioral attribute in the dynamics between PPC and CPB. This study provides primary data to support the need for health management in undergraduate education (Figure 1).
The key questions are as follows:
(1) How do SRAHP and HPLP affect the relationship between PPC and CBP?
(2) Do SRAHP and HPLP show mediating effects after moderation in the dynamics between PPC and CPB?

The research model.
Materials and Methods
This cross-sectional study aimed to determine the effects of SRAHP and HPLP on the dynamics of PPC and CPB among undergraduate students taking online classes.
Sample and Data
Participants were undergraduate students aged 19 to 29 years, taking online classes at the university. We used Google Survey to create a link to the advertisement to recruit participants. There were also links to the consent forms and the survey. These were posted in an online student community (NAVER) to collect anonymous data from January 7 to 9, 2022. There were 658 students who responded to the recruitment advertisement. After excluding those with no experience of online classes and those with insincere responses, the final group comprised 639 participants; the response rate was 97.1%. According to Bentler and Chou, 34 a sample size approximately 5 to 10 times greater than the free parameters is required to allow stable structural model estimations, indicating the need for 580–1 160 samples, based on 116 free parameters (the number of survey questions). Hence, the final number of participants in this study was adequate.
This study was approved by the Institutional Review Board of the institution where the study was conducted (IRB No. JJIRB-211215-HR-2021-1214). The online questionnaire contained information regarding the study purpose, procedures, and content related to drop-out, while the participants submitted their consent as part of the online questionnaire. All data were collected anonymously and then coded for statistical analyses to ensure privacy protection.
Measures of Variables
Positive psychological capital (PPC)
PPC was measured using a tool developed by Luthans et al 35 and translated and revised to suit undergraduate students by Kim. 36 The tool consists of 24 questions regarding self-efficacy, hope, resilience, and optimism on a self-reported 6-point Likert scale (1 = Strongly disagree to 6 = Strongly agree). The Cronbach’s ⍺ was .94 at the time of development and .92 in this study (Table 2).
Self-rated abilities for health practices (SRAHP)
SRAHP was measured using a tool developed by Becker et al, 20 translated and tested for validity in undergraduate students by Lee et al. 37 The tool consists of 24 questions regarding the management of exercise, disease, emotion, nutrition, stress, and health, on a self-reported 5-point Likert scale (0 = Strongly disagree to 4 = Strongly agree). The Cronbach’s ⍺ was .94 at the time of development and .91 in this study (Table 2).
Health-promoting lifestyle profile (HPLP)
HPLP was measured using the Health-Promoting Lifestyle II [HPLP II], a tool developed by Walker et al, 19 and translated and revised by Seo and Hah, 38 who excluded 2 duplicated questions. The tool consists of 50 questions regarding physical activity, health responsibility, nutrition, spiritual growth, stress management, and social relationships, answered on a self-reported 4-point Likert scale (1 = Strongly disagree to 4 = Strongly agree). The Cronbach’s ⍺ was .94 at the time of development and .95 in this study (Table 2).
Career preparation behavior (CPB)
CPB was measured using a tool developed by Kim and Kim 39 to measure the CPB among undergraduate students, revised by Lee 36 to include 2 additional questions, considering recent online career-related information and increased career counseling institutes. The tool consists of 18 questions regarding information search, instrument acquisition, and practical efforts, answered on a self-reported 5-point Likert scale (1 = Strongly disagree to 5 = Strongly agree). The Cronbach’s ⍺ was .88 in Lee’s 40 and .92 in this study, indicating good reliability (Table 2).
Models and Data Analysis Procedure
We used SPSS 26.0 to analyze the general characteristics through frequency analysis, description statistics, independent t-test, and 1-way ANOVA. We used Model 15 of the SPSS PROCESS MACRO to analyze the mediating effects after moderation. As the SPSS PROCESS MACRO relies on limited information estimation, the required sample size was not large, even for the mediation models after complex moderation. Notably, the Johnson–Neyman method can be used in analyzing the moderating effects. This method does not merely check the significance of moderating effects or the parallel estimation lines on the graph according to moderation variables, it also predicts the areas of significant moderating effects according to the moderation variables. These are measured as continuous variables and the sample ratios are calculated to provide specific data for result interpretation regarding moderating effects.41,42 To analyze the mediating effects after moderation, we set the independent, dependent, mediation, and moderation variables as PPC, CPB, HPLP, and SRAHP, respectively. To analyze the moderating effects, we performed mean-centering, as it reduces the probability of multicollinearity and allows convenient interpretation of regression coefficients. Finally, a bias-corrected bootstrap was performed to verify the significance of mediating effects and mediating effects after moderation at a 95% confidence interval.
