
Abstract
Patient handover, which is a method of moving the clinical data of patients to another individual or professional community, is a high-risk area for the safety of patients due to errors which can happen during staff break time, changeover shifts, and when patients are moved in and out of units. Standards for critical care nurses will improve bedside handover due to the presence of clear plans implemented by nurses who are well informed about them. To develop nursing standards for maintaining handover in the intensive care unit. A methodological and cross-sectional study was conducted at Mansoura University Hospital and included 15 experts and 150 staff nurses. Twelve items were excluded from the tool because their CVR ratio was less than 0.7. Therefore, after eliminating 12 items, the number of tool items produced was 66. The Kaiser–Meyer–Olkin value = 0.713, with the recommended value being 0.6 or above. The cut-off score for the analysis model was 0.3, and the KMO value criterion was greater than 1, which defined eight-factor loadings as the best fit for the results, accounting for 69.5% of the variance. The aim of this study was satisfactorily achieved, with 0.9055 validity and reliability for the handover instrument, which consisted of 60 items with a total reliability score.
Handover is an important nursing care process, particularly in the field of critical care.
Improving nurse handovers will contribute to improving the safety of patients.
Applying nursing standards concerning handovers in intensive care units leads to successful outcomes and increased safety for critically ill patients.
Introduction
Handover is an important nursing care process, particularly in the field of critical care, since it requires the transfer of patient data. Improving nurse handovers will contribute to improving the safety of patients. In order to deliver quality care, nurses need to be well trained and have the expertise to prevent mistakes and improve patient well-being. 1 Clinical handover is important for making clinical decisions and providing effective, high-quality nursing care. Inadequate and incomplete transfer of data can lead to unsatisfactory outcomes. 2 Clinical decision-making and the provision of efficient, high-quality, continuing care require communication skills, and clinical knowledge regarding nursing shift-to-shift handover.3,4
Critically ill patients are an important centre of care for nursing practice. For a healthy work environment, nurses must be able to collaborate and communicate effectively and to update information and their skills regarding their delivery of treatment, all of which contribute to the achievement of patient safety.5,6 During bedside handover, communication and nursing expertise are important considerations. The most significant issue with paperwork is handover, which is resolved by electronic documentation. It is important for hospital systems to implement policies and utilize standards to improve verbal and written communication involved in the handover of information by making it easy and understandable. 7
The standards may be helpful if nursing staff report concerns with verbal communication during bedside handover. There are 3 sources of patient information in the bedside handover: verbal, nurse notes, and highlighted critical information. 8 Standards for critical care nurses will improve bedside handover due to the presence of clear plans implemented by nurses who are well informed about them. 9 Patients may suffer direct effects because of insufficient or non-existent handovers. 10 Such handover issues can cause delays in diagnosis and management as well as missed or duplicated testing and the implementation of inappropriate care plans. 11
Simple forms can be used to help nurses quickly fill in bedside handover information, thus improving documentation and standards for critical care nursing. However, a new hospital standard can provide several challenges during a bedside handover, including differences in nurses’ comprehension, knowledge, coping, and motivation to put it into practice. These concerns can have a significant impact on bedside handover, especially in first-time application. 12 Nurses require training and resources to practice effective handovers that fulfill the needs of their employers, peers, and patients. Furthermore, applying nursing standards concerning handovers in intensive care units (ICUs) leads to successful outcomes and increased safety for critically ill patients. 13 How to conduct a successful handover has been evaluated in a small number of studies.14,15
According to research conducted in Egypt, 77% of nurses were dissatisfied with the present handover procedure. A 30% error rate throughout the handover process was attributed to poor communication. 16 In Egypt, there are no standards for carrying out a successful nursing handover. Thus, the aim of this study was to develop nursing standards that ensure effective handovers for nurses working in ICUs in the Emergency Hospital at Mansoura University.
Materials and Methods
Study Design
To achieve the aim of this study, a methodological and cross-sectional design was adopted. To implement the study, 3 steps were undertaken which analyze the validity of a new or modified measuring tool. The first step was to assess the content validity scale of the handover standard by evaluating inter-rater agreement among 15 experts, which includes 5 experts in administrative roles and 10 critical care nurses from the study setting. The second stage assessed the internal consistency of the developed items, using Cronbach’s alpha test. Finally, the third stage assessed construct validity by using exploratory factor analysis (EFA).
