
Abstract
In recent years, the number of students enrolling in universities for higher education has increased, and these students are more diverse than ever before. Moreover, the number of students with disabilities in higher educational institutions is also increasing. Therefore, their support needs are becoming more diverse and specialized. To examine how best to provide support to students who are unable to locate it, this study conducted a survey in which details were collected from students who were involved with university student support organizations, analyze the relationship between subjective adjustment and objective adjustment, and examine the trends in subjective quality of life (QOL). In total, 156 university students (age: mean = 22.14, standard deviation = 2.86, range = 18-7) were surveyed between April 2018 and March 2020. The Japanese version of the World Health Organization Quality of Life, Brief Version, was used to analyze trends in subjective QOL. The average QOL of students who were less likely to receive support was lower than that of the general population. The results also indicated that QOL decreased as the level of disability and health status increased. Furthermore, the results of the analysis of the relationship between the overall domain QOL and the domain-specific QOL suggested that the psychological and environmental domains contributed the most to the overall QOL. Accordingly, students at universities require assistance in a number of areas. Furthermore, it is essential to adjust the content and combination of support according to the objective level of adjustment.
Focusing on quality of life is important in assisting people with illnesses and disabilities.
We believe that our study makes a significant contribution to the literature because it examines the adaptation of students for whom obtaining support or connecting to support is difficult.
In this study, the World Health Organization’s Quality of Life Rating Scale was used to examine the adjustment of students who have difficulty connecting with support. Moreover, we also observed differences in the support needed for each the level of disability and health status.
Background
In recent years, the rate of enrollment at Japanese universities has increased, 1 and students from diverse backgrounds have enrolled at universities across the country. Furthermore, there is an increase in the number of students with disabilities in higher education institutions, especially those with developmental and mental health disorders, and the support needs of students are diversifying and becoming more specialized. 1 The Convention on the Rights of Persons with Disabilities was adopted by the United Nations in 2006, and in Japan, the obligation to provide reasonable accommodation was indicated in a law that came into effect in 2016. According to the convention, “reasonable accommodation means necessary and appropriate modification and adjustments not imposing a disproportionate or undue burden, where needed in a particular case, to ensure to persons with disabilities the enjoyment or exercise on an equal basis with others of all human rights and fundamental freedoms.” 2
Even in the US, where reasonable accommodation for students with disabilities was introduced earlier than in Japan, the number of students with developmental and mental health disorders is increasing significantly. 3 Wolf 3 states that students with developmental and mental health disorders face various difficulties after enrollment. Consequently, it is important that they are able to easily access on-campus support centers and receive effective assistance. Additionally, research in a Japanese context has demonstrated that difficulty adapting to changes in an environment and diminished motivation to study may result in poor academic performance and dropout among students from diverse backgrounds. 4
Since the enforcement of the Disability Discrimination Elimination Law in Japan, 5 the understanding and awareness of disabilities and necessary accommodations for students at universities across the country has increased. According to the National Survey conducted by the Japan Student Services Organization, 1.17% of Japanese higher education institutions had students with disabilities in FY 2019. 1 A significant difference was also found between the number of students with disabilities who enrolled at higher education institutions and those who graduated from those institutes. The number of students enrolled in the final year of a program at a higher education institution in 2019 was 5956. However, only 4203 of these students graduated. It is possible that this discrepancy is due to learning problems faced by students, such as difficulties associated with social transition and credit acquisition. Compared with the percentage of students with disabilities enrolled, the percentage of students with disabilities who receive reasonable accommodations is low. 1 Moreover, career support for students with disabilities is lacking compared with those without disabilities. 6
Among students with disabilities, the graduation rate of students with comorbid developmental and mental health disorders is remarkably low. 1 For example, in the US, the graduation rate of students without disabilities is 51.2%, whereas that of those with autism spectrum disorders is 38.8%. 6 Therefore, understanding the level of adaptation of students with developmental and mental health disorders and supporting these students is crucial.
