
Abstract
Heart failure is a progressive condition with a high burden of symptoms and clinical decompensations that causes psychological and social suffering, poor quality of life, and limited life expectancy. Therefore, it requires palliative care to control symptoms and signs, but integrating it with clinical care is complicated. We aimed to discuss the limits and possibilities of integrating palliative care in heart failure. This was a qualitative descriptive study. Semi-structured qualitative interviews were carried out between July 2020 and July 2021. We applied the thematic content analysis and the SWOT matrix. Ethical principles were respected. Ten professionals from an Institute specializing in cardiovascular diseases in Rio de Janeiro, Brazil, participated in the study, including physicians, nurses, psychologist, and occupational therapist. We identified 4 categories related to intervening factors: the patient’s profile, the emotional aspects of professionals facing these patients, the challenges to integrating and sustaining palliative care in practice, and the ways for assistance planning in this context. The existence of a specialized team, the palliative care commission, and the institutional palliative care protocol, aligned with the realistic perception of the assistance, organizational, political, and social problems, may promote the advancement of palliative care in heart failure.
● Heart Failure (HF) is the common outcome of the different diseases that affect the heart, with a high prevalence and mortality rate in the world, requiring person-centered care. ● Integrating palliative care with clinical care in HF is difficult, even in advanced HF. The lack of clarity about the trajectory of the disease, knowledge about palliative care and resources are highlighted. ● Palliative care in this context still occurs frequently at the end of the illness.
● The main health professionals’ perception about the factors that influence the integration of palliative care involved the profile of the HF patient: patients with worsening symptoms and functionality, who are unaware of the disease, arrive late to the specialized service, abandon treatment and suffer from lack of socioeconomic resources. ● Even in an Institute with a specialized team responsible for overseeing palliative care to patients with HF, there are difficulties in transforming the practice, mainly due to the lack of knowledge about palliative care by the remaining health professionals, patients, and family members. ● All factors in the integration of palliative care in HF must be contextualized. As a country in economic development and among those that provide palliative care in a generalized way, the setting evidenced strengths, such as an internal commission of palliative care, weaknesses, such as the biomedical model, opportunities in legislation and in national health system, but also threats, such as those identified in the profile of the HF patient, with difficulty in following treatment due to lack of socioeconomic resources, with portrays social inequality in the country.
● To implement actions to strengthen palliative care in HF, such as educating patients, families and health professionals about palliative care, emphasizing good communication as fundamental for this implementation. ● To create integrations between sectors and services in health organizations in order to develop models suited to each reality, advocating the recommendations of the guideline on HF and palliative care. ● To work on the limits and possibilities of integrating palliative care in HF, based on the promotion of a palliative care policy for the entire health system. For this, it is essential to review the guidelines to standardize the recommendations for the integration of palliative care in HF.
