
Abstract
Cystic Fibrosis (CF) is a genetic disorder that primarily impacts the respiratory and gastrointestinal systems. With advances in treatment and medications, the life expectancy of people with CF is continuing to increase with current life expectancy at 47 years of age. Given the increased life expectancy, people with CF are interested in childbearing but may have CF specific fertility issues that should be addressed by their CF healthcare provider. Currently, these conversations are not occurring or are suboptimal. This study aimed to investigate the practices of cystic fibrosis (CF) healthcare providers regarding fertility and fertility preservation (FP) discussions among women with CF. This was a qualitative, descriptive study. Twenty CF healthcare providers were interviewed including nurses, nurse practitioners, social workers, and dieticians among other disciplines. The semi-structured interviews were audio-recorded, transcribed verbatim, and analyzed using thematic analysis. Four themes emerged from the provider interviews about their fertility and FP discussion practices: (1) Change over Time; (2) CF Team Provides Primary Care including Reproductive Health Care; (3) Patient Support and Advocacy; and (4) Barriers and Facilitators to FP Discussions. The results of this study demonstrate an opportunity for CF healthcare providers to deliver patient-centered care. However, CF providers need to be educated on fertility and FP options. Additionally, there is a need for a more standardized structure of care to address the reproductive health of women with CF. The findings from this study may also be useful to non-CF providers who deliver care to women whose chronic illnesses impact their reproductive health.
Keywords
Fertility preservation should be an option for women with cystic fibrosis.
Cystic fibrosis healthcare providers want patients to explore fertility preservation, but they currently feel ill-equipped to hold fertility preservation conversations.
Practice implications include clinics thinking through their processes to best support fertility preservation discussions through normalizing the conversations with patients and partnerships with OB/GYN services.
Introduction
Cystic fibrosis (CF) is the most common genetic disease among Caucasians, affecting 70 000 individuals worldwide. 1 Although CF has historically been known as a disease of childhood, with medical and technological advances, this is no longer the case. Over 50% of the CF population are adults, and the current median predicted survival age of a person with CF born today in the United States is 47 years old. 1 While CF is a multi-system disease, it primarily affects the lungs, and individuals with CF will require a lung transplant to prolong life and preserve quality of life during end-stage lung disease. 2
In 2018, 253 individuals with CF received a lung transplant. 1 After receiving a lung transplant, options for conceiving a biological child are constrained due to the necessity of immunosuppressant medications which have known teratogenic effects. 3 Prior research suggests that women with CF desire to achieve many of the same life milestones as their non-CF peers, including motherhood, and would like to discuss sexual and reproductive health topics with their CF providers.4,5 However, despite the known potential need for lung transplantation in the CF population and the desire of women with CF to become mothers, the timing, frequency, and content of conversations between these women and their CF care team related to fertility preservation (FP) or fertility in general is unknown. Fertility preservation is defined as “the process of saving or protecting eggs, sperm, or reproductive tissue so that a person can use them to have biological children in the future.” 6
In contrast, oncology patients have consistently received FP counseling as part of standard care for over 15 years. In 2006, clinical guidelines for cancer patients were established to assist healthcare providers in discussing FP within the oncology population. 7 Current recommendations suggest that providers discuss FP as early as possible after diagnosis and that providers should be prepared to refer patients to fertility specialists to further address FP options. 7 Despite known reproductive issues and potential need for lung transplant in both men and women with CF, no such guidelines exist for this population. 8 The purpose of this study was to explore CF healthcare providers practices regarding fertility and FP discussions among women with CF.
Methods
This study utilized a qualitative, descriptive design and included one-on-one interviews with CF providers who were recruited from adult CF clinics across the United States by calling the clinics listed on the CF Foundation webpage and emailing or faxing information about the study. Additionally, CF-specific professional groups shared study information on their listservs. Finally, some participants were recruited via snowball sampling. Providers who were interested in participating contacted the study staff where they were screened and verbal informed consent to participate was obtained. Providers included a physician (n = 1), nurses (n = 3), social workers (n = 5), genetic counselor (n = 1), nurse practitioners (n = 3), physician assistants (n = 1), pharmacists (n = 1), and dieticians (n = 5). A wide range of CF providers were chosen for inclusion in this study to obtain a broad perspective and be representative of the multi-disciplinary approach in delivering CF care.
