
Abstract
This study aimed to identify barriers to access to palliative care through a social mapping approach. In Colombia, the barriers to access to palliative care denote an enormous geographic disparity of resources and health needs, making it necessary to conduct community-based participatory research using an approach such as social mapping. A qualitative research design was used. Stakeholders from health insurance companies, regulatory authorities, regional health secretariats, health care professionals, patient and caregiver organizations, scientific societies, and medical journalists from 7 Colombian regions participated. It involved 3 stages. Stage 1: Semi-structured, audio-recorded interviews were conducted with 36 stakeholders and were subsequently transcribed and analyzed. Stage 2: An electronic survey was conducted to obtain feedback on the first outline of the map and the categories that emerged from stage 1. Stage 3: The nominal group technique was used to analyze and validate the barriers to access to palliative care included in the final map. The COREQ checklist was used. Twenty-seven barriers to access to palliative care related to limited availability of medications, stakeholders’ poor knowledge of regulations, limited formal education in palliative care, few patients’ support networks, patient care fragmentation, few specialized programs of palliative care, and mistaken beliefs about palliative care were identified. Stakeholders’ diverse perspectives and opinions were crucial to understanding the development of palliative care in Colombia and its challenges. Better knowledge about palliative care can open opportunities to overcome the barriers identified in this study, directly impacting access to palliative care.
Keywords
What do we already know about this topic?
In Colombia, studies on the barriers to access to palliative care indicate huge geographic healthcare disparities in terms of resources and needs, especially in pain medications and the type of care provided by specialized palliative care services in intermediate cities.
How does your research contribute to the field?
Social mapping allowed palliative care stakeholders to identify locally and nationally the barriers to access to palliative care, providing an opportunity to strengthen the voice of these participants and increase their impact as advocates to improve access to palliative care in Colombia.
What are your research’s implications toward theory, practice, or policy?
Future research should confirm the barriers to access to palliative care identified in this study through quantitative research and encourage the empowerment of patients and communities as strategic actors in palliative care development and policymaking.
Introduction
There is currently a pressing need for access to palliative care given the high burden of chronic diseases and serious health-related suffering of the population, especially in low- and middle-income countries. 1
In Latin America, palliative care has developed according to the particular conditions of each country. Most countries in the Latin American region, including Colombia, are classified as middle-income countries. 2 Currently, Colombia has 79 palliative care teams (1.60 per million population) made up of different health professionals that work with patients, families, and other doctors to meet patients’ medical, social, and emotional needs. Of these, 40 are in-hospital teams, 20 are out-of-hospital teams, 10 are mixed teams (provide in- and out-of-hospital care), and 9 are pediatric palliative care teams (0.79 per million inhabitants). 3 The average annual consumption of controlled opioids in Colombia is 556.1 kg of oral morphine equivalent (about 11.2 mg per person). 3 Colombia also has 2 national palliative care associations and different medicine, nursing, social work, and psychology programs with courses in palliative care. 3
Despite the advances of recent years, the present and future care of people with cancer or chronic degenerative diseases represent a public health challenge. Many people will reach terminal stages with intense suffering and creating a high demand for health care services due to the need not only to control symptoms but also to understand clearly the type of care these people need. 4
The World Health Organization (WHO) proposes empowering people and communities, enabling the stakeholders’ participation in the dentification of health needs, 5 and recognizing their material, social, and economic conditions in their territories as influential factors in accessing health care and palliative care. 6
In Colombia, studies investigating the access barriers to palliative care indicate a huge geographic disparity in terms of resources and needs, especially in the use of pain-relief medicines and the care specialized palliative care services in intermediate cities provide.7,8 However, none of the studies have explored stakeholders’ perceptions of these problems in the regions and the factors influencing the low national coverage of palliative care services.