Introduction
Heart Failure (HF) is the common outcome of the different diseases that affect the heart. It is estimated at 26 million the prevalence of cases worldwide, with the prospect of increasing over the years, with the population aging as one of the main factors. The mortality rate from HF is high and may be underestimated if it is not considered the primary cause of death. The universal definition of HF that is clinically relevant in the global context is recent, having been published in 2021, which requires communication to transfer this knowledge to practice. Among the importance of this definition is the best evidence for shared decision-making and transitions of care between levels of care and therapy goals, which includes the integration of palliative care.1-4
In this opportunity, we disclose the definitions of the HF: “a clinical syndrome with symptoms and/or signs caused by a structural and/or functional cardiac abnormality and corroborated by elevated natriuretic peptide levels and/or objective evidence of pulmonary or systemic congestion.” 4
Based on this definition, HF is a progressive and persistent condition with a high burden of symptoms and clinical decompensations, often combined with increased psychological and social suffering, poor quality of life, and limited life expectancy over time.4,5 This set of conditions requires a palliative care approach, defined as an “active holistic care of individuals across all ages with serious health-related suffering due to severe illness.” 6
Thus, it is imperative in health care planning, goals related to the control of symptoms and signs that affect all these spheres,7,8 being the management of care by an interdisciplinary team in a continuous and person-centered way essential to improve the quality of life. 9 Well-controlled signs and symptoms in HF allow care management to be coordinated by primary care, in a network with the specialty outpatient clinic (cardiological and palliative), and other services/specialty that may be necessary, opening space for this care to be carried out directly in the community, reducing hospitalizations, and health costs to sustain the health economy. 10
Although there is no consensus in clinical guidelines on the timing of starting palliative care in HF, in line with the American Heart Association and the Global Atlas of Palliative Care, we advocate that starting palliative care as early as possible, in line with expectations and needs of each person with HF, integrated with the clinical care in HF, gradually increasing its approaches, respecting the will of the person and in response to the worsening of the signs and symptoms of HF, and evolution of its phases.11-13
However, integrating palliative care with clinical care in HF is difficult, even in advanced HF. The lack of clarity about the trajectory of the disease, professionals’ insufficient knowledge about the specialty competence of palliative care in the control of symptoms and signs, as well as the lack of resources to structure and maintain outpatient palliative care programs and home care, are many of the obstacles that contribute to the person with HF not having access to palliative care. 14 Despite scientific evidence reinforcing the importance of integrating palliative care to improve the overall quality of life and to reduce negative economic pressure on the public-private health system, barriers to this integrated care persist in practice, which still varies widely between geographic regions, in addition to the serious access difficulties, when compared, for example, to the context of oncology.11,15
Given this evidence, we aimed to discuss the limits and possibilities of integrating palliative care in HF.
Methods
Research Question
How do health professionals perceive the limits and possibilities of integrating palliative care in HF?
Design
The study design has a qualitative, descriptive, and exploratory approach.
Setting
The setting was a public Institute specializing in complex heart diseases, in Brazil. In 2018, a palliative care program for people with advanced cardiovascular diseases began in the Institute, carried out by a multi-professional team specialized in palliative care, working in the HF inpatient service. This service operates in an infirmary with 9 beds, and the health team has 7 physicians, 11 nurses, a psychologist, and an occupational therapist.
Part of this team (one doctor, 2 nurses, the psychologist, and the occupational therapist), in the same year, became part of that recently created Palliative Care Commission to advise the services and departments on decisions involving palliative care.
Faced with no clarity about the course of the disease and insufficient knowledge of health professionals about palliative care, this commission developed a clinical protocol to systematize the eligibility criteria for integrating palliative care in HF, formalize the clinical evaluation tools for assistance planning, and describe the role of each team member (nutritionist, nurse, occupational therapist, physical therapist, psychologist, and social worker) in the activities of general/primary palliative care. Whenever necessary, in the scope of specialized palliative care, the commission members accompanied patients hospitalized in other infirmaries, intensive care, or outpatient clinics.
Population/Sampling
For purposive sampling, 10 professionals from this HF inpatient service participated in the study: 5 nurses, 3 physicians, 1 psychologist, and 1 occupational therapist. All had employment relationships and experience working in the service for at least 1 year. Five nurses were not included as they were recently hired. Some medical leaves and numerous changes in work routine due to the COVID-19 pandemic made it difficult for professionals to participate. We extended the data collection period to solve this problem, which took place between July 2020 and July 2021. Even so, 3 physicians from the team could not participate in the study due to their workload.
Data Collection
Data collection was carried out by the main author, a nurse, who was pursuing her master’s degree in nursing and post-graduate studies in the residency modality in that same setting, bringing her closer to the institution and the participants before the study began.
A semi-structured interview was applied, with the questions: how do you perceive the patient with HF from your experience? How do you perceive palliative care for patients with HF? What does it mean for you to assist patients with HF in palliative care? How do you understand integrating palliative care in HF? What can hinder or facilitate this integrating? She also asked some complementary questions to deepen the phenomenon of interest. Before starting the interviews, the researcher applied close-ended questions to determine the professional profile.