Results
General Characteristics of Participants
The analysis of the participants’ general characteristics showed that 585 (91.55%) participants were <25 years, and 54 (8.45%) were ≥25 years. Participants’ age was classified into <25 years and ≥25 years, as this is the age range for completing a general 4-year formal education program without discontinuation. There were 285 (44.60%) men and 354 (55.40%) women. In terms of their majors, 111 (17.37%) were in public health care, 26 (4.07%) in arts, 246 (38.50%) in humanities, social studies, and education, and 256 (40.06%) in science and engineering. The students in Years 1, 2, 3, and 4 were 58 (9.08%), 236 (36.93%), 199 (31.14%), and 146 (22.85%), respectively. As for how long students had online classes, 319 (49.92%) stated 1 or 2 semesters, 299 (46.79%) 3 to 4 semesters, and 21 (3.29%) 5 or more semesters. The online classes were viewed as ineffective by 237 (37.09%) students and as effective by 402 (62.91%) students. The main format of online classes was video lectures for 180 (28.17%), real-time online lectures for 418 (65.41%), mixed lectures for 21 (3.29%), and LMS-based activities for 20 (3.13%) students. Most students preferred video lectures (309 [48.36%]), followed by face-to-face lectures (187 [29.26%]) and real-time online lectures (143 [22.38%]) (Table 1).
PPC, SRAHP, HPLP, CPB According to General Characteristics (N = 639).

Post hoc = Duncan; PPC = positive psychological capital; SRAHP = self-rated abilities for health practices—health self-efficacy; HPLP = health-promoting lifestyle profile; CPB = career preparation behavior a,b,c,d are categories for post hoc analysis.
PPC, SRAHP, HPLP, and CPB According to General Characteristics
Table 1 presents the general characteristics of participants and the results of analyzing the variations in PPC, SRAHP, HPLP, and CPB as per the characteristics. PPC varied significantly according to gender (t = −5.16, p < .001), major (F = 9.45, p < .001), year (F = 6.90, p < .001), duration of online classes (F = 6.34, p < .001), effect of online classes (t = 2.97, p < .001), form of online classes (F = 12.88, p < .001), and preferred form of lecture (F = 23.37, p < .001). SRAHP varied significantly according to gender (t = −4.27, p < .001), major (F = 6.64, p < .001), year (F = 8.87, p < .001), duration of online classes (F = 3.69, p = .03), form of online classes (F = 11.83, p < .001), and preferred form of lecture (F = 18.10, p < .001). HPLP varied significantly according to gender (t = −2.16, p = .03), year (F = 14.17, p < .001), form of online classes (F = 9.04, p < .001), and preferred form of lecture (F = 6.54, p < .001). Lastly, CPB varied significantly according to gender (t = −2.35, p = .02), major (F = 3.96, p = .01), year (F = 9.92, p < .001), form of online classes (F = 7.79, p < .001), and preferred form of lecture (F = 8.19, p < .001).
Descriptive Statistics and Correlation Analysis
Table 2 presents the study variables’ descriptive statistics and correlation analysis results. All correlations were positively significant (r = .675–.734) at the .001 level. The normality was satisfied, as the absolute skewness and kurtosis were less than 2 and 7, respectively. 43
Description Statistics and Correlation Analysis (N = 639).

Note. The numbers in parentheses indicate the reliability (Cronbach’s alpha).
PPC = positive psychological capital; SRAHP = self-rated abilities for health practices—health self-efficacy; HPLP = health-promoting lifestyle profile; CPB = career preparation behavior.
p < .001.