Since 2016, the Colombian Palliative Care Observatory (Observatorio Colombiano de Cuidados Paliativos [OCCP] 9 ) has monitored the development of palliative care services, policymaking, medication availability, and educational programs on palliative care using indicators. However, the stakeholders’ perspective, who know the reality directly from their territories, has not been considered, and it is needed to understand better the factors that determine access to palliative care. It also provides decision-makers and health authorities with relevant information to design action plans and strategies to reduce access gaps and improve the coverage of services needed by people with palliative needs. This work aimed to examine the barriers to access to palliative care identified by different regional stakeholders using social mapping for 7 Colombian regions during 2020 and 2021.
Methods
Qualitative research has become a useful tool for stakeholders’ participation in the search for limitations and potential solutions to problems of access and inequality in health care and palliative care. 10 This work is a qualitative study with a participatory approach that used social mapping to represent stakeholders’ perspectives and analyze access to palliative care in Colombia. The consolidated criteria for reporting qualitative research (COREQ) checklist was used to assure complete reporting.
Social mapping is a participatory social diagnostic (PSD) technique that allows community members to identify their needs, analyze the causes and consequences of their problems, and determine strengths and weaknesses to find solutions. 11 Social mapping is derived from the methods of social sciences and promotes the power of collective construction and social participation, with the potential to make the phenomena experienced by particular social groups in their territories visible to public opinion. 12 It has been used in different studies in health care by summoning people to structure points of view and realities of their territories and communities.13,14 MacConville 15 conceptualizes social mapping as an approach to reveal the dynamics of patients, families, and health professionals within their historical, political, and social context and their relationship with each other. It visually expresses the complex reality of the data of specific territories and represents it on collectively constructed maps. 16
For our study, the methodology proposed by Moliner 17 was used, with the following stages: (1) Search for information: A literature review that helps conceptualize and plan the mapping activity. (2) Awareness raising: Engagement of stakeholders in the regions to participate in the study. (3) Information gathering: Interviews, discussion meetings, field notes, and surveys. (4) Data processing and analysis: Interviews transcriptions, field notes, survey results, and map drafts are the basis of the analysis. (5) Information validation: Review the information together, creating a space where participants can make comments and suggestions and add further information.
Study Participants
Convenience sampling was used in this study. By writing invitations (letters and e-mails) and phone calls, the stakeholders shown in Table 1 were invited to participate in the study.
Description of the Role of the Study Participants.
People who expressed interest and had experience and knowledge in palliative care were included in the study. People with commercial interests were excluded.
A territorial distribution by nodes proposed in previous studies on essential medications for palliative care in Colombia was used. 8 This distribution groups 1 Capital District and 32 Departments of Colombia that share similar demographic, cultural, and political-administrative characteristics into 7 regional partitions or nodes: Bogotá, the Pacific, Orinoquia, the Center, the Northeast, Amazonia, and the Caribbean. This division of the Colombian territory permits comparisons among and generalizations about the regions. Table 2 shows the profile and number of stakeholders for each regional node.
Profile and Number of Participants for Each Node.

RP = representatives of patient/caregiver organizations; MJ = medical journalists; RSS = representatives of scientific societies; HP = health professionals; RE = regulatory entities, departmental and municipal health secretariats; HIC = health insurance companies.
Conducting Social Mapping in the Regions
Initially, the social mapping construction was planned to be carried out collaboratively and in person with stakeholders and researchers. However, due to the COVID-19 pandemic, the study had to be methodologically adapted to facilitate stakeholders’ participation in the different regions using online tools and remote communication. As part of the social mapping planning, the researchers designed 3 strategies framed in 3 stages:
Stage 1: An interview guide was designed for researchers before semi-structured interviews with stakeholders occurred. The interview guide was reviewed by 3 national palliative care experts, and it included aspects related to the regional context, the demand for palliative care, the supply of resources to meet palliative care needs, and the access barriers to palliative care (See Supplemental Material 1). Some questions addressed topics like specialized palliative services, essential medicines, palliative care education, vitality, context of palliative care, and funding, which are the domains proposed by the OCCP in its model for the development of palliative care in Colombia. 9 The objective of this stage was to obtain information about the access barriers to palliative care mentioned by the stakeholders, identify categories, and develop a first version of the map.