The World Health Organization Quality of Life (WHOQOL) is an international quality-of-life assessment instrument. The World Health Organization describes quality of life (QOL) as an “individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns.” 7 The WHOQOL has been developed and standardized to enable all individuals to measure “subjective evaluation that is embedded in a cultural, social, and environmental context” in terms of physical and psychological wellbeing, level of independence, social relationships, beliefs, and living environment. 8 The WHOQOL is used to assess the QOL of university students, including those with disabilities, in Japan and overseas.9,10 Studies have reported a lower QOL in students with developmental disorders than in those without disorders.9,11,12 Among students with psychiatric disorders, those with eating disorders tend to have a lower QOL, 13 and those with mood disorders have a lower QOL in terms of physical health, psychological health, social relationships, and environment. 14
Moreover, it has been found that feelings of anxiety and sadness affect QOL. 15 Based on survey data from a sample of 286 students, a multiple regression analysis was carried out using relevant items from the World Health Organization Quality of Life, Brief Version (WHOQOL-BREF) questionnaire to assess satisfaction with health and QOL. The results of the analysis revealed that perceived support for the basic psychological needs of autonomy, competence, and relatedness significantly predicted satisfaction with health and QOL among students. 16 Coutinho et al 17 investigated the QOL of 347 college students, including those with mental health disorders, and applied structural equation modeling to determine the impact of mental health disorders on QOL. The findings reported higher levels of anxiety and experiential avoidance and lower QOL in students with chronic illness than in those without disabilities. Furthermore, an association between anxiety and psychological QOL was revealed. 17 Thus, providing treatment for anxiety and psychological support are important for improving QOL.
A subjective aspect of QOL is subjective well-being, 18 which is divided into 2 domains: cognitive and affective. 19 Moreover, 2 studies conducted on university and junior college students 20 and on students with disabilities, respectively 21 revealed a correlation between subjective well-being and self-esteem, suggesting that enhancing students’ self-esteem may improve their subjective QOL.
Several studies also point to the importance of social factors, such as belonging and self-advocacy, in any assessment of QOL. For instance, Fleming et al 22 state that a sense of belonging and self-advocacy are important for college adaptation. Fredette et al 23 demonstrate the importance of support structures and services. These studies highlight the need to focus on psychological and social factors in the assessment of QOL. It is important to understand the unique needs of students to develop appropriate interventions to facilitate their adjustment to college. However, no study has investigated the adaptation of students who are in need of support.
To determine how best to provide support for students with difficulty connecting with support, it is necessary to accumulate information on the actual conditions of students in maladjusted states. It is the objective of this study to examine subjective QOL as one of the information sources on the actual conditions of students who find it difficult to access support services. The subjective perception of various domains by university students influences their mental and physical functioning and behaviors regardless of the presence or absence of disabilities or diseases, as demonstrated by previous studies.24,25
This study aimed to conduct a questionnaire survey of university students connected to student support services to determine how support can be provided to students who have difficulty connecting with support. Moreover, the relationship between disability level, health status, and subjective QOL will be clarified. We hypothesize that students who have difficulty connecting with support will have lower QOL than the general population of the same age group. Additionally, we hypothesize that QOL would decline as disability and health status deteriorates.
Methods
Sample
Students who had difficulty accessing support organizations within and outside the university were operationally defined as “students who find it difficult to connect with support.” The participants in the study were “students who are in need of support,” including those who had taken a leave of absence or dropped out. We expected that these students would have difficulties in various aspects of their lives, such as overall health, interpersonal relationships, and study and career choices.