Setting
This study was conducted in 5 ICUs at Mansoura University hospital and Emergency hospital, including the surgical ICU (9 beds) and anaesthesia (8 beds) ICU at Mansoura University hospitals and the medical, surgical, and general ICUs at the Emergency hospital. The medical ICU includes 10 beds that receive patients who experience neurological impairment, poisoning, or shock. The surgical ICU contains 10 beds providing care for patients with trauma and surgical disorders. The general ICU includes 4 beds. All ICUs have access to advanced technology and provide care to critically ill patients. The nurse–patient ratio is nearly 1:2.
Population
Group 1 consisted of a convenience sample of 15 experts in administrative roles and critical nursing staff (4 administrative workers and 4 critical nursing staff working as academic professors from administration and critical care and emergency departments, 3 senior researchers with PhDs, 2 doctoral students, and 2 head nurses from hospitals). Group 2 included 150 nurses who worked and provided direct patient care in critical care units. According to the sample size calculator, a margin of error of 5%, a confidence level of 95%, and an estimate of P: .25, the total sample size was 150 nurses. The convenience sampling used the following inclusion criterion: all nurses who have been working in a critical care unit for at least 6 months.
Data Collection
Step 1: Content Validity
In the development phase of the instrument, a review of the literature and a Delphi procedure were carried out. 17 The content validity of the handover standard tool was determined to evaluate the extent to which the questionnaire items measure handover standard technique. Construct domains were determined qualitatively during the tool development process, as stated above. An extensive literature review9,18,19 allowed for finding items that were brief. Applying a quantitative approach to content validity, 20 the items were closely examined by 15 experts in administrative roles and critical nursing: 2 medical consultants, 2 head nurses from the study setting, 2 academic staff from administration, 4 professor faculty members in critical care and emergency departments, 3 PhD senior researchers, and 2 doctoral students. According to their perception of the importance of the handover standard, they ranked each item on a 3-point scale: essential (3), useful but not essential (2), or not essential (1). The following equation was used to compute the content validity ratio (CVR) for each item: CVR = (E − N/2)/(N/2), where N represents the total number of assessors, and E represents the number of assessors who rated the item as “important.” The score was accepted if it fell between 0.7 and 1. 21 Twelve items were excluded from the developed tool because their CVR score was less than 0.7; thus, the number of items ended up at 66 after excluding these 12 items.
Step 2: Internal Consistency
After we collected the data from the 150 studied staff nurses by using the new version of the tool, their responses were evaluated on a 3-point scale (0 = does not apply, 1 = applies incompletely, 2 = applies completely). Then, internal consistency analyses were performed, calculating Cronbach’s alpha for each subtest. 22 Cronbach’s alpha ranges from r = 0 to 1, with r = .7 or greater considered as sufficiently reliable. Forty items had good internal consistency (ranging from 0.7 to <0.9), 11 items had excellent consistency (≥0.9), 9 items ranked at acceptable consistency (0.6 to <0.7), and 6 items had poor and thus unacceptable consistency and so were excluded from the study. Therefore, the tool was reduced to 60 items.
Step 3: Construct Validity
The construct validity of the full sample (N = 150) was calculated using factor analyses. 23 The sample obtained a Kaiser–Meyer–Olkin (KMO) value of 0.713 (the recommended value is 0.6 or above). The cut-off score for the analysis model was 0.30, and the KMO value criterion was greater than 1, which defined eight-factor loadings as the best fit for the results, accounting for 69.5% of the variance. All 60 items were incorporated into the checked factor solutions, with a factor weight exceeding 0.3.
Ethical Considerations
The study was approved by the Research Ethics Committee of the Faculty of Nursing, Mansoura University (ref. no. P.0226) and by the hospital administration where the study was conducted. The study’s aim was explained to all nurses, and written informed consent was obtained from the subjects prior to study initiation. They were informed that participation is voluntarily and that they have the right to withdraw without any penalties. Also, confidentiality was assured through data coding. Data were safely stored in a cabinet, and no one had access to the data except the investigators.