Interviews were carried out individually, in a private and quiet room, at the Institute, outside the participant’s working hours. The average duration of the interview audios was 25 min. Interviews did not need to be repeated or had their transcribed content altered after the participant validation. Field notes were made after the interviews.
Data saturation started to be observed from the fifth interview onward, which may be related to the fact that all study participants come from one team. To minimize this bias, we tried to guarantee representativeness in the groups of physicians and nurses. And although the team only had one psychologist and one occupational therapist, we observed that their speeches maintained the pattern of repeating the information.
Data Analysis
We employed content analysis in the thematic modality. 16 Two authors were involved in this analysis, performed manually in all its phases; the discussions in evaluation boards of the master’s course and in the research group with the other authors contributed to reducing bias.
The SWOT matrix (an acronym for Strengths, Weaknesses, Opportunities, and Threats) 17 was used to summarize information and help to discuss the limits and possibilities of integrating palliative care in HF. Thus, we developed thematic units in a mixed manner. One part was derived from data, and another was identified according to the questions and objectives beforehand.
The commitment to the investigated phenomenon, the dedication of sufficient time for data collection and its continuous review conferred methodological rigor. The author responsible for data collection established a good relationship with the participants. All stages of the study were independently reviewed by seasoned professors and discussed in groups during the stages of evaluation of the master’s degree.
Ethical Issues and Approvals
The research project was approved by the Research Ethics Committee on March 21, 2020. We submitted to each participant the purpose of the study and the ethical issues surrounding the research. All were aware that they could withdraw at any time, without prejudice, and in agreement with the study, they signed the Informed Consent Form.
Alphanumeric codes identified the excerpts from the interviews with the letter E for the interviewee and its sequential number to guarantee anonymity.
Results
The following characteristics of the professional profile stood out: 9 participants were female; 5 were between 31 and 40 years old; the training time ranged between 2 and 25 years, and the experience in palliative care was concentrated between 2 and 4 years. Four professionals had post-graduation in palliative care.
Four thematic units emerged (Figure 1).

Thematic units and subcategories. Rio de Janeiro, Brazil, 2021.
Thematic Units 1. Profile of the HF Patient
The professionals highlighted the patient’s profile, once the clinical condition is complex and capable of affecting all dimensions of people’s lives.
[. . .] is a frail, limited patient, especially in the advanced stage; an individual with many losses in their social and family space, ending up with great anguish. Considering motor and psychological skills, I see that it is a devastating disease. [. . .]. (I9)
In addition to this profile, it was highlighted that the patient is unaware of the disease, its evolution and therapeutic regimen.
It’s a patient with a very high burden of symptoms, little knowledge about the disease, treatment, and prognosis. It’s some sort of a lost patient; many already have a long-time evolution of the disease [. . .]. It is a sad, depressed patient who often feels that they are losing and that the therapies have failed. All those HF symptoms keep worsening, and the quality of life is poor. (I4)
A differential of these patients is the delay in changing their physical appearance, which was associated with a delay in self-perception of the severity of the disease and its evolutionary stage, as well as a factor that influences adherence to therapy.
Patient with cancer knows they will be bald; they visualize their physical condition. As patients with HF often have no physical change, in the beginning, they get well structurally before reaching the stage of cachexia. Until they understand the severity, there is a very long distance [. . .]. There are many abandonment cases because they get better and do not understand the process of becoming sick [. . .]. (I2)
Patients with financial difficulties face more obstacles to treatment continuity, especially when related to the need for regular attendance at services.
I want to offer a consultation or other service, but he can’t come to the hospital regularly, because he has no financial condition, and the illness prevents him from working [. . .]. Sometimes not having a high level of education is not so important. He doesn’t have much education, but he lives close to the institution and can be here whenever necessary. (I2)
Thematic Units 2. Emotional Aspects of Health Professionals When Dealing With Patients With HF
The extended follow-up periods and the frequent hospitalizations of those patients create the opportunity for a relationship, which reflects in the way the professional deals with the situation, either manifesting frustration for the failure of therapies or withdrawing and protecting themselves psychologically from the losses, which can influence the assistance planning, especially in the determination of when to offer palliative care.
