
Abstract
Background:
Effective management of frequent users of emergency departments (FUED) remains challenging. Case management (CM) has shown to improve patient quality of life while reducing ED visits and associated costs. However, little data is available on FUED’s perception of CM outside of North America to further improve CM implementation.
Objectives:
Explore the FUED’s perspectives about CM in Switzerland.
Design, Setting & Participants:
Semi-structured qualitative interviews eliciting FUED’s experiences of CM were conducted among 20 participants (75% female; mean age = 40.6, SD = 12.8) across 6 hospital ED.
Outcomes measures & Analysis:
Inductive content analysis.
Main Results:
Most participants were satisfied with the CM program. In particular, FUEDs identified the working relationship with the case manager (cm) as key for positive outcomes, and also valued the holistic evaluation of their needs and resources. Overall, patients reported increased motivation and health literacy, as well as facilitated interactions within the healthcare system. Conversely, a small number of participants reported negative views on CM (ie, stigmatization, lack of concrete outcomes). Barriers identified were cm’s lack of time, COVID-19′s negative impact on CM organization, as well as lack of clarity on the objectives of CM. FUED perceived CM as useful, in particular establishing a working relationship with the cm. Our results suggest that CM can be further improved by (1) professionals remaining non-judgmental toward FUED, (2) making sure the aims and objectives of the CM are understood by the participants, and (3) allowing more time for the cm to carry out their work.
Case Management (CM) improves quality of life of Frequent Users of Emergency Department (FUED; >5 ED visits/year), reduces the number of ED visits and associated costs.
Our research provides insights into FUED’s perception of CM and identifies points for improvement.
Findings confirm that CM meet the target population’s needs, addressing the barriers identified by FUED in CM may help improve CM’s effectiveness.
Introduction
Overcrowding of Emergency departments (ED) is a challenge. A minority of patients visit the ED 5 times or more within 12 months and are defined as frequent users of ED (FUED). 2 A study conducted in Lausanne, Switzerland, established that 4% of ED patients accounted for 12% of all ED visits. 1 FUED often cumulate mental and physical comorbidities, substance abuse as well as social problems.1-3
In response, interventions tailored to FUED needs have been developed, such as case management (CM). CM is based on the global management of patients. Case managers (cm) provide counseling on healthcare system utilization and social issues. Moreover, cm redirect FUED to a range of community-based and hospital services, facilitating continuity of care. 4 Evidence shows that CM is effective in improving patient quality of life (QoL) while at the same time reducing the number of ED visits and related costs.4-7 No studies have evaluated CM from the user’s perspective outside of North America.8-12 Participants emphasized the quality of the relationship with the cm as CM’s key to the success of the program. Other outcomes identified were help in navigating the healthcare system.
These findings have provided a call for conducting more qualitative research on FUED’s experience of CM in other countries. 13 Considering the important differences in healthcare systems across countries worldwide, it is important to explore how the abovementioned findings are transferable outside of North America. Switzerland’s healthcare system differs from US and Canada’s in that it provides insureds universal coverage based on compulsory health insurance. Insureds pay private insurers to cover healthcare costs, although according to the modality of health insurance chosen, patients must additionally contribute out-of-pocket toward incurred healthcare costs.
To the best of the authors’ knowledge, no qualitative research has explored FUED’s perspective on CM in a country with a health insurance system comparable to the Swiss one. To fill this gap and to contribute to this important line of research, this study aimed to explore FUED perspectives on CM in the French-speaking part of Switzerland. Specifically, it aimed to explore FUED’s experience and opinion of CM, as well as its usefulness, benefits, positive and negative aspects, relevance and differences compared with usual care.
Method
Procedure
For over 10 years, the department of Vulnerabilities and Social Medicine of the University Institute for General Medicine and Public Health has collaborated with Lausanne University Hospital’s ED to develop, evaluate, and implement a targeted CM for FUED. CM is therefore an ongoing program. Its implementation, as well as various previous promising findings reported in Lausanne, 6 have led to an ongoing research project investigating the implementation of CM in EDs open 24 hours a day, 7 days a week, in French-speaking Switzerland, 14 in which this current secondary study is nested.