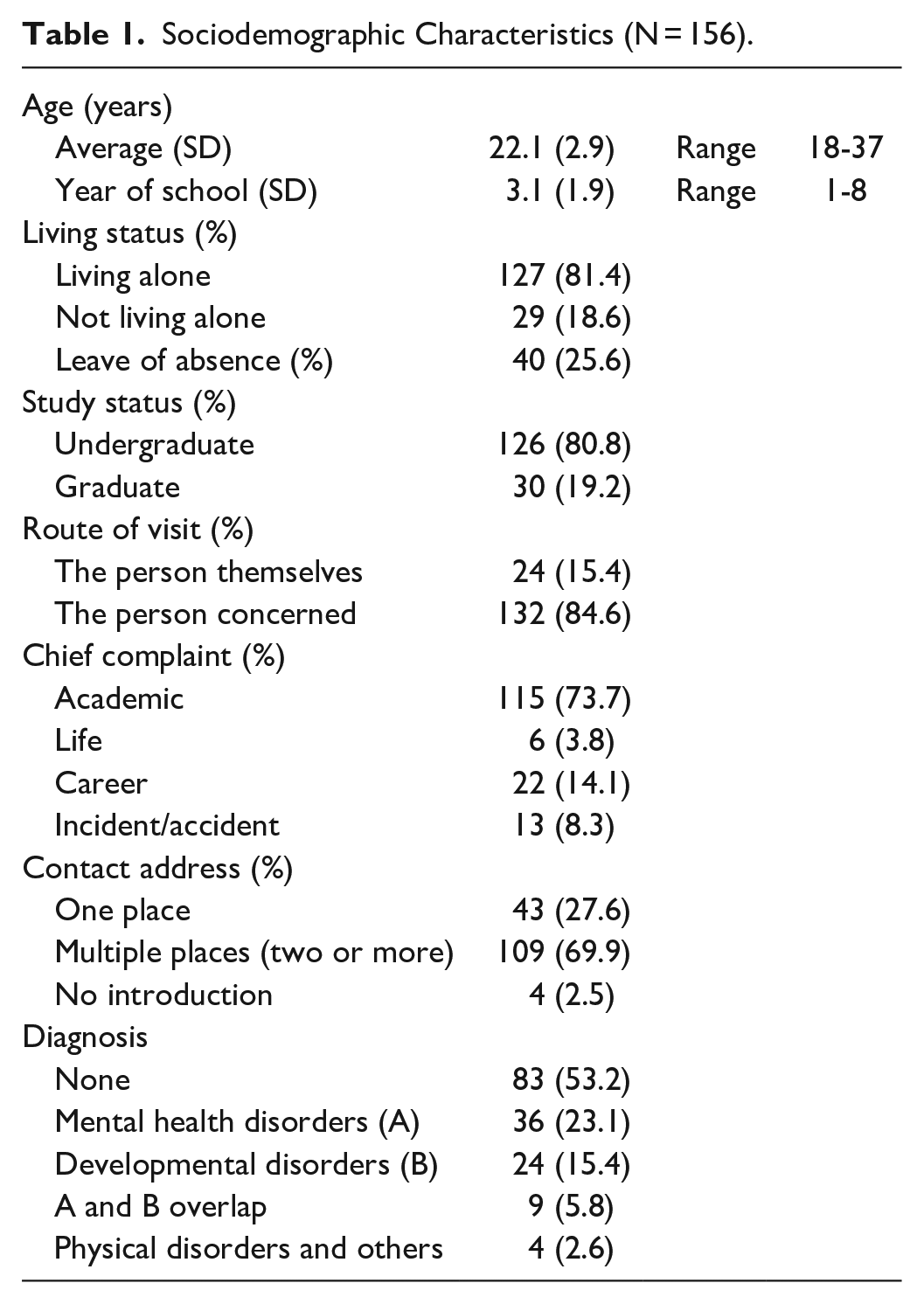
The recruited sample consisted of 156 university students, including those with and without disabilities (age: mean = 22.14 years, standard deviation = 2.86, range = 18-37 years) who consulted the staff at the Center for Health Sciences and Counseling (CHC), Coordination Section (CS), Kyushu University, Fukuoka, Japan, between April 2018 and March 2020. Kyushu University is a university with approximately 11 600 undergraduate students and 7000 graduate students, totaling about 1860 students. The CS mainly supports (1) those who have difficulty in coming to the CHC on their own initiative, (2) those whose support needs are unclear, and (3) those who do not know where to find the appropriate support for their needs.
The participants had visited the CS for various reasons (eg, concerns relating to mental health, academic and professional careers, adjusting to college life, communicating with others, financial matters, and suicidal ideation). The consultants also provide consultation to other students, parents, and faculty members (Table 1). An additional sample of 307 individuals aged 20 to 29 years (of the 2007 members of the general population sampled) was included and used as a control group. 26
Sociodemographic Characteristics (N = 156).