The study received institutional review board approval prior to initiating the study. All semi-structured interviews were audio recorded and conducted either in person or via the telephone. Table 1 contains key questions from the interview guide. Interviews lasted an average of 37 minutes, and participants were compensated $20 for their time.
Key Questions From the Interview Guide.

Analysis
Twenty participants were interviewed. Data collection was completed when data saturation was reached, and no new themes emerged from the interviews. Interviews were transcribed verbatim in English by a transcription service, coded using NVivo 12 software, and analyzed via the thematic analysis process outlined by Nowell et al 9 to ensure trustworthiness of the results. Multiple steps occurred during the analysis, with major procedures described below. First, the authors familiarized themselves with the data by both conducting the interviews (CC and SL) and reading the transcripts (all authors). Author 1 (JC) and author 2 (CC) coded the transcripts independently to generate codes and themes, then subsequently met and discussed the coding structure, coming to agreement on any points of conflict with the last author (SL) who confirmed the coding structure and resulting themes.
Results
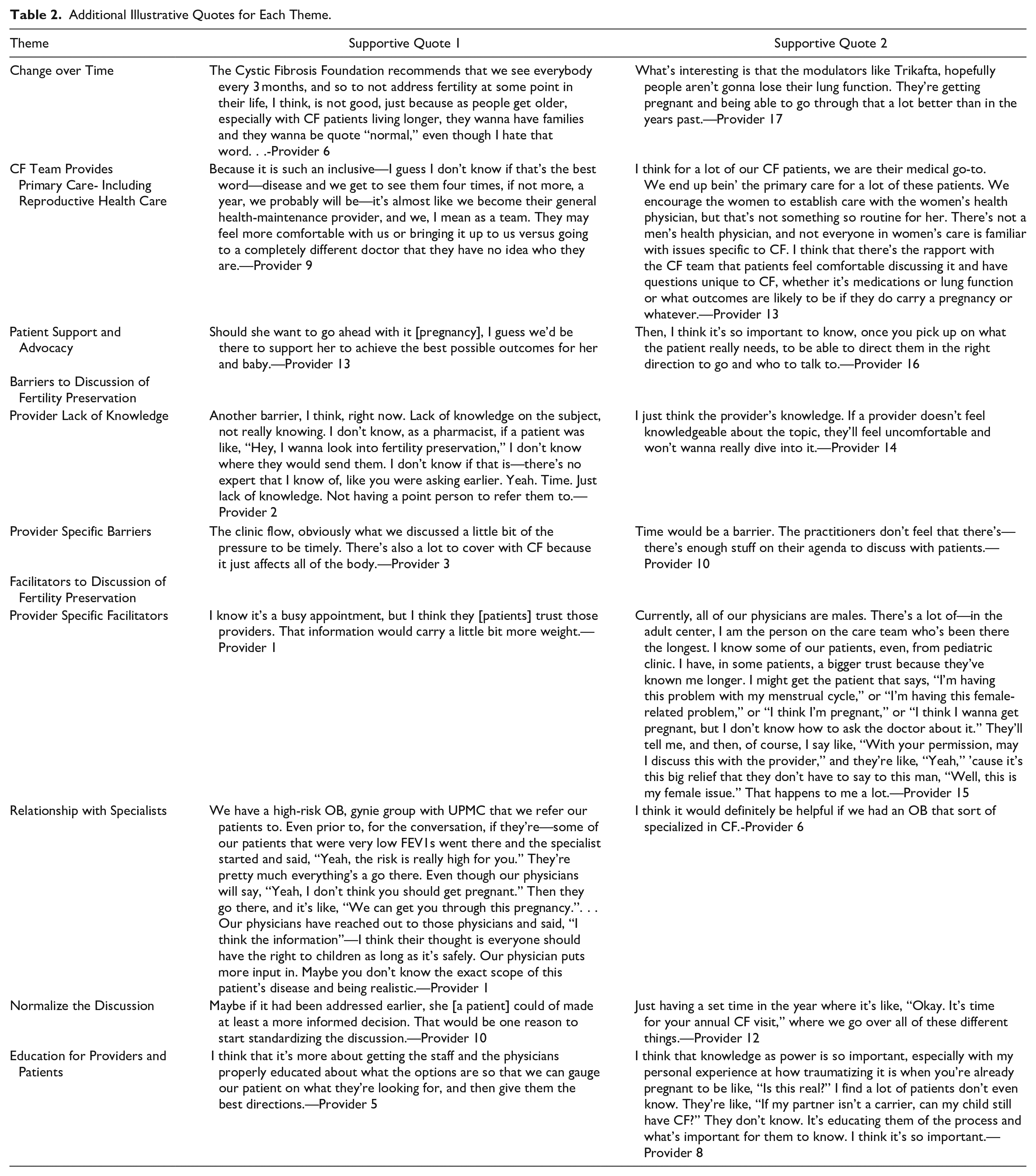
Four themes emerged from the analysis: (1) Change over Time; (2) CF Team Provides Primary Care including Reproductive Health Care; (3) Patient Support and Advocacy; and (4) Barriers and Facilitators to Discussion of FP topics. Each of these themes are discussed in detail below. Table 2 contains additional supporting quotes for each theme.