The parent study procedures were based on the 5 stages of the Generic Implementation Framework (GIF) (ie, development, exploration, preparation, operation, and sustainability). 15 During the 6-month’ operational phase, the research team quantitatively assessed participants in the selected EDs to evaluate FUED trajectories after receiving CM. A sub-sample of participants was invited to participate in semi-structured interviews exploring their experience and perceptions of CM. Interviews were conducted by telephone, by a female Master-level psychologist (MG) and a female Master-level medical student (LS), under the supervision of a female PhD senior researcher (VG). Participants received a voucher of CHF 10.- (~10 USD) in compensation for their time. Written informed consent was obtained from all participants in each of the participating ED sites. All procedures were approved by the respective local ethics committee.
Intervention
The cm was comprised of nurses, sometimes teaming up with a physician. They received a common toolkit of resources and training in CM. 16 The first point of contact between cm and FUED took place in the ED, where participants underwent a global evaluation. Next, the cm and the participant identified together the specific needs and objectives of the FUED and scheduled ambulatory appointments. The intervention terminated once the FUED was fully integrated in a functioning healthcare network.
Participants
Similar to the parent study, 14 inclusion criteria were: being 18 years of age or older, having visited an ED 5 times or more within the previous 12 months, and being fluent in French. Exclusion criteria included having fewer than 2 vulnerability factors in addition to ED frequent use (ie, social, somatic, mental health, and risk behavior), incapacity to provide informed consent, plans to leave Switzerland within less than 18 months, life expectancy of 18 months or less, awaiting incarceration or being incarcerated, having a family member already enrolled in the study. For the current study, 2 additional exclusion criteria were added: lack of CM follow up (ie, lack of regular attendance to the CM’s appointments) and incapacity to take part in a qualitative interview. Forty participants were randomly recruited from the 58 FUED in the parent study across the 6 participating hospital EDs in the French-speaking part of Switzerland (See Table 1 for ED characteristics). Twenty FUED agreed to be interviewed (6 refused, 6 were unreachable and 8 were excluded: 4 because of incapacity to do an interview and 4 because of lack of follow-up in the CM program). Participants were more often women (75%, n = 15), and mean age was 40.6 (SD = 12.8). Tables 2 and 3 provide detailed information on participating hospitals participant characteristics.
Emergency Departments Characteristics.

Patient Recruitment by Hospital.

Demographics of the Participants (N = 20).
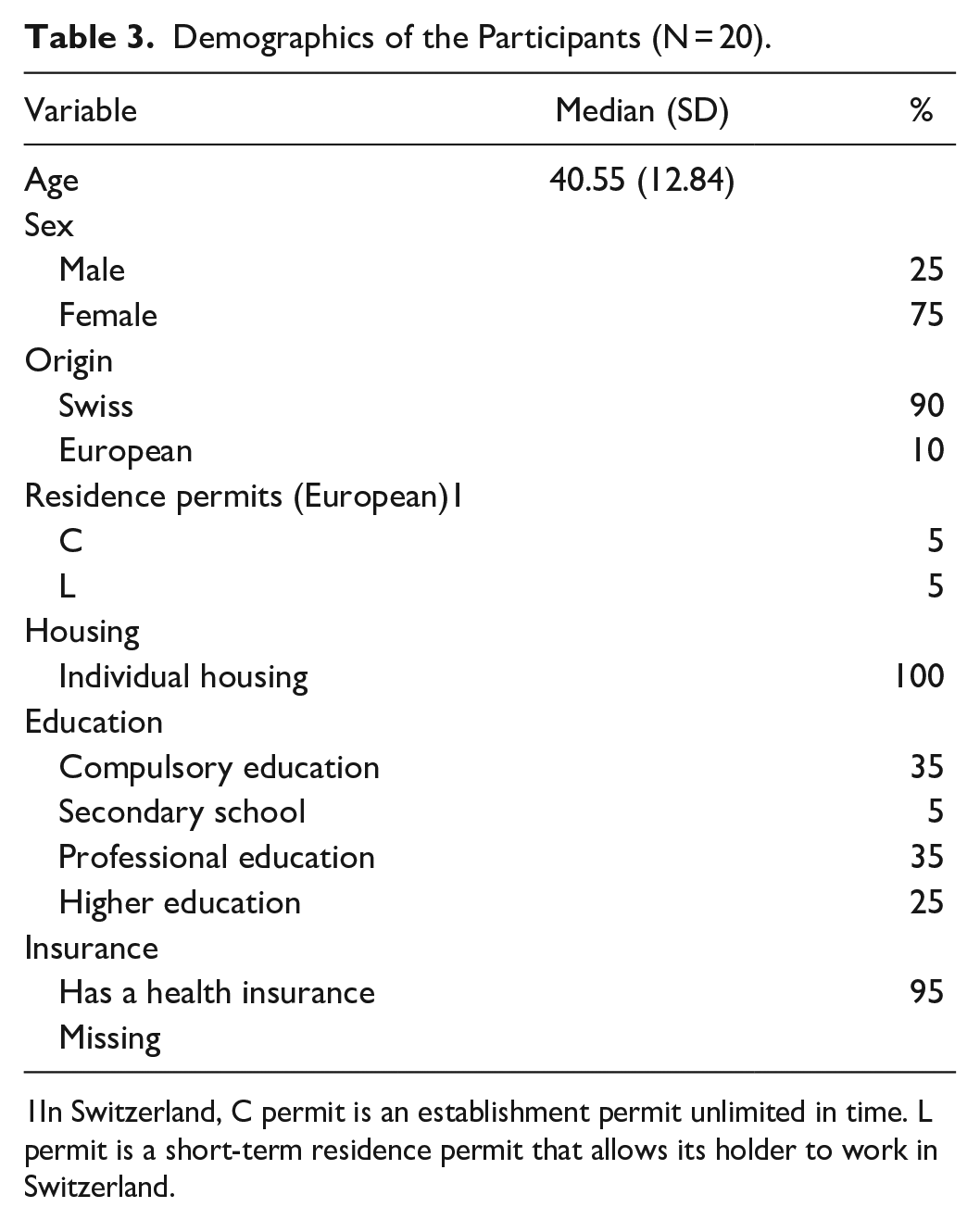
1In Switzerland, C permit is an establishment permit unlimited in time. L permit is a short-term residence permit that allows its holder to work in Switzerland.
Measures