Assessment QOL
The WHO, with the aid of 40 collaborating centers around the world, has developed 2 self-administered instruments for measuring QOL—WHOQOL-100 and WHOQOL-BREF—that can be used in various cultural settings, while allowing the results from different populations and countries to be compared. 26 The WHOQOL-100 assessment was developed by the WHOQOL Group in 15 international field centers simultaneously to develop a QOL assessment tool that could be applicable cross-culturally. 16 We used the Japanese version of the WHOQOL-BREF—WHOQOL-26, a 26-item quality-of-life assessment form based on the WHOQOL100—to assess the self-perceived QOL of participants. 26 The WHOQOL-BREF comprises 24 items classified into 4 domains (physical health, psychological health, social relationships, and environment), and 2 items about WHOQOL as a whole. Each item is assessed on a 5-point scale (1 = very poor; 2 = poor; 3 = neither poor nor good; 4 = good; 5 = very good). According to the WHOQOL, the physical health domain refers to the ability to carry out daily activities. The WHOQOL domain of psychological health asks about self-concept, and the WHOQOL domain of social relationships asks about satisfaction with relationships with others, as well as perception of support from others. In the environmental domain, questions are asked about the living environment and the availability of support services.
The 36-item World Health Organization Disability Assessment Schedule II (WHODAS 2.0) was administered to participants for measuring disability and health status across 6 functioning domains over 30 days. The item-response theory-based scoring was used, 27 and each domain score was calculated by adding the item responses, ranging from 1 (“no difficulty”) to 5 (“extreme difficulty/cannot do”). A summary score (overall disability) was also determined from all items. The summary and domain scores were transformed into 0 (best) to 100 (worst). Additionally, these scores were classified into 3 categories according to level of disability and health status: severe, moderate, and mild. The disability scores were arranged in descending order, with the top 33 percentile defined as severe, the next 34 percentile defined as moderate, and the remaining 33 percentile defined as mild.
Procedure
The study was conducted at the CS of the CHC, Kyushu University, Japan. Participants were students aged 18 to 37 years who visited the center over a period of 2 years (between April 2018 and March 2020). Following the end of each consultation, the aforementioned 2 instruments for measuring QOL were provided to students by the authors. Demographic data included the following: age, year of school, living status, leave of absence, undergraduate or graduate, route of visit, contact address, complaint, and diagnosis. A completed consent form was also obtained. Data from the demographic questionnaire were only used to determine the characteristics of participants. All procedures were performed in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Research Ethics Committee of Kyushu University (No. 202003).
Data Analysis
First, the QOL domain scores for the participants in the study were compared with those of members of the Japanese population obtained using stratified sampling methods (N = 307; 154 men, 152 women, one person with gender dysphoria; age range 20-29 years). 26 The difference in the mean value of the QOL, ES, and confidence interval between the CS user and control groups was compared using Student’s t-test. Second, a multivariate analysis of variance was conducted using QOL, with domain as the dependent variable, and disability level (classified into 3 groups based on WHODAS 2.0 conversion scores: severe, moderate, and mild) as the independent variable. Third, Pearson’s correlation analysis was used to assess the correlation between QOL by domain. Multiple regression analysis (forced imputation method) was conducted to examine the influence of domain-specific QOL on overall QOL. A P-value of <.05 was considered to indicate statistical significance. Statistical analysis was performed using SPSS version 25.0 (SPSS Inc., Chicago, USA).
No statistical sample size calculations were conducted. Because, for backward-looking research. However, we have confirmed the detection post hoc powers. post hoc powers of 100% to detect differences in mean of Overall average (0.32), Physical health (0.86), Psychological health (0.42), Social relationships (0.05), and Environment (0.18), respectively, for QOL score, assuming a common SD of 47%, using a two-group t-test with a two-sided significance level of P < .05 for between CS users and control group.
Results
The QOL domain scores for the participants in the recruited and control groups were compared using stratified sampling methods. The minimum and maximum mean values of the 5 domain categories of the WHOQOL-26 (“total,” “physical health,” “psychological health,” “social relationships,” and “environment”) evaluated by the CS users were 2.58 and 3.36, respectively (Table 2). By contrast, for the control group aged 20 to 29 years, the minimum and maximum mean values were 3.17 and 3.44, respectively. A slight difference was observed by gender. 26
Comparison of QOL Values Between CS Users (N = 156) and Individuals in the Control Group (N = 307).
