
Abstract
This descriptive study retrospectively evaluates the reach and impact of cohorts enrolled in Group (in-person, 2017-2020) and Self-Directed (remote, 2019-2020) delivery formats of the evidenced-based health promotion program, Walk with Ease, implemented statewide in North Carolina. An existing dataset consisting of pre- and post-surveys were analyzed for 1,890 participants; 454 (24%) from the Group format and 1,436 (76%) from Self-Directed. Self-Directed participants were younger, had more years of education, represented more Black/African American and multi-racial participants, and participated in more locations than Group, though a higher percentage of Group participants were from rural counties. Self-Directed participants were less likely to report having arthritis, cancer, chronic pain, diabetes, heart disease, high cholesterol, hypertension, kidney disease, stroke, or osteoporosis, though more likely to report being obese or having anxiety or depression. All participants walked more and expressed higher confidence in managing joint pain following the program. These results promote opportunities for enhancing engagement in Walk with Ease with diverse populations.
What do we already know about this topic?
The Walk with Ease program has been shown to help people with arthritis and chronic pain to reduce pain, stiffness, and fatigue, while increasing balance, strength and walking pace, and improving overall health in various populations.
How does your research contribute to the field?
The differences observed between Group and Self-Directed Walk with Ease participants in this study advance our understanding about the 2 delivery formats and point to opportunities for enhancing participation and engagement in the program with more diverse populations in the future.
What are your research’s implications toward theory, practice, or policy?
Expanding upon existing participant recruitment pathways for and ensuring availability of both delivery formats of Walk with Ease is needed to have the broadest possible reach and impact.
Introduction
Healthy Aging NC an initiative of the North Carolina Center for Health and Wellness at the University of North Carolina Asheville, serves as a statewide resource center for evidence-based community health programs such as Walk with Ease (WWE). WWE was developed by researchers at the University of North Carolina, Chapel Hill, in collaboration with the Arthritis Foundation, and has been recognized by the Osteoarthritis Action Alliance and the Centers for Disease Control and Prevention as an arthritis-appropriate, evidence-based intervention. These interventions are community-based programs that have undergone a review process and met established criteria to have a positive impact on persons with arthritis. 1
The WWE program has been shown to help people reduce pain, stiffness, and fatigue, while increasing balance, strength and walking pace, and improving overall health.2-4 WWE participants have shown more confidence, less depression, less health distress, and less pain than control groups. 5 WWE has also been established as suitable for implementation by organizations for workplace wellness programs to increase physical activity.6,7
The COVID-19 pandemic shed a light on the health disparities that historically marginalized and rural populations have been experiencing across North Carolina (NC).8,9 This called for Healthy Aging NC to expand its menu of evidence-based health programs to include remote and virtual delivery formats of the evidence-based health programs we support to reach more diverse and underserved populations. WWE was uniquely positioned to help accomplish this, having already established a Self-Directed delivery format of the program, where participants are able to complete the program from home. The COVID-19 pandemic helped open the door for further operationalizing and streamlining referral pathways and data collection for the Self-Directed delivery format. Relevant questions were included in the data collection tools to help understand what populations were being reached through this delivery format. WWE participants were enrolled into 1 of the 2 delivery formats of the program utilizing funds from a 5 years Centers for Disease Control and Prevention grant. This funding allowed us to offer the program at no cost to participants.
This descriptive study reports and examines the characteristics of participants of the traditional in-person, instructor-led delivery method, Group (2017-2020), and the remote delivery method, Self-Directed (2019-2020), of the WWE program implemented in NC. In partnership with the Osteoarthritis Action Alliance, Healthy Aging NC analyzed existing data on participants of WWE to observe the relationships between delivery method, Group or Self-Directed, and all other documented variables available including demographic information, location, and pre- and post-program survey results.
Methods
Study Design
This is a descriptive study of all individuals who participated in the evidence-based program, WWE, in NC between 2017 and 2020. In this secondary data analysis, it is a convenience sample of all those who self-selected into the program in 1 of 2 formats, Group or Self-Directed, and filled out a pre-program survey. The sample size was determined by participant self-selection into the program over these years; no power calculation was conducted for this study.
Location
Group program participants engaged in the program at senior centers, Area Agencies on Aging, and other sites in 21 counties in North Carolina in 2017 to 2020. Recruitment was rolling based on when and where group classes were offered. Self-directed participants engaged in the program where they work or live in all 100 counties in NC in 2019 to 2020. Recruitment of NC state employees occurred in fall of each year and others joined as they learned about it through open enrollment.