It is a patient that when you can follow the entire history, you even feel some burden because it starts at the beginning of HF. You invest all your time there in prevention and care, but you see an increase in the progression of the disease, which gives you some anguish because they return many times [. . .]. So, the HF patient is not a short-term patient who went through a procedure and left afterward. It is a patient with whom you create a connection. I try to keep a certain safe distance, but there is no way; you get involved. It is difficult. (I1)
Thematic Units 3. Challenges of Integrating and Maintaining Palliative Care in Practice
Although the institution is working to overcome some challenges to integrate and maintain palliative care practice in HF, the problems have strong roots in the model of care, the budget deficit, and cultural factors related to the disease and death, which impact the assistance microenvironment context. In addition to the following reports, a summary of what was presented is shown in Figure 2.

Challenges of the microenvironment of the investigated context. Rio de Janeiro, Brazil, 2021.
[. . .] When you are inside a cardiac specialization hospital of great surgical complexity, everything is focused on the heart, on the surgery. And when there is nothing else to be done for this patient besides an invasive approach that will change the course of the disease, they become terminal, and then they think about calling the palliative care team when it is already late [. . .]. But every professional should already have this perspective of palliative actions because we do not have enough professionals to provide specialized palliative care [. . .]. (I9) [. . .] we still have high turnover in nursing, and until you reinsert that group, that professional, within that care or that protocol, it’s not easy. So, this is also a difficulty because nursing ends up being our pillar, and when you get through those changes, that pillar gets to be a little hollow inside. (I10)
Internal problems relate to other external issues, from the macroenvironment system problems that undermine palliative care. In addition to the following reports, a summary of what was presented is shown in Figure 3.