Mediating Effects After Moderation
Table 3 presents the results of analyzing the mediating effects after moderation for HPLP and SRAHP in the dynamics between PPC and CPB among undergraduate students (R 2 = .612, F = 199.69, p < .001). A significant positive effect on CPB was observed for PPC (b = 0.261, p < .001) and HPLP (b = 0.674, p < .001). The effect of SRAHP on CPB was not significant; however, it mitigated the PPC–CPB dynamics (b = −.081, p < .05) and strengthened the relationship between HPLP and CPB (b = .250, p < .001). On the one hand, the higher the PPC, the higher the CPB, and the increase was greater when SRAHP was relatively low. On the other hand, the higher the HPLP, the higher the CPB, and the increase was greater when the SRAHP was relatively high. Lastly, the mediating effects after moderation for HPLP and SRAHP were positive, with statistical significance.
Mediating Effects, Moderating Effects, and Mediating Effects After Moderation (N = 639).

IV = PPC; Med = HPLP; Mod = SRAHP; ModMed = mediating effects after moderation of HPLP and SRAHP, Bootstrap sample size = 5000. CI = confidence interval; LL = low limit; UL = upper limit.
p < .05. ***p < .001.
Figure 2 shows the graph visualizing the moderating effects of SRAHP. The group with low SRAHP showed a greater increase in CPB, with an increase in PPC, compared to the group with high SRAHP. After applying the Johnson–Neyman technique to determine the significant region of the moderating effect, the moderating effects of SRAHP were significantly positive in the range of −2.185 to 1.298, to which approximately 97% of the entire sample corresponded. In addition, compared to the group with low SRAHP, the group with high SRAHP showed a greater increase in CPB with an increase in HPLP. After applying the Johnson–Neyman technique, the moderating effects of SRAHP were significantly positive, in the range of −1.635 to 1.481, to which approximately 99% of the entire sample corresponded. The Johnson–Neyman technique results suggested that the moderating effect of SRAHP was significantly universal in most samples.
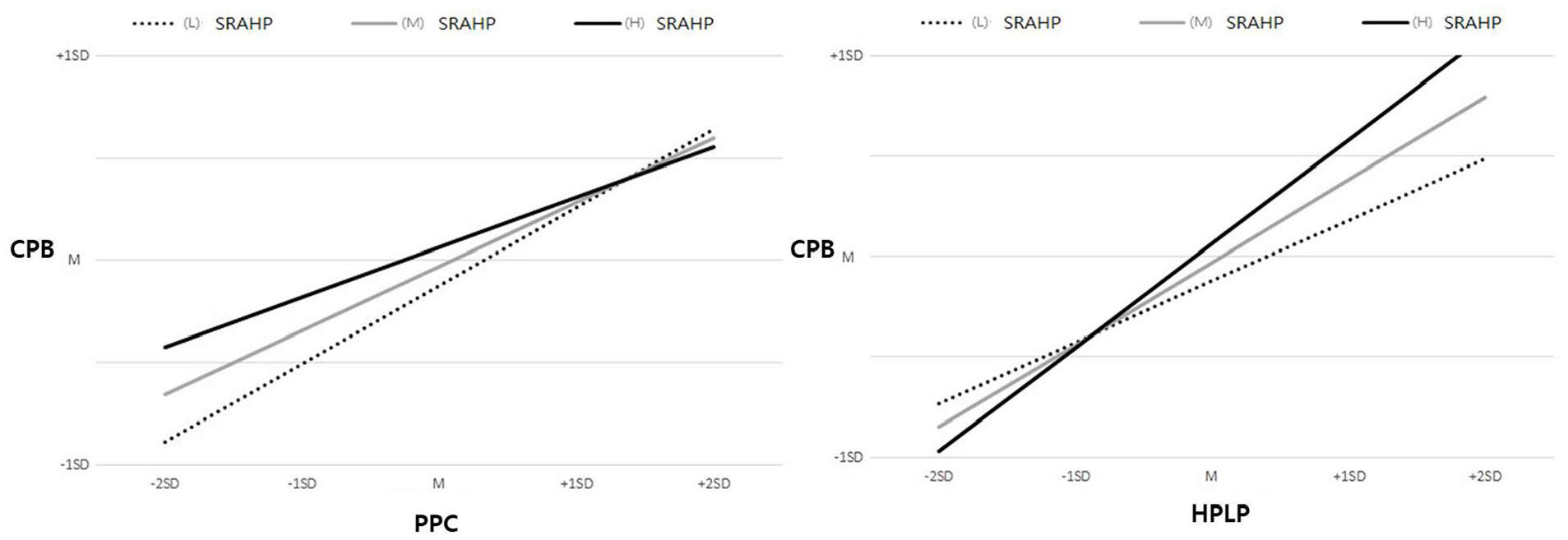
Graph of moderating effects for SRAHP.