Intervention
Group WWE is an 18-session program that meets in-person for 1 h, 3 times per week, for 6 weeks. All participants receive a WWE guidebook which includes health education materials to support participants through the program such as: a walking contract, goal setting and walking tracking forms, a recommended walking schedule, and self-assessments. Each Group WWE session consists of a brief interactive health education session, warm-up, stretching, up to 35 min of self-paced walking, and cool-down activities. Group WWE leaders support participants in developing specific, measurable, and attainable goals and in navigating the WWE guidebook to encourage engagement between group classes. Group WWE can be adapted to accommodate various levels of ability, including individuals who need an assistive device to walk. 10 Group WWE is facilitated by a certified leader who has undergone an Arthritis Foundation approved online training which consists of reading a guide, watching webinars, and passing a multiple choice test. Group WWE leaders must also maintain a CPR Certification and are responsible for taking attendance, distributing pre- and post-program surveys, and submitting paperwork back to Healthy Aging NC.
Self-Directed WWE is entirely self-led by the participant who receives the guidebook and completes the 6-week program on their own schedule. Self-Directed participants can choose whether they’d like a digital copy of the guidebook in PDF format, or if they’d like a print copy shipped to their mailing address of choice. Self-Directed Enhanced WWE is an additional delivery format that can be implemented virtually by a trained WWE leader who determines the level and type of engagement with participants throughout the 6-week program and encourages participants to walk on their own, while starting and ending the program at the same time with a group of individuals. The CPR certification requirement is waived for leaders implementing this delivery format. For the purposes of this study, Self-Directed Enhanced participants were grouped with Self-Directed participants.
Participants
Participants self-selected into participation in both the Group delivery of WWE and the Self-Directed WWE programs. To be eligible, participants had to be at least 18 years of age. WWE was developed by the Arthritis Foundation as a strategy for managing and preventing arthritis, as such participants were not required to have arthritis.
Participants in the Group delivery method of WWE typically found the program through the marketing and promotion efforts of the community-based organization (CBO) hosting the program. There are a number of toolkits available to these CBOs provided by the Arthritis Foundation, Osteoarthritis Action Alliance, and Healthy Aging NC to support these efforts. Healthy Aging NC’s primary network of partners include NC’s 16 Area Agencies on Aging (AAAs) and the CBOs they are connected with such as senior centers, residential facilities, parks and recreation departments, and more. Group WWE leaders promote the program and recruit participants using flyers, online announcements, and/or word of mouth.
Program promotion for Self-Directed WWE was most often conducted in partnership with NC’s Office of State Human Resources, which promoted WWE as a “warm up” to an established state employee walking initiative called Miles for Wellness. Wellness leaders of state entities across NC shared the opportunity with their employees to sign up through the Self-Directed WWE registration portal hosted by the Osteoarthritis Action Alliance. The portal continues to be available on an ongoing basis and shared freely with Healthy Aging NC’s partners. Any adult residing in NC who could benefit from the program can register at any time and at no cost to them.
All participants who enrolled in either delivery method in NC between 2017 and 2020 were included in the sample of this study and agreed for their de-identified data to be analyzed and reported on as part of the enrollment processes.
Data Collection and Analysis
A collaborative project led by the North Carolina Center for Health and Wellness established a process of centralizing data collection and entry into a national database for the purpose of measuring the reach and impact of evidenced-based health programs offered by Healthy Aging NC’s partner organizations across NC. The data collection packets required for Group WWE leaders to submit included workshop cover sheets, attendance tracking forms, and pre- and post-program surveys and were mailed or scanned and emailed via encryption to Healthy Aging NC’s data administrator.
The Osteoarthritis Action Alliance supports the data collection process for NC’s Self-Directed WWE participants through the online registration and engagement portal they host that requires participants to fill out pre-program information as a part of the enrollment process and provides access to post-program surveys following completion of the program. The portal additionally enables automated weekly motivational email messaging following enrollment and has expanded to support weekly goal setting and success tracking, links to printable tools and resources, and certificates of completion for those who finish the post-program survey.