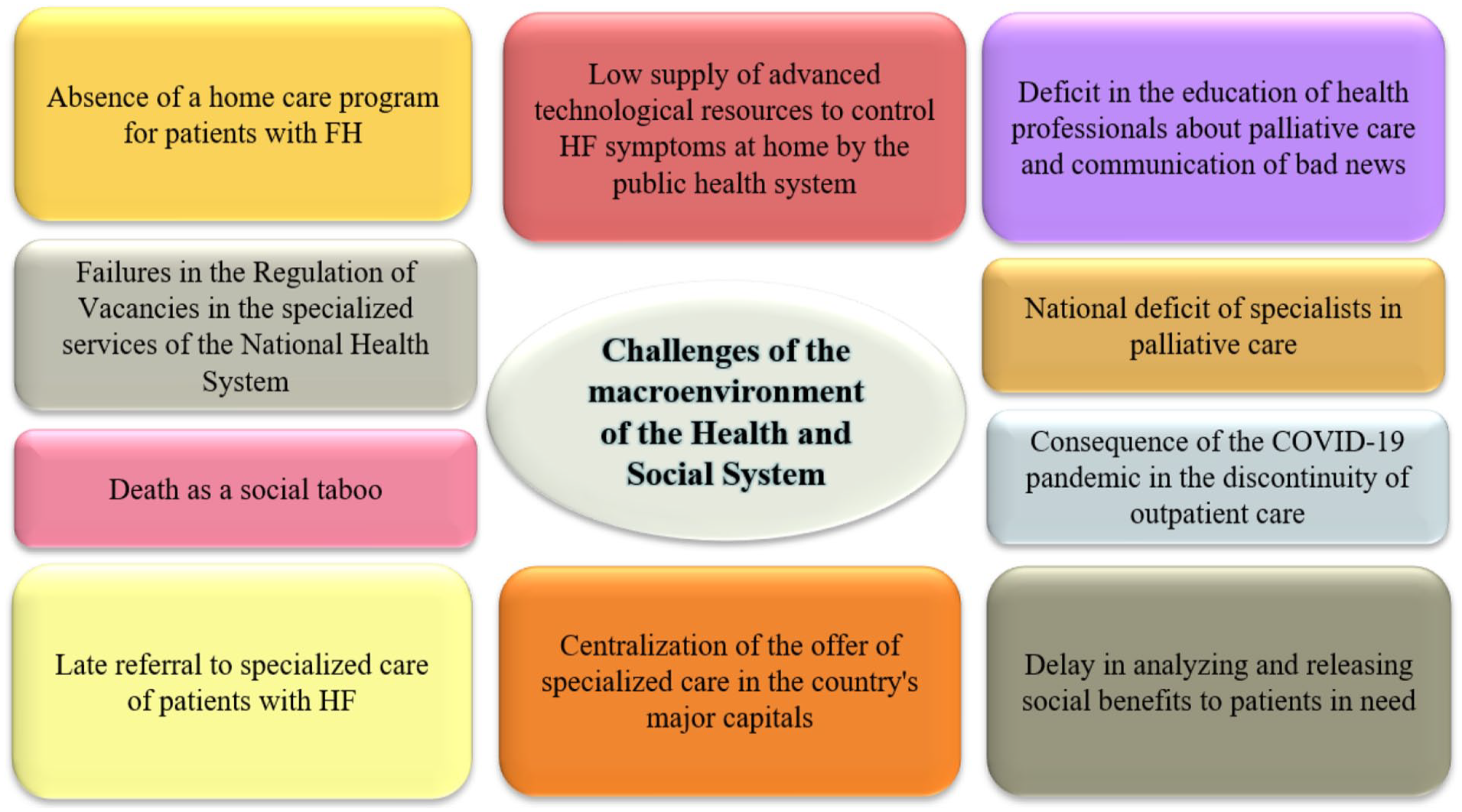
Challenges of the macroenvironment of the Health and Social System. Rio de Janeiro, Brazil, 2021.
[. . .] when we study palliative care, we notice that the ideal death is at home in the countries where that notion is more widespread among the population. But to do so, there must be a structure, a trained multidisciplinary team, material, and preparation of the patient and family, because it is not easy. In our case, death usually occurs in hospitals, and a patient with advanced disease in the hospital will invariably be subjected to procedures that will not make a difference in the outcome and will at some point undergo therapeutic futility [. . .]. (I8) Some patients live far away and cannot follow the treatment properly. So, it’s not that they don’t understand, but they can’t attend the professionals’ appointments, so we try to manage and make all the appointments on the same day. Sometimes it is not feasible because it takes the whole day, and the patient comes with city transportation [. . .]. (I2)
Thematic Units 4. Directions of Care Planning for Patients With HF in Palliative Care
From the factors that threaten the integration of palliative care, the participants pointed out strengths and opportunities, despite the damage caused by the pandemic.
The multidisciplinary team helps a lot because there are more people looking at the same issue and pointing out from their perspective something that will add up to our needs. (I8) Make the patient feel useful. When the patient participates in the care, understands their disease, and knows what palliation is, it is entirely different. When patients get involved, we avoid facing difficulties with the treatment, and there are not so many barriers. (I6)
To summarize the quotes of this thematic unit, the SWOT matrix was applied (Figure 4), according to health professionals’ perceptions about the intervening factors to integrating palliative care in the assistance planning for a person with HF.

Application of the SWOT matrix in the investigated context. Rio de Janeiro, RJ, Brazil, 2021.