The semi-structured interviews were conducted with an interview guide featuring open-ended questions and prompts to assess the participants’ experience of CM. The prompts explored CM from the participant’s perspective. The 20 semi structured interviews lasted between 28 and 60 minutes with a mean duration of 39:3 minutes (SD = 11.5). The interviews were conducted by a master-level female medical student (LS) and a master-level female psychologist (MG) over a period of 7 months, from January to July 2020. The study team conducted interviews until data saturation was obtained.
Analysis Plan
Interviews were conducted in French and audio recorded, transcribed verbatim and stripped of identifying information before analysis. Data were analyzed with a conventional content method 17 in an inductive way. 18 Two female researchers (MG, master-level psychologist and LS, master-level medical student) conducted the initial coding independently. Both researchers met to merge their codes and create a codebook that would include the common codes; idiosyncratic or redundant codes were grouped or removed. A third senior female researcher (VG, psychologist, PhD-level senior researcher) tested out the codebook by coding independently 2 interviews, and the codebook was adapted according to her feedback. Two researchers (master-level psychologist and master-level medical student) double-coded 10% of the interviews independently with the final codebook; any discrepancies were addressed until a consensus was found. This process was conducted until obtaining an adequate intercoder concordance of more than 80%. 19 A single coder (master-level medical student) independently coded the remaining interviews and explored the overreaching themes. The software used was Atlas.ti version 9 (ATLAS.ti Scientific Software Development GmbH).
Results
Five themes emerged from the inductive analysis and were similar through the different sites. To ensure clarity, we organized the themes in 2 parts, including positive and negative perspectives about CM. Among the positive perceptions, 3 themes emerged: (1) participants appreciated the fact that CM covered a large range of topics during the CM; (2) participants identified the quality of the relationship with the cm and the global evaluation as main differences with usual care; (3) benefits and outcomes of CM compared with usual care: gain in motivation, improved health literacy, and improved interactions with the healthcare system. Among the negative perceptions, 2 themes emerged: (1) participants reported CM’s negative aspects such as few perceived benefits of the program and a sense of stigmatization; (2) participants reported CM’s obstacles such as uncertainty around the CM’s objectives, covid-19, and cm’s lack of time
Participants Appreciated the Fact That CM Covered a Large Range of Topics During the CM
General opinion
Most participants had a positive opinion of the CM program. Participant 17 disclosed: “I would not change anything. I am seeing only good out of it.”
Topics covered
FUED overall perceived the CM’s content as comprehensive. The topic they responded to most frequently was mental health. When asked about the aim of CM, participant 5 answered: “To stop my panic attacks.” Participants commonly described having discussed their experience in healthcare: “The hospitalizations, what they were doing in the hospital.” (Participant 2) When asked about their goals when attending appointments, participants frequently answered that they wanted to reduce their ED visits: “To find a solution for me so that I don’t come back all the time to the ED.” (Participant 6).