The pre- and post-program surveys that all participants receive as part of their involvement in the program include self-reported demographic information along with questions about their days and minutes spent walking and their confidence levels managing joint pain and stiffness on a scale of 1 to 10. See Supplemental Appendix A and B to review the pre- and post-surveys (modified versions of validated evaluation tools for the WWE program 11 ). The University of North Carolina Asheville’s Institutional Review Board approval and the Osteoarthritis Action Alliance’s Institutional Review Board exemption were received for all data collection tools and methods.
Demographic, location, and pre- and post-program survey information from the existing data sets described above were scaled and analyzed. Independent Sample t-tests were used when comparing numerical data from pre-surveys between Group and Self-Directed participants. Chi-Squared tests were used when comparing pre-survey categorical data between groups. To understand the impact of the program on participants within each group, paired sample t-tests were used to assess differences in pre- and post-surveys. All analyses were conducted using SPSS V25.
Results
Data was collected on a total of 1,890 WWE participants in NC from 2017 to 2020, 454 (24%) of which participated in the Group delivery method and 1,436 (76%) of which participated in the Self-Directed or Self-Directed Enhanced delivery method of the program. The statistically significant differences (P < .005) observed between Group and Self-Directed participants demonstrated that Self-Directed participants were younger, had more years of education, and represented more Black/African American and multi-racial individuals than Group participants. Self-Directed participants were also less likely to report having arthritis, cancer, chronic pain, diabetes, heart disease, high cholesterol, hypertension, stroke, and osteoporosis, though more likely to report being obese and having anxiety or depression than Group participants. Demographic information about all participants is presented in Table 1.
Characteristics of Group (G) and Self-Directed (SD) WWE Participants in NC, 2017 to 2020.
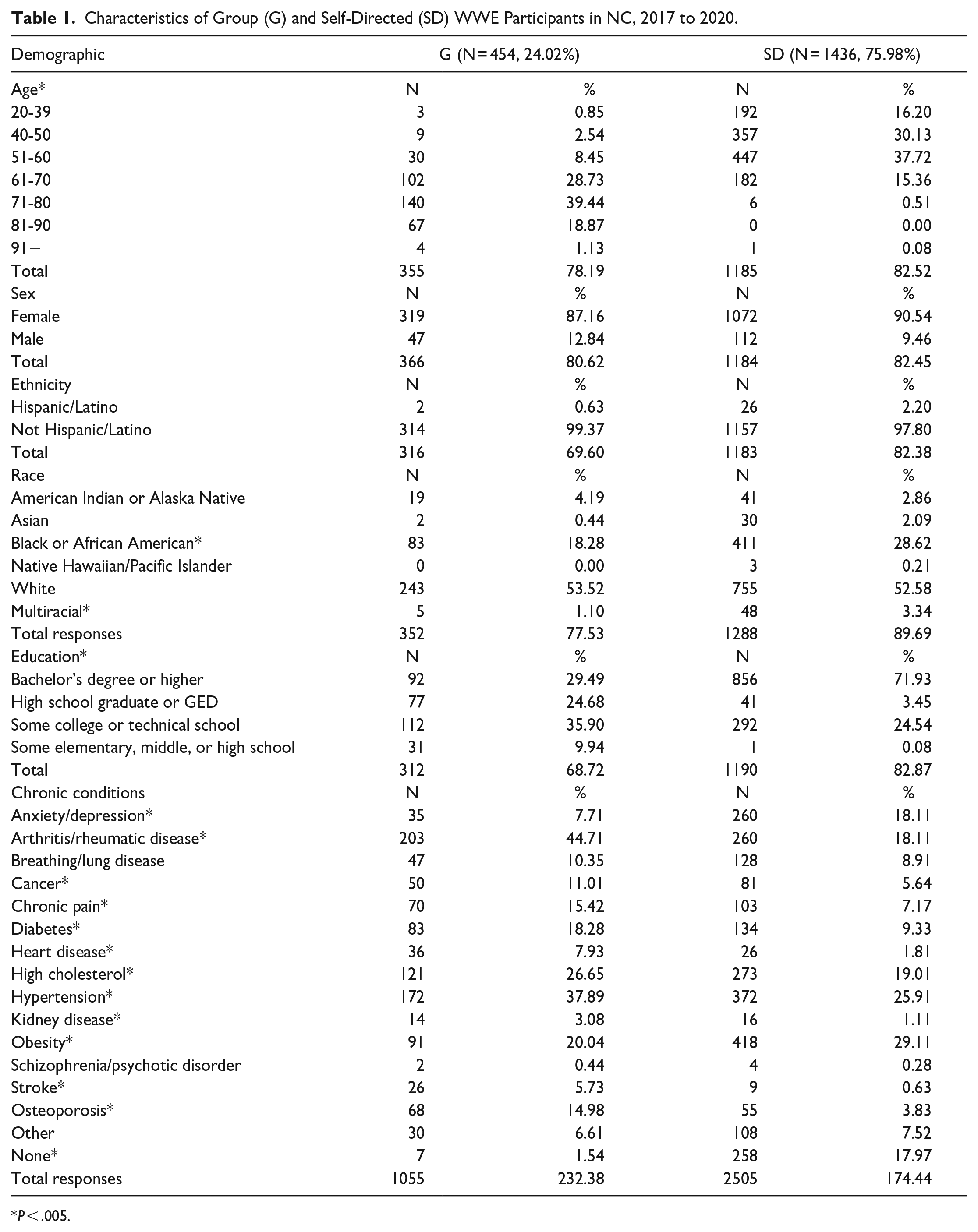
P < .005.