Analysis
Statistical analyses were conducted using the Statistical Package for the Social Sciences Version 23. 24 Before beginning the analyses, the researchers ensured that all of the standards for recording integrity and scoring accuracy were met. Reliability of internal consistency was measured by using the alpha (or alpha coefficient) of Cronbach, developed by Lee Cronbach in 1951, which tests reliability or inner consistency. Cronbach’s alpha ranges from 0 to 1, with an r = .7 or above deemed adequately precise. EFA of variables in multivariate statistics is the mathematical approach used to discover the underlying function of a relatively large number. EFA is a technique for factor analysis whose major aim is to identify the fundamental relationships between variables measured. To confirm the factor structure of the instrument, the principal component factor analysis with variable-max rotation was utilized as an EFA. The data are suitable for factor extraction, as shown by Bartlett’s test of sphericity and the KMO indicator (the recommended value is 0.6 or above7; Bartlett’s test of sphericity: P .001).
Results
Table 1 reveals that 46.7% of experts were aged between 41 and 50 years, while 52% of staff nurses had an age range between 30 and 40 years. Regarding length of experience, 40% of experts and 60% of staff nurses had between 11 and 15 years of experience. When surveyed about previous workshops, all experts reported attending previous workshops, while only 25.3% of staff nurses had attended workshops.
Characteristics of Studied Experts and Staff Nurses.