Additional Illustrative Quotes for Each Theme.
Change Over Time
Providers had either personally seen or were aware of major changes in the CF health trajectory due to advances in medicine and technology. Provider 4 explained what they had seen over the course of their career, “Right now, we are in a different era, where we went from let’s present your [CF patient’s] lunch and your nutrition . . . Now . . . we’re thinking about fertility.” With this progress, providers recognized that the information and education they provide to patients had changed as well. Provider 19 spoke to the way education of families had changed, “I think 10, 15, 20 years ago, we were telling parents that their sons couldn’t have kids.” While providers acknowledged that treatment and fertility options had changed drastically, they felt there was a lack of information to guide patients to make informed decisions. Provider 18 explained, “I think the other thing that CF teams need to acknowledge . . . is that what we know about fertility with women and CF is outdated and not accurate anymore. As women live longer with higher lung function, their experience of pregnancy is gonna be really different than it was 15 years ago.”
Modulator baby boom
A subtheme of Change over Time was specifically the way modulators, new medications used to treat CF, have changed the outlook for patients and their ability to become a parent. Ten of the 20 providers reported an increase in pregnancies since modulators became a regular part of CF care. Some providers were excited for their patients to be able to experience the milestone of parenthood. Provider 2 stated, “So many Trikafta [CF precision medication] babies. It’s wonderful.” Additionally, Provider 5 noted, “With the genetic modifiers that have been coming out, we’ve actually had an increase in patients actually becoming pregnant. We have eight females in ‘19 that became pregnant, and I think seven delivered.” Providers suspected the increase in pregnancies was a direct result of highly effective modulators, especially the triple combination drug, elexacaftor/tezacaftor/ivacaftor (brand name Trikafta in the United States). Some providers believed that some women with CF viewed modulators as a kind of fertility enhancing medication, due to its apparent success in enabling pregnancies to occur. Provider 14 expounded on this, “We’ve [the clinic] had a pregnancy boom. We’ve also had a few people start Trikafta to get pregnant. We have now a few patients who are pregnant on Trikafta.”
CF Team Provides Primary Care Including Reproductive Health Care
Another theme that emerged was that the CF care team serves as the de-facto primary care providers for patients with CF, which means that they are being asked to address concerns related to reproductive health. Over half of the interviewed providers acknowledged that they served as the primary care providers to their patients. Provider 4 explained, “Essentially, we’re primary care physicians for our CF patients. Whether we want it or not, that’s how they [women with CF] see us.” Provider 15 explicated the necessity of speaking to more than just CF [lung and digestive] conditions because patients rely on the holistic care the CF care team provides: “So many of our patients treat the CF team, the CF doctor, as their primary care physician. We’re their primary medical team, and I think it’s prudent for us, because of that, to talk about the whole body.” CF care team members were dedicated to the service of their patients and wanted to provide knowledgeable, holistic care, including reproductive health care. These providers believed that they were the best equipped to deliver holistic care, perhaps even more so than a traditional primary care provider. Provider 2 pointed out that even when a patient has a primary care provider, the primary care providers will send patients back to the CF care team for consultation on certain issues: “These patients are coming to us for all kinds of issues, not just their lung function. . . . a primary care physician’s gonna refer them right back to us. We act as their PCP, and we do more than just lungs in a cystic fibrosis clinic.”