Group participants completed 454 pre-surveys and 219 post-surveys. Self-Directed participants completed 1,436 pre-surveys and 240 post-surveys. As seen in Table 2, Group participants significantly increased their average minutes spent walking per day by 8.12 and their average days walking per week by 1.23. Their average confidence levels managing joint pain and stiffness also increased by 0.26 on a 1 to 10 scale, though this result did not show statistical significance. Self-Directed participants significantly increased their average minutes spent walking per day by 6.00, their average days walking per week by 1.23, and their average confidence levels managing joint pain and stiffness by 0.60 on a 1 to 10 scale. 97.8% of Self-Directed and 99.5% of Group post-survey respondents said they would recommend the program to a friend as well.
Mean Pre- and Post-Program Survey Results for Group (G) and Self-Directed (SD) WWE Participants in NC, 2017 to 2020.

Significant differences (P = .000, t = −5.286) were also observed between the zip codes listed for Group and Self-Directed participants. Self-Directed participants represented a larger variety of zip codes and a wider spread of participants across the state than Group participants, as seen Figures 1 and 2, showcasing NC state maps of where Group and Self-Directed participated in WWE. However, Group participants represented a greater percentage of rural counties than Self-Directed participants, as seen in Figure 3.

Map of group WWE participants in NC, 2017 to 2020.

Map of Self-Directed WWE participants in NC, 2017 to 2020.

Rural versus Urban Counties represented in Group (G, N = 454) and Self-Directed (SD, N = 1,241) WWE participants in NC, 2017 to 2020 17 .
Discussion
Demographic Comparison
Self-Directed participants were younger on average than Group participants given the differences in approaches to program promotion between the 2 delivery formats. The difference between age groups with older adults typically lagging behind younger adults in internet use in their everyday life might also help explain this. 12 This highlights a strength of the Self-Directed format because when individuals engage in healthy habits earlier on in life, early onset of arthritis and other chronic conditions that benefit from active lifestyles can be mitigated. 13
Group participants were recruited through the aging network, with 76.0% participating in the program at a AAA or Senior Center, while Self-Directed participants were recruited through the Office of State Human Resources, with 81.4% actively working as state employees when enrolled in the program. This may also explain why Self-Directed participants had more years of education and reported less chronic diseases with the exceptions of anxiety, depression, and obesity. These 3 latter conditions have all been correlated with sedentary jobs and lifestyles which could explain this difference.14-16
As anticipated, Self-Directed WWE reached more participants (1,436 participants; 76.0%) than Group WWE (454 participants; 24.0%) by creating an opportunity for individuals to participate from anywhere, without relying on a physical location or leader. Additionally, more Self-Directed participants identified as Black/African American and multi-racial compared with Group participants. This is related to Self-Directed participants also representing a wider variety of zip codes across the state of NC (see Figures 1 and 2). Self-Directed WWE is more accessible in that it can be completed from anywhere at no cost to program providers or participants and therefore reaches a more diverse population in terms of race and location.
However, Group WWE reached a greater percentage (57.0%) of participants in rural counties across the state than Self-Directed WWE (26.5%) as seen in Figure 3. Group participants were recruited in communities where they live and therefore are concentrated in counties where organizations have the capacity to offer and promote the program. In fact, over 25% of all Group participants came from only 3 rural counties. Whereas, in order to register as a Self-Directed participant, access to the internet and a certain level of technological literacy was required.