Discussion
The scores of each variable among undergraduate students were PPC = 4.02, SRAHP = 2.52, HPLP = 2.75, and CPB = 3.28, all of which corresponded to a moderate level on the respective scales. The scores reported in studies investigating the same variables before the COVID-19 pandemic were PPC = 4.19 in Kim 36 and HPLP = 2.76 in Ryu and Park. 44 These scores are similar to the scores in this study. For SRAHP, a direct comparison was difficult because of the lack of studies reporting on undergraduate students. However, in Nam and Lee’s study, 45 the score range of subcategories of SRAHP was 3.12 to 4.12 among undergraduate students with a major unrelated to sports, implying a decrease in SRAHP, compared to the time before the COVID-19 pandemic.
In contrast, CPB showed an overall increase, compared to previous studies: 3.19 in Kim and Kim 43 and 3.03 in Kim. 46 Nonetheless, analyzing the variation according to the general characteristics showed that the CPB was the lowest for students with an art major, presumably because the students had to take only online classes in a field that requires face-to-face practical courses.47,48 This is in line with the work of Jang, 49 who reported that the low concentration in students during an online practical course was reflected in the output, while the course delivery itself was ineffective. In addition, for online classes, the students mainly partaking in video lectures showed a low level of CPB, which may be because of the absolute influence of time management on CPB, which causes a learning gap among students. However, video lectures were preferred to real-time online lectures because of the freedom in selecting when to watch the lecture. Thus, the results indicated that online classes during the COVID-19 pandemic impacted undergraduate students’ CPB.
We took a multidimensional approach when examining the factors influencing CPB during online classes. The first question was, “How do SRAHP and HPLP affect the relationship between PPC and CBP?” The results showed that HPLP and PPC had a significant positive effect on CPB, whereas SRAHP had no significant effect on CPB.
As a concept focusing on positive psychology in promoting health over disease and merits over demerits, PPC is viewed as an essential factor in overcoming challenges and preparing for the future by developing positive merits.35,50 Thus, it has been reported as a significant influencing factor related to careers in previous studies.51,52 Likewise, PPC was shown to have a significant effect on CPB in the current study, which suggested that personal resources for positive psychology still had significance in CPB, even during the pandemic, with online classes as the main educational format.
Furthermore, while HPLP has not thus far been regarded as a factor influencing CPB, it was shown to have a significant positive effect on CPB in this study. This is significant in identifying the role of HPLP in an environment with online classes. In contrast, SRAHP showed no direct effect on CPB. In general, self-efficacy is a strong influencing factor of CPB, but SRAHP (health self-efficacy) in this study is a specific concept developed to improve health practices in the promotion of health management. 37 Lee 31 reported that self-efficacy and SRAHP converged on a shared concept, but diverged based on low correlation. This study’s results indicated that self-efficacy and health self-efficacy should be distinguished, with respect to CPB.
The second study question was, “Do SRAHP and HPLP show mediating effects after moderation in the dynamics between PPC and CPB?” The analysis showed that SRAHP and HPLP had mediating effects after moderation in the PPC–CPB dynamics, suggesting that PPC ultimately affected CPB. Notably, a high level of SRAHP led to a stronger mediating effect by HPLP. This result necessitated a detailed look into the moderating effect of SRAHP.
We observed a moderating effect of SRAHP in the relationships between PPC and CPB, as well as between HPLP and CPB. Undergraduate students have been provided with positive learning and psychological support programs to self-develop their psychological competence and resolve problems related to their careers and employment.53-55 The results of this study highlight a greater increase in CPB with an increase in PPC for individuals with low SRAHP than those with high SRAHP. This indicated that support should be provided to undergraduates to enhance their CPB by increasing PPC among students with low SRAHP. Comparing the mean scores of SRAHP among different groups of participants in this study showed that the scores were lower for males than for females, for science and engineering majors than for other majors, and for Year 2 students than for other students. In addition, the scores were lower for individuals stating online classes as ineffective than those stating that they were effective. The significantly lower scores for individuals mainly taking video lectures should be considered in the future selection of participants. Alternatively, previous studies on SRAHP mainly targeted individuals with specific diseases. 56 Thus, there is a lack of primary data on general undergraduate students. Therefore, studies should continue to investigate the factors influencing SRAHP in undergraduate students taking online classes.