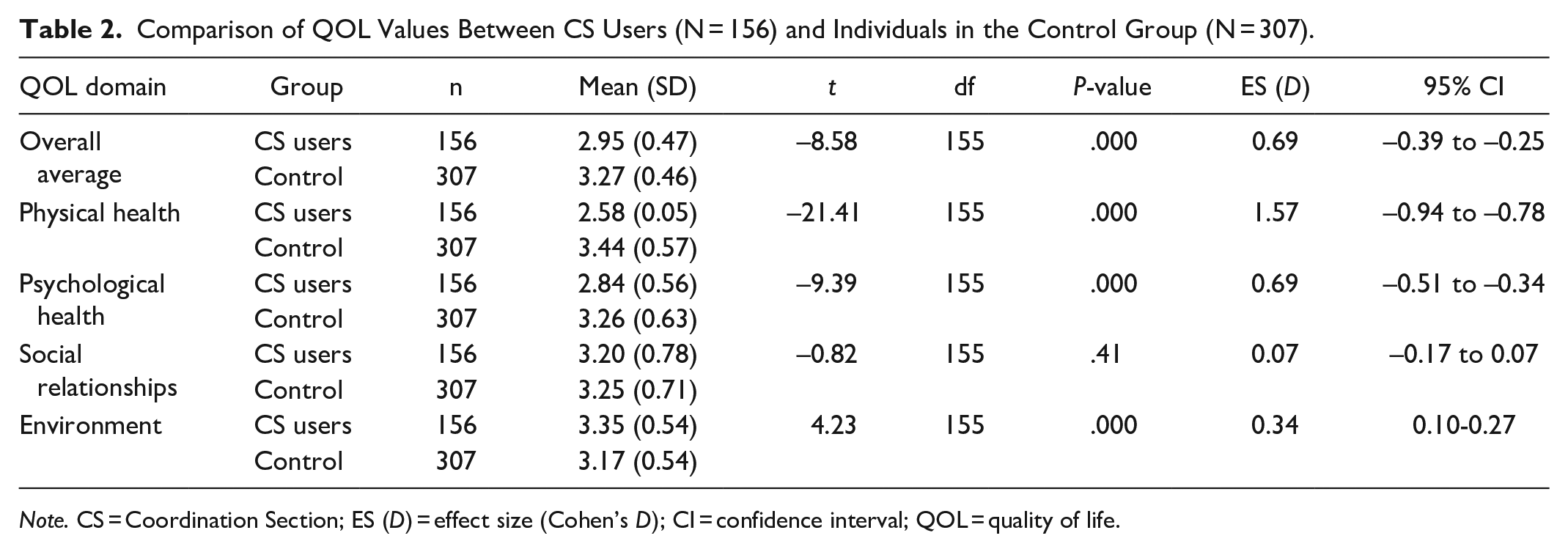
Note. CS = Coordination Section; ES (D) = effect size (Cohen’s D); CI = confidence interval; QOL = quality of life.
According to the t-test, if the ES is <0.20, there is no effect; if it ranges from 0.20 to 0.50, it is small; if it ranges from 0.50 to 0.80, it is medium; and if it is ≥0.80, it is large. 28 The results revealed that the scores for the total, physical health, and psychological health domains were significantly lower in the CS user group than in the control group (P < .000). However, the environmental scores of the CS users were significantly higher (P < .000) than those for the control group. The ES analysis revealed a difference between the QOL values of the CS users and members of the control group with respect to the total, physical health, psychological health, and environmental scores (total: ES [Cohen’s D: referred to as d] = 0.69; physical: ES (d) = 1.57; psychological: ES (d) = 0.69; environmental: ES (d) = 0.34).
As noted earlier, 3 categories were established according to the level of disability using total WHODAS 2.0 scores, and the QOL in each domain was compared using a multivariate analysis of variance (Table 3). Students with severe disabilities were found to have particularly poor social relationships.