Discussion
The aspects that characterize the progression of HF are likely to negatively influence the patient during the course of the disease since they imply increased demand in the management of care and impair their ability to self-care and, consequently, to provide sufficient resources to maintain their well-being. The frequency of clinical decompensations, the progressive intensity of symptoms, and emotional imbalance are devastating consequences of HF, and social deprivation further disrupts adherence to treatment and quality of life. 18
Our data reveal that even in an Institute with a specialized team responsible for overseeing palliative care to patients with HF, there are difficulties in transforming the practice, mainly due to the lack of knowledge about palliative care by the remaining health professionals, patients, and family members. In a similar study conducted in Australia, it was noted that even in countries where access to palliative care is widespread, there are very similar barriers to the institution of this care in HF, such as the clinical profile of the patient, the education needs of health professionals, patients, and families on palliative care, as well as the acceptance of this care by the patient. 19 It is perceived, many times, that the unawareness, especially of the patients, about their disease and its evolution, does not favor the opening for discussion about palliative care. 20
Among the strategies to minimize the lack of knowledge about palliative care in HF, a recent study applied weekly telehealth sessions led by palliative care nurse specialists to discuss relevant topics such as self-care, symptom management, and decision making. These interventions improved quality of life-related outcomes at week 16, but not at the end of the intervention at week 32, when the positive effects could not be maintained or were not as pronounced as at the beginning of the intervention; and patients who completed the entire intervention did not have less use of health care resources, such as emergency department visits, at 16 or 32 weeks. The authors claim that identifying clinical signs or screening in the clinic to provide an early indication of palliative care in HF remains difficult because palliative care in this context often occurs at the end of the disease. 21
Although patients with HF can manifest very limiting and long-lasting symptoms, the variable prognosis of the course of the disease, with possibilities of life-prolonging therapies, makes it difficult to decide when to start palliative care.20,22,23 Thus, in harmony with what is recommended by the World Health Organization, the authors defend the beginning of palliative care at the diagnosis of HF, assuming that all health professionals can perform generalist/primary palliative care and that includes attention to biopsychosocial needs, creation of a relationship, consideration to the family and communication for decision-making. The offering of palliative care is a fundamental addition to the care of patients with HF and their families; however, not only in Brazil but also worldwide, there is still a shortage in the allocation of resources and few human resources specialized in palliative care. Therefore, the education in generalist/primary palliative care for teams watching patients with HF presents an opportunity to fill this gap and ensure that they receive the highest quality of care across the spectrum of their disease, from diagnosis to death. 24
Evidences show the potential benefits integrating palliative care along the path of HF to increase quality of life. Examples of these benefits are adherence to treatment, stimulation of self-care, and better symptom control, among which the improvement in pain, dyspnea, intolerance to exertion, anxiety, and depression stand out, contributing to well-being, and emotional and spiritual comfort. 13 However, there is disagreement among clinical care professionals in HF regarding the ideal time to start palliative care for each stage of the HF, mainly because it is a long-term disease with better clinical stability, unlike oncology, which due to the characteristics of its evolution, favors prognosis, and patient recognition of palliative care. Hence the importance of thinking about early integrating palliative care in the management of chronic illness, such as HF, to meet the expectations and needs of each person, as they manifest themselves, considering the complexity of self-care and the impact of the disease on everyday life.13,14,25
According to a recent review, to overcome the challenge of integrating palliative care in HF, it is necessary to address key elements in the clinical, professional, organizational, and health care levels for those patients. For that, it is required to work on promoting a palliative care policy for the entire health system, create integration between sectors and services in health organizations, and develop models appropriate to each reality, recommending HF guidelines endorsements and palliative care. Moreover, in the professional sphere, promote the education of health professionals involved in the provision of HF care, emphasizing the fundamental part of good communication in implementing palliative care. In the clinical sphere, it is necessary to work with an assistance philosophy focused on the patient as the center of care and to be aware of the early involvement of the principles of palliative care. 26
The study participants reinforced the issue of the patient’s late arrival in specialized assistance. This fact reveals that the curative care model is one of the main weaknesses of the microenvironment policy in the investigated context, for not attributing importance to palliative care, especially when the patient arrives late to the hospital and specialized care. Besides the profile of the patient with HF highlighted in this study, it must be considered that this patient has traveled a tiring, arduous, long, and confusing pathway until arrival at the hospital. And the outcome of arriving at the specialized hospital may even provide false expectations given the prognosis of that already advanced disease.