Physical health was also a common theme. Participant 14 disclosed: “I did not know [. . .] that [this] pain could be similar to angina.” Participants also covered broader aspects of their lives, such as their relationships (“I have also talked about my romantic relationships.” (Participant 3)); daily activities (“They [cm] asked me if I went out of the house.” (Participant 17)); financial issues (“He [cm] gave me phone numbers, like social welfare.” (Participant 5)); and substance abuse (“The aim: stop smoking cannabis.” (Participant 3)).
Participants Identified the Quality of the Relationship With the cm and the Global Evaluation as Main Differences With Usual Care
Compared with usual care, participants valued the cm’s global evaluation of their case: “They [cm] are healthcare professionals but they want to know beyond my illness, how I live things.” (Participant 17).
Participants noted a difference in the quality of their relationship with the cm. Interestingly, previous encounters with healthcare professionals were described as negative among most participants. Nearly all participants brought up the importance of being heard (“They [cm] were human, professionals. They were listening to me!” (Participant 17)) and taken seriously (“They [cm] saw that this was not in my head, and they told me that clearly.” (Participant 2)).
Benefit and Outcomes of CM Compared With Usual Care: Gain in Motivation, Improved Health Literacy, and Improved Interactions With the Healthcare System
Moral support as main benefit
When asked about the most beneficial aspect of CM, almost all participants answered moral support. “I felt supported, and it was useful for me.” (Participant 2).
Gain in motivation
Participants commonly expressed how CM helped them feel more motivated: “Well, it helped me in a way that I felt more secure, I could progressively get out of my house.” (Participant 17).
This gain in motivation was also related to participants’ health. Participant 3 described how the cm helped him/her: “To persevere, to take the first step to call my therapist, to book an appointment, to show up.” Participant 20 explained that this motivation came from the fact that somebody cared about him/her: “Well, now there is someone who cares about my pain and so I will try to get better.”
Improved health literacy
Some participants reported that CM helped them better identify symptoms requiring urgent care. “They set me limits, there I have to go, not go.” (Participant 15). For some participants, the cm helped them gain a finer understanding of their illness: “It is just to be on the same page about the different illnesses we have.” (Participant 18).
Furthermore, some participants highlighted the fact that the cm guided them in their navigation through the healthcare system, referring them to practitioners and finding alternatives to ED as a source of care: “Because [. . .] when we have a big problem, what do we think? ED! [. . .] Because we don’t know all the little crossroads that we can take rather than going straight forward to the ED.” (Participant 10).
Improved interactions within the healthcare system
For some FUED, the cm was perceived as an ally within the healthcare system: “[the cm] proved to me that there still are some people on the medical side that really cared about the patient.” (Participant 20). Interestingly, participants reported that they had developed a protocol of care in collaboration with their respective ED thanks to the cm. Participant 1 explained: “When I come to the admission of the ED, they know me, I say: ‘There is that protocol’ and then it is transmitted to the nurses.”
A participant also reported perceiving the cm as being a bridge to communicate with the hospital team: “I think the information I gave her [cm], she must have put it in my file and let the staff know.” (Participant 4).
In general, participants reported feeling less fearful about the healthcare system since benefiting from CM: “Before, when I had to go [to the ED] I had this pain, it made me anxious! I did not want to go, but now, ever since there is that protocol, I don’t have this anxiety anymore.” (Participant 13).
Participants Reporting CM’s Negative Aspects Such as Few Perceived Benefits of the Program and a Sense of Stigmatization
For some participants, the outcomes were neither obvious nor concrete enough: “After all, I was expecting that someone would study my case more and not only that [the cm] suggests me to make an appointment with a psychiatrist” (Participant 6). A few participants felt that the CM program was of no use to them: “Well, in the long run I can tell you honestly that this is not useful.” (Participant 7).
Although rarer, a few participants explained that they experienced untoward consequences of CM, such as a sense of stigmatization for having been included in the program: “Well, now the few times I go to the ED, I feel even worse than before [. . .]. I am apologizing [. . .] to have had come to the ED for so little.” (Participant 8). Some participants explained that they felt judged by the offer to enroll in the parent study and that the reason they felt they were being followed up was to prevent them from going back to the ED: “I didn’t dare to go back to the ED. I was thinking—Well now I have been red-flagged.” (Participant 15).