Comparison Between QOL Domain Value and Level of Disability (N = 156).

Note. QOL = quality of life.
P < .05.
The correlation between QOL domains was also examined using the Pearson’s correlation analysis. Moreover, we found a highly significant correlation between the scores of each QOL domain (Table 4).
Correlation Between QOL Domains (N = 156).

Note. QOL = quality of life.
P < .001.
Finally, a multivariate analysis was performed with overall QOL scores as the dependent variable, and the 4 domains as the independent variables. Multiple regression analysis using the forced entry method revealed that the psychological health and environmental domains have a positive and significant influence on overall QOL. Conversely, the physical health and social relationships domains were found to have no statistically significant influence on overall QOL.
The goodness of fit of the multiple regression model in this study was significant at the 1% level (F(4, 151) = 33.38, P < .01), suggesting no multicollinearity problem (VFI value: 1.57-2.02).
The results of correlation analysis and multiple regression analysis suggest that the correlations found between overall QOL and the domains of physical health and social relationships may be pseudo-correlations. Therefore, we calculated partial correlation coefficients between overall QOL and the domains of physical health and social relationships using the psychological and environmental domains as control variables. The results showed no statistically significant correlation between overall QOL and these domains (physical domain: r = .095, n.s.; social relationships domain: r = .033, n.s.). Based on these results, the psychological health and the environmental domains contribute substantially to the overall QOL of students who are less likely to have access to support. The correlations found between overall QOL and the physical health and social environment domains were shown to be pseudo-correlations with the psychological health and environment domains as control variables (Table 5).
Multiple Regression Analysis Between QOL Domains and Overall QOL (N = 156).

Note. QOL = quality of life.
P < .001.
Discussion
We conducted a study to assess the subjective QOL of university students who utilize the CS, which serves as a coordination function within the university. We analyzed the relationship between the average subjective QOL, disability level, and subjective QOL domain, as well as the overall subjective QOL and each domain. The difference in average QOL values showed that students with difficulty obtaining support have a lower average QOL value than the general population of the control group. By contrast, the average QOL value for the environmental domain was higher for these students than for the control group, but the ES was smaller.
The results of this study suggest that the subjective QOL of students who have difficulty obtaining support is low in all areas of life. This is consistent with previous studies that have found that people who abandon/give up coping behaviors when faced with situations that make it difficult for them to adapt to academic, personal, and social life tend to experience low QOL. 29 This may suggest that difficulty obtaining support may lead to an inability to cope. Moreover, it is important for university student support centers not only to wait for the students themselves to offer support, but also to frequently approach them from the supporters’ side.
By analyzing the relationship between disability level and all domains of subjective QOL, a statistically significant association was found between the subjective QOL and disability level for all 3 categories (mild, moderate, and severe). It was revealed that the QOL for the domains of physical and psychological health was significantly lower in the severe and moderate disability groups than in the mild disability group. This suggests that students have an accurate understanding of their own disability and health status. Subsequently, in the domain of social relationships, the QOL scores were lower in the severe disability group than in the moderate and mild disability groups. This indicates that students with disabilities are often unable to connect with the people around them. Finally, a significant difference was observed between each of the 3 disability categories in terms of environmental domain scores and overall QOL. It was considered that the degree of impairment for students in each of the disability categories might be associated with the perceived suitability of the surrounding environment.
In a previous study that assessed the QOL of university students with developmental disabilities, 10 we found that they were highly depressed and anxious and had a low subjective QOL. Notably, although the results of this study were not exclusively based on students with developmental disabilities, they are common in that they are students who find themselves in a disabling situation. The results support the findings of Watanabe et al. 10 All aspects of a student’s life are expected to be negatively affected by their disability and health status. In particular, if the disability status is more pronounced, this suggests a greater impact on the student’s interactions with their surroundings and life in general.
Based on our results, considering the best method or approach for intervention according to the nature and severity of the disability is critical. For instance, if impairments are recognized in the physical and psychological domains of the group with moderate disabilities, professional support should be provided to address the physical and psychological concerns of these students. In addition to these issues, it is suggested that maladaptation in the domains of social relationships and environment worsens with the degree of disability. Thus, students should be provided with appropriate support and reasonable accommodations.