Stage 2: A survey created in electronic form (Google Forms) was used to obtain feedback on the first outline of the map and the categories that emerged from stage 1. The objective of stage 2 was to gather information on the stakeholders’ opinions about the categories and improve the first version of the social map with this information.
Stage 3: The nominal group technique, a procedure for gathering information from groups of people who have insight into a particular area of interest, was used in this stage. 18 The nominal group consisted of health professionals from different regions who had participated in the previous stages and analyzed the results of stages 1 and 2. The objective of this stage was to identify contradictions and possible overlooked access barriers and validate the final version of the map.
Data Collection per Stage
The data collection was conducted collectively and involved regular communication with the stakeholders during the 3 proposed stages.
In stage 1, data were collected from 36 stakeholders using semi-structured interviews that lasted between 1 and 2 h. All the researchers, experienced in conducting semi-structured interviews, participated in this stage. For each regional node, at least 2 stakeholders presented in Table 1 were invited to be interviewed. The objective of the study was explained, and dates were agreed upon for online meetings with each participant so that all stakeholders were represented. For subsequent analysis, all the interviews were audio-recorded and transcribed verbatim by the researchers in MS Word. Field notes describing the researchers’ impressions of the interviews were taken during the interviews and served later to complement the analysis. Data saturation for each node was reached when the stakeholders did not provide new information that would contribute to identifying more barriers. Interviews were coded and synthesized using NVivo software. The thematic categories that emerged (pain medications, funding, public policy, education, vitality, and palliative care services) contributed to the elaboration of the first version of the social map. Traditionally, social mapping is carried out in face-to-face meetings, and the participants design and locate symbols on a map. However, given the methodological adaptation made due to the COVID-19 pandemic, the layout of the social map was made by 2 graphic designers who, together with the researchers and based on the stakeholders’ interviews, created the first outline of the map, including the thematic categories and graphic icons designed to express the essential visual characteristics of the barriers identified by the stakeholders.
In stage 2, data were collected from 29 stakeholders who participated in stage 1 using an electronic survey. The following are some of the questions asked in the survey:
Do you consider that all the barriers to access to palliative care were included in the map of your region according to the following categories (medicines, funding, public policy, education, vitality, palliative care services, and context)?
If you consider that a barrier has been omitted, please mention it below.
Do you think the map’s design adequately represents the barriers to access to palliative care in your region?
Do you think the graphic icons on the map appropriately express the access barriers in your region?
The data collected with this survey helped redesign the map and confirm the categories identified, solving contradictions among stakeholders. New access barriers were represented with new graphic icons. The categories identified (public policy, specialized palliative services, essential medicines, education, vitality, context, and funding) were used to classify the identified barriers. With the stakeholders’ feedback in this stage, the graphic designers and the researchers could produce an evolved version of the first social map.
In stage 3, data were collected during the nominal group meeting. Eight health professionals from different regions who had participated in stages 1 and 2 made up the group. They were selected by convenience, considering their professional profile (participants with experience treating patients with palliative needs and knowledge of the procedures that health insurance companies and hospitals followed) and greater participation in the previous stages of the study. The meeting involved brainstorming and making contributions to the latest version of the map and emerging categories to reach a consensus on the barriers to accessing palliative care and how to include them in the map. The nominal group meeting was recorded and transcribed verbatim in Word to implement the stakeholders’ recommendations and improve the social map.
Access Barriers Representation
Using the categories resulting from in stage 1 and the regional maps drafted in stages 1 and 2, a national map of the Colombian territory was drawn, refined with the nominal group’s recommendations in stage 3, and shared with all the stakeholders.
Data Analysis
The semi-structured interviews and field notes of stage 1 were analyzed using a thematic analysis following Andréu-Abela’s 19 proposal that develops theoretical and thematic frameworks based on the information that emerged from the data. Two researchers independently conducted the coding and categorization and subsequently collated and unified. NVivo software was used to facilitate systematization and coding.
Results of the electronic survey in stage 2 were downloaded from Google forms as a spreadsheet for further analysis. The contributions made by the stakeholders were examined and listed by topics to be included in the map.