A study conducted on the elderly with HF brought interesting results to this analysis on initiating palliative care. The study highlighted frailty as a multidimensional construct of cumulative deficits to assess the importance of the main clinical problems and events that result in the use of health care resources, with decision-making on assistance planning based on 2 directions, from aggressive management to a palliative approach. There is no discourse on joint and integrated care, but rather one or the other, in the way of referral to palliative care. Interestingly, of the 204 patients who died during the study period, 113 (55.4%) were referred for palliative care without evidence of life expectancy since that referral. However, less than 50% of the non-fragile or mildly frail patients were referred for palliative care. Overall, the referral rate was relatively low compared to the high and early mortality. 27
We highlight the importance of the outpatient clinic for the practice of specialized palliative care integrated into the care of patients with HF. The literature suggests the strengthening of nurse-led outpatient HF clinics. They would reduce hospitalizations and premature death by facilitating personalized follow-up, with connections that contribute to controlling symptoms and signs of the disease since nurses, in the context of nursing care, tend to begin palliative care earlier than physicians.20,28,29
Strengths and Weaknesses
The main strength of this study is to objectively present which factors can influence integrating palliative care in HF. The SWOT matrix produced structured results, relating the internal and external factors that influence this integration. There is also a guide to practice, highlighting the actions that must be maintained, improved and incorporated, which based on the discussion, can be applied in other contexts (Table 1). Despite the limits of human resources with experience in palliative care, this study addressed the multidisciplinary team, which, through in-depth interviews, presented an integrated and detailed view of the phenomenon.
Actions That Can Strengthen the Implementation of Palliative Care.

However, the participation of only 10 professionals from the same team was a limitation, considering that any integration proposal requires the participation of all those involved. In this case, in addition to the saturation criteria, we must consider the lack of calculation and justification for the sample size selected in this study.
The setting, specialized in cardiology, is another limiting factor, considering that most of the population with HF is treated in general hospitals, which can interfere with the generalization of results for integrating palliative care. The study needs to be expanded to other settings, including primary health care, with the participation of other professionals, such as clinical care in HF, patients and family member.
Implications for Clinical Practice and Policy
To synthesize the implications for practice and policy, the Table 1 shows a set of actions that can strengthen palliative care, according to the experience of the study setting.
Conclusion
The participants highlighted factors that hinder integrating palliative in HF such as characteristics of the patient’s profile involving the severity of symptoms and signs, poor quality of life, lack of knowledge of the disease and its progression, late start of treatment and risk of discontinuity because of socioeconomic factors. In addition to causes related to the biomedical model, the low investment in palliative care in the health care network, the difficulty in clinical judgment and decision-making about for whom, how, and when to palliate.
The professionals’ perception is realistic, based on practice, but limited to the fact that they are part of the same team. However, this purposive sampling sought to give visibility to the results that this team has already achieved, and to contribute to changing the institutional culture of integrating palliative care in HF.
All limits and possibilities of integrating palliative care in HF, aligned with the expectations and needs of each person, must be contextualized to better structure the action plan, and thus promote integrated care, improve the quality of life, and sustain systems of health.
Supplemental Material
sj-doc-2-inq-10.1177_00469580231160897 – Supplemental material for A Qualitative Study of the Limits and Possibilities of Integrating Palliative Care in Heart Failure
Supplemental material, sj-doc-2-inq-10.1177_00469580231160897 for A Qualitative Study of the Limits and Possibilities of Integrating Palliative Care in Heart Failure by Karoliny Alves Santos, Liana Amorim Corrêa Trotte, Audrei Telles, Tereza Cristina Guimarães, Eunice Sá and Marcelle Miranda da Silva in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-1-inq-10.1177_00469580231160897 – Supplemental material for A Qualitative Study of the Limits and Possibilities of Integrating Palliative Care in Heart Failure
Supplemental material, sj-docx-1-inq-10.1177_00469580231160897 for A Qualitative Study of the Limits and Possibilities of Integrating Palliative Care in Heart Failure by Karoliny Alves Santos, Liana Amorim Corrêa Trotte, Audrei Telles, Tereza Cristina Guimarães, Eunice Sá and Marcelle Miranda da Silva in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-3-inq-10.1177_00469580231160897 – Supplemental material for A Qualitative Study of the Limits and Possibilities of Integrating Palliative Care in Heart Failure
Supplemental material, sj-pdf-3-inq-10.1177_00469580231160897 for A Qualitative Study of the Limits and Possibilities of Integrating Palliative Care in Heart Failure by Karoliny Alves Santos, Liana Amorim Corrêa Trotte, Audrei Telles, Tereza Cristina Guimarães, Eunice Sá and Marcelle Miranda da Silva in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to thank the professionals who participated the study.