In numerous domestic and international studies, an increase in self-efficacy led to an increase in HPLP, 43 suggesting that self-efficacy is a powerful predictor of HPLP. In the current study, the group with high SRAHP showed a greater increase in CPB with an increase in HPLP than the group with low SRAHP, suggesting an intensifying effect. Therefore, to enhance CPB effectively in the undergraduate education field, a form of management should be provided to relay high SRAHP directly to high HPLP. This study showed that SRAHP was significantly higher among Year 1 students than among Year 2, 3, and 4 students; hence, if health management is undertaken during the first years, when SRAHP is high, it will be effective in increasing CPB. This phenomenon is predicted to be caused by the shorter length of total exposure to risk factors that come with the university culture in Korea, such as drinking and smoking. However, as there is insufficient evidence due to the absence of past studies, it is anticipated that discussions based on this finding will continue in the future.
Applying the Johnson–Neyman method in analyzing the moderating effect of SRAHP, a significant effect was found for 97% of participants in PPC–CPB dynamics and 99% in HPLP–CPB dynamics. This suggested that SRAHP and HPLP, with a direct effect on CPB, had a notable impact on CPB in most undergraduate students as a moderating factor.
These results highlight the importance of paying attention to multidimensional health management to enhance career preparation behaviors among college students learning on online platforms and suggest that colleges must provide health management along with psychological support as a part of their educational services.
Considering the contributions of this work, 1 key strength of this study is that while health-related properties have not been a central focus in studying career preparation behaviors among college students, we analyzed both the psychological aspect (self-efficacy for health management) and behavioral aspect (health-promoting behaviors) of health management as a predictor of career preparation behaviors. Coccia (2022) suggested that, although no countries were perfectly prepared for a pandemic, 1 common feature among those countries that have managed the crisis well was that these countries have a public governance, as well as financial resources for the health care system, which also played an important role. 57 Colleges must therefore be equipped with a department dedicated to managing students’ psychological, social, and physical health, as well as the required manpower; furthermore, awareness on this matter should be raised through national policies.
Finally, online education will continue to be utilized even after the end of the COVID-19 pandemic, as online education has seen tremendous advances during the pandemic. Because our study data were collected in a special situation in Korea, where all education were transitioned to online platforms as a result of the pandemic, our findings will serve as useful foundational data for establishing public governance, based on technical advances, in preparation of the future, and possibly another pandemic. Moreover, the results of our study provides evidence for defining the roles of health managers in college education settings in the future.
Conclusion
Resulting from the COVID-19 pandemic, the educational format was rapidly converted to an online model, with which educators and students have become familiar. In such changes, efforts to enhance the CPB level in undergraduate students play an important role in the undergraduate education field. The findings of this study on undergraduate students taking online classes suggested that to aid with CPB, an improved PPC was necessary. During that process, the effects were higher if the level of HPLP was higher. Thus, as the physical activities and lifestyle patterns may change in students with the change in their learning environment, there should be more focus on undergraduate students’ health.
Furthermore, based on the moderating effect of SRAHP, as identified in this study, the undergraduate education field should ensure that the health-related psychological confidence in students is raised and relayed to actual health practices. Therefore, the perceptions about health problems among young adults must be transformed both socially and in policies, and colleges should pay attention to students’ health from their first year and systematically promote health-promoting behaviors and resolve health problems by employing health management experts and instituting departments dedicated to this purpose. Such effort will lay the grounds for college students to design their future and prepare for their careers even during a crisis, such as the pandemic. However, this study involved only college students in Korea and thus cannot be generalized. Further studies are needed on more diverse racial groups from more countries, based on our results.
Footnotes
Acknowledgements
The authors express sincere gratitude toward all students who participated in the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2021R1F1A1062667).
CRediT author statement
Hee-Dong, Kim: Methodology, Validation, Formal analysis, Writing—Original Draft, Writing—Review & Editing, Visualization, Myoung-Lyun, Heo: Conceptualization, Formal analysis, Data Curation, Writing—Original Draft, Writing—Review & Editing, Supervision, Project administration, Funding acquisition.