Finally, the transcription of the nominal group session was used to identify the main ideas and contributions of the stakeholders in this stage. The comments, contributions, and adjustments made by the stakeholders were organized in a matrix to be used to produce the final social map.
Ethical Considerations
This study was approved by the Institutional Review Board at the Universidad El Bosque (UEB-2019-536). Informed consent was sent via e-mail to all participants to read and sign. If any query was raised concerning the study, it was answered by e-mail. The confidentiality of the participants was respected by using codes and no personal identifiers. Confidentiality risks of participants in the nominal group were disclosed to the participants in the informed consent as it could not be ensured that other participants would not share or disclose information after the session.
Results
The 3 stages of the study allowed the stakeholders to identify 27 barriers to access to palliative care in Colombia. Table 3 shows the barriers distributed by categories and territorial nodes consolidated in stages 2 and 3.
Barriers to access to palliative care distributed by domains and territorial nodes.
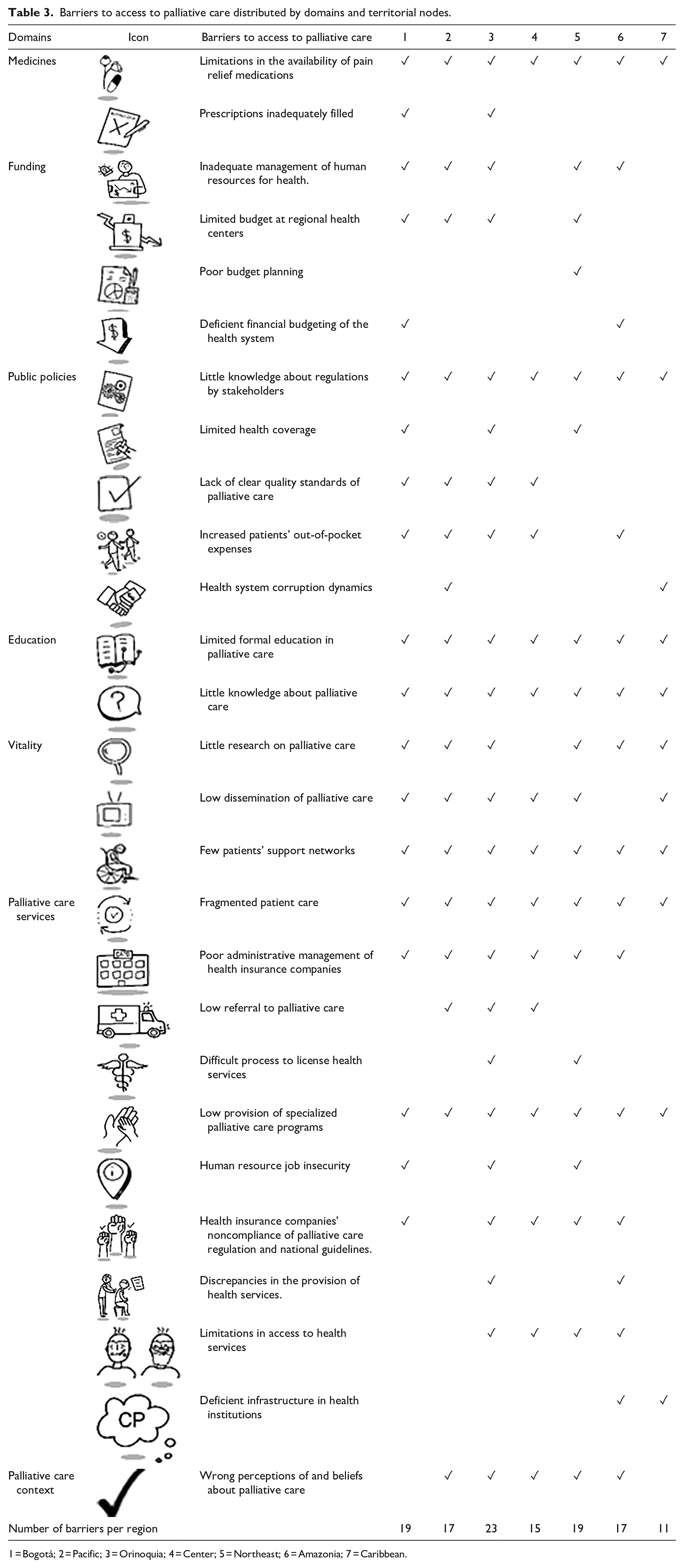
1 = Bogotá; 2 = Pacific; 3 = Orinoquia; 4 = Center; 5 = Northeast; 6 = Amazonia; 7 = Caribbean.