Participants Reporting CM’s Obstacles Such as Uncertainty Around the CM’s Objectives, Covid-19, and cm’s Lack of Time
A common obstacle brought up by participants was confusion around the CM program’s objectives and organization. Participant 16 explained: “Because we covered all the themes, it became confused in my mind.”
The CM program was also impacted by the COVID-19 pandemic. The cm had to integrate measures such as social distancing and contact the participants by telephone instead of seeing them in person: “I think that human contact [. . .] is still better than talking over the phone.” (Participant 18).
Lack of time from the part of the cm was also pointed out as a disadvantage: “I would have appreciated to have more time.” (Participant 5).
Discussion
This study explored FUED’s perspectives on CM in hospitals across the French-speaking part of Switzerland. Our main findings were that most participants endorsed the CM program mainly because of the working relationship they were able to establish with the cm. The latter was considered as key to the success of the CM program and resulted in participants’ increased motivation, as well as improved interactions with the healthcare system and improved health literacy. Negative aspects of CM were also identified, including the sense of stigmatization that some patients felt for having been chosen for the study, and also a lack of clear explanations on the actual aim of CM. Barriers to CM were also identified such as confusion around the CM’s objectives and organization, COVID-19′s impact on CM’s organization and cm’s lack of time.
These findings corroborate results from previous studies in this population, suggesting that the therapeutic alliance created between the cm and FUED is a major component of success of CM programs, and that the positive working relationship established with cm can motivate FUED to change their perception and use of the healthcare system (eg, improved navigation in the healthcare system).8-12 These findings are consistent with one of the founders of the humanistic approach in psychology, Rogers, 20 who believed that patients are experts to themselves and therefore are able to change provided they are given the possibility to actively engage in the process of their treatment.
Moreover, our study emphasized the knowledge that participants’ overall healthcare literacy can be improved through CM, leading to improved navigation skills across the healthcare system. These findings also helped to increase our own understanding of the mechanisms that drive a successful CM program.
Untoward consequences of CM were also reported. For example, this study is, to the best of our knowledge, first to document how some FUED felt stigmatized for having been included in such a program. Furthermore, some participants failed to see the benefits of CM, which may suggest that approach is still not the panacea for all FUED. This study identified a number of barriers to the successful rollout of the CM program which, taken together, could be addressed as follows: (1) always maintaining a non-judgmental attitude toward FUED, keeping in mind the importance of building a relationship of trust between FUED and healthcare professionals; (2) ensuring that patients participating in a CM program have a clear understanding of how and why the program can benefit them to reduce confusion and avoid misconceptions about CM; and (3) providing cm with more time and resources to carry out their work.
Limitations
First, our results showed an overrepresentation of female responders (75% (Table 3)), whereas most studies have shown a slight tendency toward male preponderance in this patient population.21,22 Second, we cannot exclude desirability bias, although both positive and negative perceptions of the CM program were reported by participants. Third, our study ran during the COVID-19 pandemic, likely impacting participants’ perception of CM (for instance, participants reported missing the one-to-one encounters). However, all participants started the intervention before the pandemic and for some, the intervention was over by the time lockdown measures were implemented, thereby limiting the extent to which this aspect may have weighed on outcomes. Furthermore, we added lack of follow-up in the CM (ie, lack of regular attendance to the CM’s appointments) as an exclusion criterion because, consistent with the qualitative inquiry, we aimed to recruit participants with a strong experience of CM to increase the validity of the investigation. We cannot exclude a participation bias, although participants did mention both positive and negative aspects, thereby increasing our confidence regarding this risk. Finally, most of the participants included in this study were recruited in peripheral hospitals. Although it is possible that the experience of CM differs between peripheral hospitals comparing to university hospital, the findings reported by the participant included from the university hospital aligned with those yielded in the peripheral hospitals.
Conclusion
Our study was the first to evaluate CM from the FUED’s perspective on a large scale of hospitals across Switzerland. Results confirmed that FUED can gain trust and knowledge in the healthcare system through personalized follow-up. New aspects emerged, such as a sense of being stigmatized by some participants from being included in CM. Future quantitative research is required to evaluate whether the perceived outcomes identified by FUED corroborate the association made between CM, QoL and reduced ED visits.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Swiss National Fund for Scientific Research (grant number: 407440_167341).
Ethics
All procedures were approved by the Swiss Ethics Committee on research involving humans in the Canton de Vaud (project number: 2018-0042).