In the environmental domain, the WHOQOL includes access to professional support and ease of living (housing, transportation, leisure, and others). 26 Our results show that students with severe disabilities have considerably little interaction with other people and find it difficult to receive support from those around them. It is assumed that such students are unable to act spontaneously, and there are at risk of becoming socially isolated. Therefore, it is necessary for teachers and parents to cooperate and assess their living conditions. Based on these facts, it is vital for them to collaborate and provide support intervention according to the ability of these students. In addition, based on the findings of a report by Van Hees et al, 30 combining multiple types of support for the students with disabilities is critical to enable them to succeed in various fields, such as academics, school life, and daily life, and to increase their satisfaction level. Moreover, the university would be required to perform a coordinating function in building a multi-layered support system.
An analysis of the relationship between overall QOL and domain-specific QOL scores revealed that the domains that affected the overall QOL of students with disabilities the most were the psychological and environmental domains. Overall QOL for the general population was found to be related to QOL in all domains. 26 The results obtained for the general population differ from those of a previous study, 31 and the current study provides new findings in this regard.
The psychological domain of the WHOQOL includes questions relating to perceptions of body image, emotions, self-value, and beliefs. In previous studies, the psychological domain has also been considered to reflect self-concept. 31 Social comparison with others of a similar age has been found to play an important role in the self-concept formation of Japanese college students. 32 Accordingly, it is considered that they assess their own living conditions in relation to the living conditions of others of the same age. Therefore, professional psychological support is required for students to reconsider themselves in a broader and overall positive manner.
Finally, the environmental domain comprises items relating to aspects such as management of personal finances, safety, insurance, medical services, opportunities to acquire information and technology, leisure activities, and transportation.21,26 This environmental domain emphasizes the importance of providing professional help to students who experience difficulty obtaining help. Thus, it is important to offer advice and assistance to students with disabilities who are unsure of where to find professional assistance or how to connect with those who are concerned about their well-being. Moreover, it is vital that professional support be interrelated and empathetic. Since the combination and coordination of support is expected to be difficult, we believe that the involvement of a single point of contact for a variety of consultations is necessary as individual students have unique needs requiring tailored support.
The results of the multiple regression analysis did not yield significant Bae’s in the areas of physical health and social relationships. Future studies should elaborate on this finding by revising the model of QOL.
Conclusions
According to this study, the subjective QOL of students who have difficulty obtaining support is lower than that of the general population of the same age group. It was also suggested that the nature of support and intervention needed depends on the level of disability and health status. Finally, this study found that the subjective QOL of these students differs from that of the general population, highlighting the importance of psychological and environmental factors. These findings underscore the importance of providing multiple types of support for these students. It is also important to adjust the content and combination of support according to the level of disability and health status. To develop a multi-layered support system and enable various support functions to work together organically, adopting a broad and inclusive approach is crucial.
Furthermore, evaluating student support at Japanese universities from an international perspective is warranted. As the WHOQOL-26 rating scale is used internationally, the results can be compared and examined in a global context. Future research should focus on international contexts and comparisons.
Developing effective intervention programs is the subject of future research.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231159728 – Supplemental material for The Quality of Life of Students With Difficulties Accessing Support
Supplemental material, sj-docx-1-inq-10.1177_00469580231159728 for The Quality of Life of Students With Difficulties Accessing Support by Yusaku Omodaka and Takeshi Sato in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors thank the students who used/visited the Coordination Section at the Kyushu University Center for Health Sciences and Counseling for their support with the questionnaire.
Authors’ Contributions
YO designed the study, collected the data, performed statistical analysis, and drafted the manuscript. TS contributed to data interpretation and final manuscript preparation. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI under Grant Number JP21K13476. The funder had no role in the design of the study or collection, analysis, or interpretation of data, or in writing the manuscript.
Ethics Approval and Consent to Participate
The study was approved by the Research Ethics Committee of Kyushu University (No. 202003). Written informed consent for participation was obtained from the students.
Consent for Publication
The survey to evaluate student support was conducted with verbal consent. In addition, the opportunity to opt out was provided.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.