Table 2 reveals that, from the pool of 78 items, 66 were rated by all 15 assessors as essential or useful for a handover standard tool, with a CVR that ranged from 0.7 to 1.0, and these items were kept. However, 12 items were rated as not useful or unessential by the majority of assessors, with a CVR ranging between 0.55 and 0.64. These items were discarded. Then, the 66 items’ reliability was measured using Cronbach’s alpha test. Six items (2, 8, 20, 21, 55, and 64) had a reliability score between 0.48 and 0.58, and thus we excluded those items from the tool. The remaining 60 items had reliability scores ranging from 0.64 to 0.93.
Content Validity Ratio and Internal Consistency for Handover Tool Items.

The 60 handover items were formatted on a Likert-type scale, which was administered to the staff nurses who enrolled in the study. The EFA in Table 3 revealed an 8-factor solution, with 60 items loaded above critical level, ranging from 0.53 to 0.9. Therefore, all 60 items were included because no items were loaded as low or non-significant. Following the literature review, the 8 factors were identified as organization, time and place, leading handover, communication, handover sheet, nursing care, documentation, and outcome. The 8 factors explained 67.5% of the overall variance when considered together.
Exploratory Factor Analysis for 60 Items of the Handover Tool (N = 150).
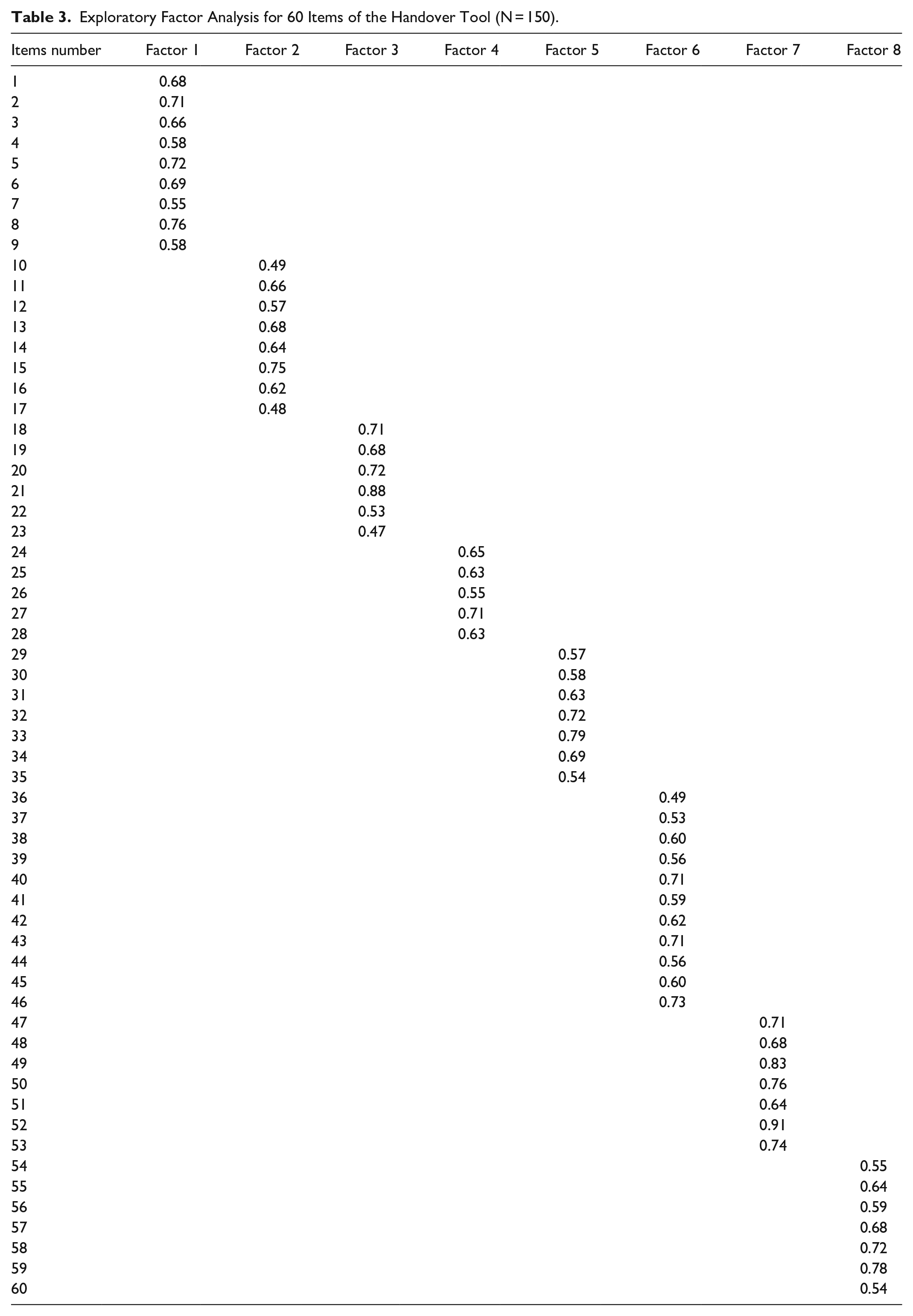
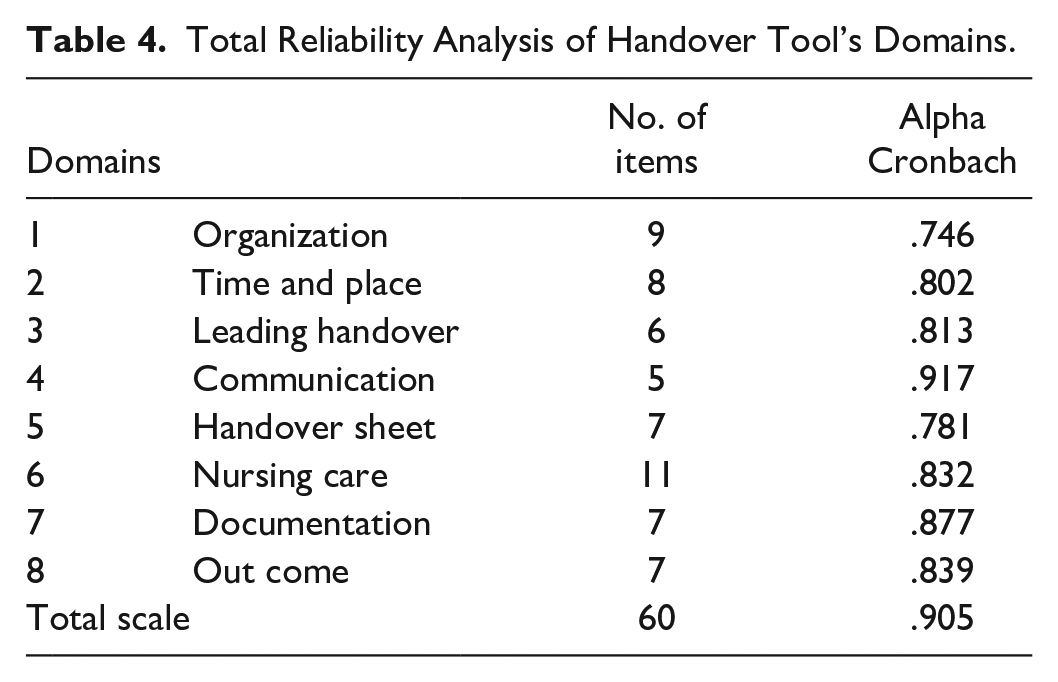
Table 4 shows that all reliability scores of all domains of the developed tool ranged between 0.746 and 0.917. The communication domain had a score of 0.917, while organization was 0.746. In addition, reliability scored as .905.