Patient Support and Advocacy
Many providers reported a desire to support and advocate for their patients. Part of this support included respect for their patient’s autonomy. “We have to allow them [patients] to make decisions, even if we don’t think that they’re good decisions,” said Provider 8. Providers wanted to provide resources and information to patients, although it may not be readily available, especially about the intersection of CF and fertility. Despite this fact, Provider 11 felt a responsibility to go further and help patients find what they need, “I’ve really tried to take on the role of helping them find the right resource.” Providers also felt that it was important to provide patient-centered care, acknowledging that each individual would be different and would have different personal desires and life goals. Provider 19 noted that supporting patients does not mean forcing them into one life trajectory, such as having children: “. . .but sometimes you feel like you’re putting social norms on them [patients with CF]. Like, “Oh, you’re 33 or 35. You should be thinking about kids.” I don’t wanna— force them to feel like they have to be thinking about kids if that’s not something that they want.”
Barriers and facilitators barrier-lack of knowledge
Providers overwhelmingly reported a lack of knowledge about CF-specific fertility issues and advanced reproductive options. This lack of knowledge resulted in feelings of discomfort when talking with patients about these topics or a need to let another health care provider be “in charge” of this discussion. Provider 3 stated: “I oftentimes might share . . . what I know generally about fertility, but then say, ‘Let me get you somebody who knows more that can talk to you and address that on a deeper level.” Provider 9 echoed the need to let discussions of fertility be addressed by another team member, as they did not feel like they had much knowledge about this area, “I like to tell my patients, ‘I guess I can talk about that [fertility] and keep you entertained until a real person that knows about it can come in here’.” Many providers felt that they personally should not be the ones to do in-depth discussions about fertility or FP options with their patients due to a lack of knowledge, but overall, they felt that the CF care team should initiate general discussions with patients and refer to fertility specialists as needed.
Barriers: Opinion, gender
Providers acknowledged that their own specific attributes, like their gender or opinion on reproduction, could prevent open and effective discussions about fertility or FP with patients. “Some of that, too, is due to the mindset of some of our senior physicians kinda feeling like it’s their place to decide whether or not a woman should try to have a child or not,” reported Provider 11. Some providers felt that they knew patients’ social situations well enough to be concerned if the patient wanted to pursue parenthood. Provider 15 expounded on this point: “Okay, so patients might feel judged if they [the patient] say, ‘I wanna have a baby,’ and actively trying to have a baby, but you [the provider] know their social situation. You’re like, ‘I don’t think you have a job, and you can barely take care of yourselves, and you bring a different boyfriend in here every week.’ Yes, I think people would judge patients for that.”
The judgment that patients perceive from their providers may discourage patients from being honest about their family planning goals with their CF care teams. Providers believed that this perceived judgment was a barrier to having quality, patient-centered discussions on fertility and reproductive options.
Another barrier includes a lack of comfort that patients sometimes feel in bringing up any sexual and reproductive health topic with a male provider. “I know that some of our female patients . . . might feel more comfortable bringing it up to me . . . but may not feel comfortable asking one of our male doctors about it,” stated Provider 5 who is female.
Provider 11 noted that it is not just an awkward female-male dynamic, but that it may be a male’s lack of understanding related to the biological need to have a child, “All of our pulmonologists are male. Sometimes I think they—. . . view it . . . like, ‘You have this chronic disease. Pregnancy takes a toll on your health. I just don’t think you should do it,’ and kind of shut the door at that . . . One [provider] in particular has a very strong feeling and will frankly tell women that they shouldn’t have children, shouldn’t try to get pregnant..”