Although there were no significant differences in gender representation between the 2 groups, there were many more female than male participants in both groups. This is consistent with other WWE participant demographics.2,6,7,11,18 Some possible reasons for this include lifespan being longer and arthritis prevalence being higher in women than men, and therefore women being more drawn to a program developed by the Arthritis Foundation that caters to older adult populations.19,20
Program Impact
In this study, all participants walked more days and minutes on average and expressed higher levels of confidence in managing joint pain and stiffness following completion of the program than at the start of the program. These findings are consistent with existing literature establishing both Group and Self-Directed WWE as arthritis-appropriate evidence-based interventions.11,21 Group participants appeared to have higher mean improvements in days and minutes spent walking, however, with the law of initial values 22 at play, considering Self-Directed participants started at a higher baseline and were therefore expected to see less improvements than Group participants (see Table 2). Additionally, people with greater social support for physical activity are more likely to participate in leisure time physical activity which may also help explain these apparent differences. 23
Limitations
All demographic information and pre- and post-program survey results were self-reported by participants and therefore lend themselves to personal biases. Response rates on the post-program surveys were also limited. The average online survey response rate in published research is 44.1% 24 and response rates for Group participants ranged from 38.8% to 48.2% and from 15.9% to 16.7% for Self-Directed participants, depending on the question with a total of 219 Group and 240 Self-Directed participants submitting a post-program survey. Additionally, while offering the WWE program remotely has many advantages (flexible scheduling, generating greater rates of enrollment into the program, and representing younger and more diverse populations), it’s much more challenging to collect post-program surveys and therefore also more difficult to understand completion rates and other potential benefits of this delivery format.
Future Recommendations
Existing literature offers recommendations for overcoming barriers to WWE implementation and evaluation such as relying on experienced volunteers or organizational staff rather than volunteer lay leaders to implement WWE, evaluating available resources prior to program implementation, identifying internal program champions, and assessing potential delivery method adaptations that could improve the fit between the WWE program and the organization offering it.16,18,25-27
The Osteoarthritis Action Alliance’s 2.0 WWE registration and engagement portal offers an opportunity for Healthy Aging NC to approach this by customizing recruitment efforts into various specific groups across the state, rather than focusing on state employees alone. To address low post-survey participation rates and lack of information about Self-Directed participant engagement in the program, providing Self-Directed participants more regular opportunities to provide feedback such as weekly emails or texts with mini-surveys or requests for responses may open more lines of communication between WWE program providers and self-directed participants. This way, more information about participant engagement could be captured throughout the 6-week program.
Further, the results of this study point to opportunities for deepening collaborations between organizations that are focused on arthritis prevention and management with those that are focused on obesity, anxiety, depression, and other chronic conditions to reach younger audiences and for employers to adopt Self-Directed WWE as an employee wellness program.
The differences observed between Group and Self-Directed WWE participants in this study advance our understanding about the 2 delivery formats and point to opportunities for enhancing participation and engagement in the program with more diverse populations in the future. Expanding upon existing participant recruitment pathways for and ensuring availability of both delivery formats of WWE is needed to have the broadest possible reach.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580231152314 – Supplemental material for Reach and Impact of In-Person and Remote Delivery Formats of Walk with Ease
Supplemental material, sj-pdf-1-inq-10.1177_00469580231152314 for Reach and Impact of In-Person and Remote Delivery Formats of Walk with Ease by Nadia Z. Mazza, Amy Joy Lanou and Serena Weisner in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580231152314 – Supplemental material for Reach and Impact of In-Person and Remote Delivery Formats of Walk with Ease
Supplemental material, sj-pdf-2-inq-10.1177_00469580231152314 for Reach and Impact of In-Person and Remote Delivery Formats of Walk with Ease by Nadia Z. Mazza, Amy Joy Lanou and Serena Weisner in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
NCCHW’s Data Administrator, Janice Self; NCCHW’s Emeritus Health Coach, Ellen Garrison; Arthritis Foundation’s Director of External Affairs, Nick Turkas.
IRB approval was awarded or exempt for all data collection methods (IRB numbers: 1673856-3 UNC Asheville IRB; 19-0621 OAAA IRB Exemption).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible by cooperative agreement CDC-RFA-DP18-1803, grant number NU58DP006449 from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
Copyrighted Material Statement
No copyrighted surveys, instruments, tools, and/or any other copyrighted material was used for or within this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.