Total Reliability Analysis of Handover Tool’s Domains.
Discussion
Based on the results of our study, 12 items were excluded from the tool because their CVR ratio was less than 0.7. Therefore, after eliminating these 12 items, the number of tool items produced was 66. The KMO value = 0.713, with the recommended value being 0.6 or above. The cut-off score for the analysis model was 0.3, and the KMO value criterion was greater than 1, which defined 8 factor loadings as the best fit for the results, accounting for 69.5% of the variance.
This study was undertaken to validate a modified handover tool. Our 3-step review started by assessing the validity of the instrument’s material, assessing the degree to which each item reflected a chance to develop handover skills, and validating the revised handover. The CVR approach 20 was used to maintain tool validation among 15 experts in administrative roles and critical nursing. In addition, construct validity was established through EFA 25 and indicated an eight-factor solution, with 60 items loaded above critical level. As a result, the final version of the handover tool has 60 elements divided into 8 subscales/domains. Then, an internal consistency test was conducted using Cronbach’s alpha test for the 8 domains, with results showing that 7 domains had good reliability, while the communication domain had an excellent reliability score, as was the case in previous studies. 26 Three factors were found and extracted, accounting for 66% of the total variance. The HPT’s reliability was further tested, as evidenced by a KMO measure of sampling adequacy score of 0.793. It was revealed to have exceptional internal and inter-rater reliability.
Furthermore, a study found focus group discussions with a randomly chosen panel clarified why items were approved or rejected for the evidence-based clinical nursing handover standard. 27 An item must reach a consensus of about 70% for inclusion, and they concluded that the survey would allow the establishment of a proven nursing handover standard for use during shift changes. Handover is critical for communicating important patient information from one nursing shift to the next. 28
Similarly, a study conducted in Turkey used the English version of the Handover Evaluation Scale and contextualized it to a Turkish nursing sample, discovering that it included 10 elements and 2 variables that explained 68.96% of the total variance. 14 Furthermore, another study using the Turkish validation of the Handover Evaluation Scale found that 17 items were included in the original version and 6 items were omitted in the report. 29 As a result of the analysis structure, a one-factor scale was obtained. The result of the KMO test was 0.90, and the result of the Bartlett sphericity test was significant (P < .01). Moreover, an Italian study indicated that the Cronbach’s alpha was .79. It is thus accurate and reliable for the handover version of the CEX Italian scale and can be used to measure the efficiency of nurse handovers. 30
Conclusion
Handover is critical for communicating important patient information from one nursing shift to the next. Nurses’ safe practice can be improved by implementing standardized and structured shift handover. The aim of this work was achieved satisfactorily, as we established the validity and reliability of a handover tool formed from 60 items, with a total reliability score of .905. The Egyptian version of the handover tool is reliable and valid for shift handover between nurses. Furthermore, the method described here might be considered appropriate clinical research practice when surveying a large group of nurses and thus may allow for the transfer of the standard to other settings and provide safety for handovers.
Study Limitations
The study was conducted in only 1 setting, so further research studies are needed to assess confirmatory factor analysis for the tool with larger sample sizes in different settings. Moreover, further research is warranted on applying and developing tools to assess nurses’ competency relating to handover in ICUs.
Footnotes
Author Contributions
All authors listed meet the authorship criteria and all authors are in agreement with the content of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.