Clinic limitations
A majority of providers reported some type of clinic-related barrier, usually time or space. In most CF clinics, patient appointments are lengthy, with several multidisciplinary providers seeing the patient during the visit. Providers felt that they needed to cover many topics, such as medications, treatments, and specific dietary or respiratory needs. These needs took precedence over talking about topics like fertility or family planning due to time constraints. Provider 2 stated, “Time. I hate saying that 'cause it sounds so callous, like, ‘We [CF team] don’t have time for that [FP or fertility],’ but, honestly, we are addressing so many things in clinic.” Not only can finding time to discuss fertility or reproductive health be a problem but finding the space to keep a patient in a room longer or adding a provider to address those topics would be challenging. Provider 14 explained the logistical challenge: “I think clinic time and space. If you only have a 30-minute slot and. . . if you run out of time. . .sometimes those [fertility or FP topics] are the things that unfortunately get bumped.”
Facilitators
The providers also specified known or potential facilitators for bringing up the topic of fertility or FP with patients. Some of these related specifically to the provider themselves, including having good relationships with the patient. Another facilitator involved having relationships with fertility specialists. These relationships would simplify the referral process and standardize provider action when a patient is interested in learning more about their reproductive options. Further facilitators for enabling discussions of FP or fertility included normalizing the discussions and imparting education for providers and patients.
Provider specific facilitators
Some providers felt that having trusting relationships with their patients enabled them to bring up sensitive topics more easily, “I’ve been in this role for 19 years. . . I’ve known these patients. That’s what I love about CF is that it’s a chronic disease that you get to know your patients and feel very comfortable with them,” recounted Provider 17. Providers recognized that having personal, friendly relationships with patients aid in their ability to talk about fertility or reproductive health. Provider 19 explained how having a relationship with a patient who would likely have a lung transplant in the future would allow her to feel comfortable bringing up the option of FP: “If I knew a patient really well, I think I’d maybe bring it up, especially if it [transplant]. . .probably is coming. . .I think it would be easier to bring it [FP] up.”
Relationships with fertility specialists
Although not always available or even feasible depending on the infrastructure of the health care system wherein the CF clinic is located, having the opportunity to collaborate with, or refer to, fertility specialists is a particularly salient facilitator. Provider 18 described a high-functioning collaborative approach currently established at their center: “We have developed a relationship with a maternal and fetal health provider who has developed an interest in CF. We collaborate with her regularly with our patients who are pregnant. Then we coordinate CF clinic visits with prenatal visits, and so it can all happen on the same day and there can be good discussion between all team members.”
In clinics that did not already have a referral system or partnership in place, it was highly desired. Having an option to refer patients to a fertility specialist would ease the lack of knowledge and comfort currently plaguing CF care team providers and ultimately be beneficial to patients. “I think that would be fantastic to have one go-to for all of our pregnant patients and for all of our fertility referrals. . . we could learn a lot from that individual,” stated Provider 13.
Additionally, while having an embedded fertility specialist as part of the CF care team would be ideal, it may not be feasible for all clinics. The expense, time, and space required to include an additional CF team member are considerable barriers for many clinics. Provider 2 was also cautious but hopeful about integration of fertility specialists, “In a perfect world, yes, I think that would be awesome if we could have an OB. Even a nurse practitioner trained. I think that would be ideal.”
Normalize the discussion
Eleven of the 20 providers indicated that it would be helpful to bring the topic up regularly and predictably. Study participants suggested standardizing the discussion so that patients and providers know when the discussion would take place. Provider and patient discomfort from speaking about sensitive topics may be eliminated by having the discussions regularly. Provider 14 described a need to speak about it with predictability, “I think if you standardize it, nobody would [be] taken by surprise. . . we talk about it just like we talk about enzymes, and nutrition, and goin’ to college. . . it just becomes a part of their preventative care.”
Education for providers and patients
Fourteen of the 20 providers described the necessity of education for both providers and patients regarding fertility in women with CF, as well as the option of FP. “I think staff education is where that starts, and I think having educational materials would be a huge facilitator,” recommended Provider 3. To better serve people with CF, providers were interested in learning more about fertility and FP options, however, the opportunity to learn more about these specialty topics is not readily available. Provider 7 expressed, “I mean we would love to learn about it [reproductive options for women with CF]. It’s just, we don’t have a lot of resources for that in [specific U.S. state].”