Author Contributions
Conceptualization, Karoliny Santos and Marcelle Silva; methodology, Karoliny Santos and Marcelle Silva; formal analysis, Karoliny Santos, Liana Trotte, Tereza Cristina Guimarães and Marcelle Silva; investigation, Karoliny Santos; data curation, Karoliny Santos and Marcelle Silva; writing—original draft preparation, Karoliny Santos and Marcelle Silva; writing—review and editing, Karoliny Santos, Liana Trotte, Audrei Telles, Tereza Cristina Guimarães, Eunice Sá and Marcelle Silva; visualization, Karoliny Santos, Liana Trotte, Audrei Telles, Tereza Cristina Guimarães, Eunice Sá and Marcelle Silva; supervision, Marcelle Silva; project administration, Karoliny Santos and Marcelle Silva; funding acquisition, Eunice Sá and Marcelle Silva. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Nursing Research, Innovation and Development Centre of Lisbon (CIDNUR).
Ethical Approvals
The research project was approved by the Research Ethics Committees of the Escola de Enfermagem Anna Nery and Instituto Nacional de Cardiologia on March 21, 2020 (report no. 3.927.652).
Informed Consent Form
You are being invited to participate as a volunteer in the research entitled: “Integrating Palliative Care in the Assistance Planning for People with Heart Failure,” which has as objectives: to identify health professionals’ perceptions about the factors intervening in the integration of palliative care in assistance planning for a person with heart failure and discuss the limits and possibilities of that integration.
Your participation is not mandatory and will consist of a semi-structured interview with open questions and filling out a form with personal data, in order to enable a better characterization of the sociodemographic profile of the interviewees. The interview will be held in your work environment in a private place, according to your available time, seeking not to interfere with the routine of the service. An mp3 audio device will be used to record the interview content and the statements will be transcribed and identified by alphanumeric codes. You may withdraw your consent at any time from participating. The refusal, withdrawal or suspension of your participation in the research will not result in prejudice. You will not incur any expenses and you will not receive any remuneration either.
The risks of this research are minimal, since it may cause discomfort in the psychic, moral, cultural and spiritual dimensions during the interview responses when addressing aspects of palliative care and the end of life process, allowing for self-reflection on them. The researcher undertakes to interrupt the interview at any time, according to her own will, and if any discomfort occurs that is harmful to her health, the psychology service of the institution will be called and assistance requested. In case of damage demonstrably arising from the research, you will be entitled to compensation through judicial channels, as provided in the Civil Code, the Code of Civil Procedure and Resolution No. 466/2012, of the National Health Council (CNS).
If you agree to participate, you will be contributing to the future improvement of care provided by nurses and other health professionals to patients with chronic HF in palliative care, based on the results achieved by this study.
The data collected will be used only in this research and kept in a physical and/or digital file under the custody of the researcher for a period of 5 (five) years after the end of the research.
You will receive a copy of this term containing the contacts of the Research Ethics Committees - CEP, the researcher in charge and the other members of the research team, being able to eliminate your doubts about your participation now or at any time. If you agree to participate in this research, sign at the end of this document, which has two copies, one for you and the other for the responsible researcher.
Data Availability Statement
The data used during this study are available from the corresponding author, under request by e-mail.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.