Readily available content to aid in the education of both providers and patients was a decidedly apparent desired commodity. Provider 18 gave very specific recommendations, “I think that some standardized, vetted, centralized content that’s written in plain language and ideally translated into Spanish would be helpful.”
Discussion
In response to the research questions guiding this study, we learned that: (1) CF providers feel underprepared to discuss FP as an option prior to lung transplantation, (2) that CF Centers could benefit from having a plan in place to guide women with CF with any decisions about FP, and (3) that CF providers do view reproductive health as an important aspect to overall health, however, there is so little knowledge of or resources for FP, that they do not feel that they can counsel women about this option. Findings from this study revealed several clinically relevant implications. First, providers acknowledge that the CF world has entered a new era, in which people with CF are living longer and have the opportunity to experience developmental milestones that were not previously possible for them. Therefore, it is essential for the CF care team to have a central role in addressing options for parenthood. Second, providers want to support and advocate for their patients and have been trying to address or circumvent barriers. They recognize that while they may not agree with their patients’ decisions, they still support the autonomy and life goals of the people they serve. Third, providers are not afraid of having fertility or FP conversations with patients, but there are barriers, such as a lack of information, that they feel must be addressed so that they can knowledgeably present options to their patients. To address numerous barriers to FP discussions, providers identified several strategies, including education for both providers and people with CF, normalization of fertility and FP discussions, and having collaborative relationships with reproductive specialists. Ultimately, CF providers recognize the importance of their role in sexual and reproductive health (SRH) discussions.
Kazmerski et al 10 found that discussions of SRH among adolescent and young adult women with CF do not occur regularly in the CF clinic. The findings from the current study support Kazmerski et al’s 10 findings, with CF providers reporting many barriers that prevent them from engaging in meaningful, patient-centered conversations about SRH. In another qualitative study of women with CF and their thoughts about pregnancy, women reported that the CF team did not communicate with them about fertility and reproduction, as well as a need for more education and counseling in the area of SRH. 11 Providers in the current study corroborated the findings by Kazmerski et al, 11 indicating that both the patient and providers acknowledge that there is a lack of intentional and meaningful discussions about SRH in the CF community. The current study adds more evidence to the scientific literature that CF-specific SRH education is lacking.
Limitations
One limitation of this study is that the majority of participants were female. Having a male perspective could provide more insight specifically into the perceptions of the gender differences in having fertility or FP conversations in the CF community. Another possible limitation is the use of women’s health services which may exclude persons who can gestate but do not feel comfortable seeing a women’s healthcare provider. Another potential limitation is in the transferability of these findings to other chronic diseases. While the sample described here is only CF providers, other chronic conditions may have similar concerns related to SRH. Findings from this study can serve to provide insight into discussions related to fertility and FP in other rare or chronic diseases, with hopes that more specific knowledge may one day come to serve other disease populations.
Practice implications
The CF providers who participated in this study provided actionable ideas for improving patient-provider discussions related to fertility and FP. Figure 1 contains a checklist of options for providers to consider when implementing changes in their SRH discussion protocol based on suggestions provided by the participants in this study. First, providers need additional education regarding fertility and FP options for women with CF, and research is warranted to identify the best approach to providing this specialized education and training. Fertility and FP is a relatively new area of research as people with CF are now living long enough to start having these discussions. Second, there is opportunity to work with obstetricians, gynecologists, or other fertility specialists to meet the unique needs of women with CF. While some CF clinics already have established collaborative relationships, the majority do not. As the CF community continues to thrive in the new era of CF care, it is imperative that CF clinics develop a formal infrastructure to support the needs of women with CF across the lifespan, which includes motherhood. Third, SRH and FP discussions must be normalized in the CF care model. Patients and providers need to be aware that these discussions will occur at regular intervals to meet patients at their current life stage.
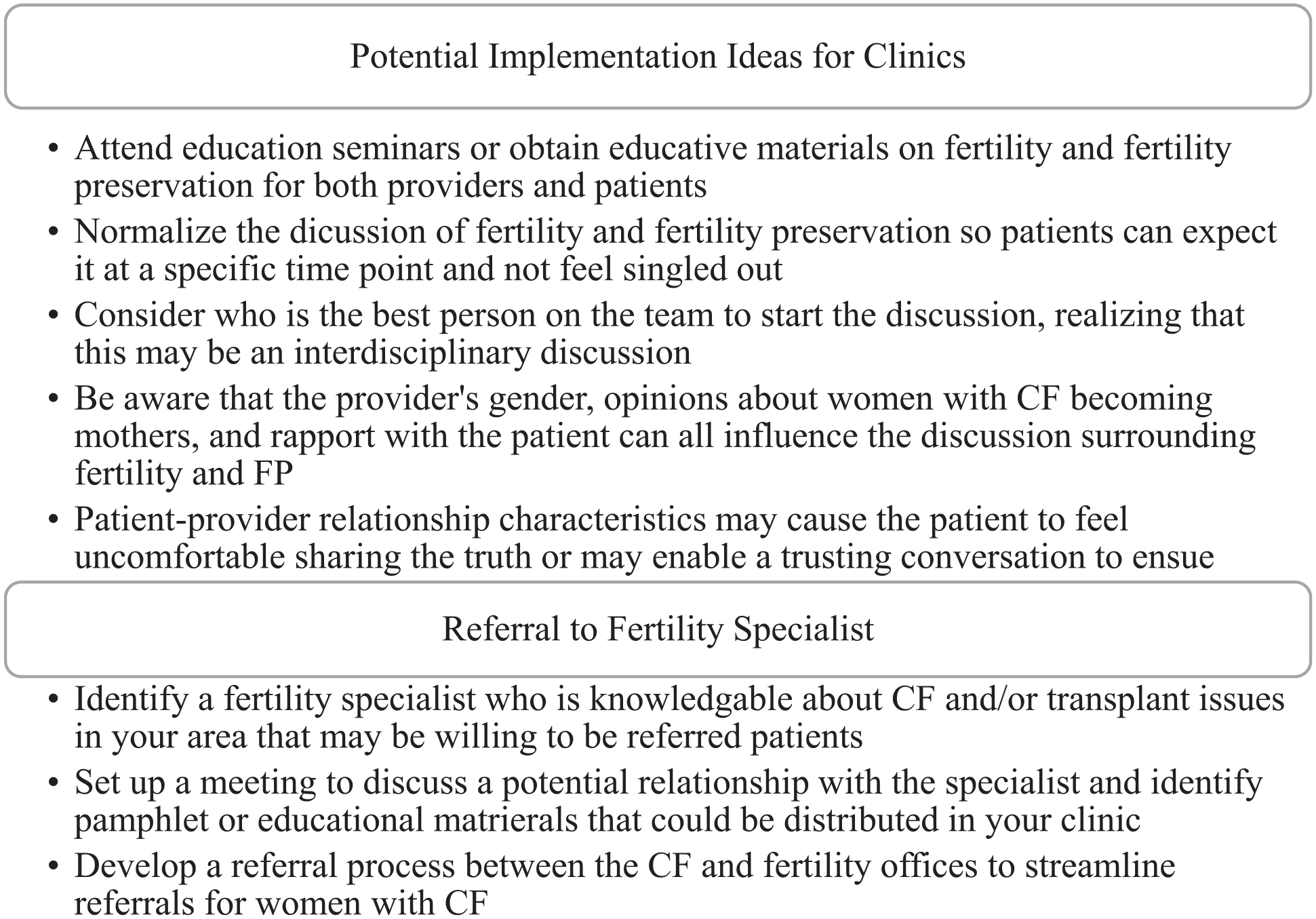
Facilitators identified by providers that clinics may benefit from implementing.
Conclusion
The results of this study highlight opportunities for improvement in initiating and sustaining patient-centered discussions about fertility and FP in the CF community. Further research must be done to determine the best ways to integrate these discussions into standard practice for comprehensive care delivery. With advancements in medicine and technology, options for motherhood for these women have changed, and CF providers need specialized knowledge and tools to fully support and guide their patients through the life course.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NICHD under grant 1R03HD097262 – 01. APC funding for this article was supported by the UAB Libraries APC Fund.
Ethical Statement
This study received institutional review board approval at the authors’ university before the study began.