Seven access barriers were reported in all nodes: (1) limited availability of pain relief medications, (2) little knowledge about regulations by palliative care stakeholders, (3) limited formal education in palliative care, (4) little knowledge about palliative care, (5) few support networks for patients and family caregivers, (6) fragmented patient care, and (7) inadequate provision of specialized palliative care programs. Six regional nodes reported low research development on palliative care, low dissemination of information about palliative care, and poor administrative management of health insurance companies.
In 5 regions of the country, the stakeholders acknowledged that patients and families travel to other territories to receive palliative care. This barrier causes cost overruns in the health system and long administrative processes that delay patient care. The lack of information systems, official records, and updated clinical practice guidelines in palliative care hinder decision-making. Two access barriers related to social determinants of health showed, on the one hand, how little public discussion on palliative care had taken place and, on the other hand, the dynamics of corruption that affect the creation of health services and budget allocation. Orinoquia and northeast regional nodes reported the highest number of barriers (23 and 19, respectively). Some of the barriers to palliative care are described below in the words of the participants.
Public Policy
It involves stakeholders’ perceptions of the role of regulation and policies in promoting and accessing palliative care. 12 The barriers identified were the lack of knowledge about palliative care among citizens and some health professionals, the lack of knowledge about regulations and policies on palliative care, regulation enforcement variability in health care centers, and poor control by regulatory authorities.
“...decision makers have turned their attention to other issues and that is because there is an absolute lack of knowledge in the general population about what palliative care is.” (E9. Medical Journalist, Bogotá). “All EPS [health insurance companies] should have palliative care programs. You ask if they have a program and they say they don’t, and that is because there is no regulation monitoring us” (E20. Nurse Manager, Bogotá).
Palliative Care Services and Essential Medicines
Service provision covers the quantity of specialized pain and palliative care services, and essential medicines in palliative care address the issue of controlled opioid consumption in the country. 12 The barriers identified in these 2 categories are created by the health system (i.e., problems in working conditions, health coverage, infrastructure, equipment, socioeconomic conditions of the territories); barriers related to administrative processes carried out by health insurance companies, and health care provider centers; access barriers in rural areas; low economic resources of patients and caregivers for transportation to health care centers; lack of information about palliative care services among the population; palliative care considered as a taboo; health care focused on pain management; and poor knowledge of medications, especially opioids, among health care workers.
“Having access to opioids is very important, we only have morphine, some hydromorphone, the rest of opioids. . . so far tapentadol has arrived” (E10. Patients Association, Orinoquia node). “. . . the social conditions are difficult. Patients don’t even have money for transportation and it’s out of our hands” (E13. Health professional, Bogotá).
Vitality
Vitality involves the resources available to promote palliative care development. 12 The barriers identified were the lack of collaboration between palliative care groups and patient associations (individualized efforts), the low awareness of palliative care information systems, and the lack of creation of volunteer groups.
“. . . we don’t know if there is a consolidated working group or if they are working with us. We know professionals who deal with the subject, and we rely on them” (E1. Patients’ association, Bogotá). “. . .Volunteering in Colombia is not as well regarded as in the United States. Praising those who give hours of their time to do something positive in their community is frowned upon.” (E12. Health professional—Physician, Northeast node).
Funding
Funding involves the allocation of resources to ensure access to palliative care at all levels of the health system and the availability of regional economic resources. 12 The barriers identified were high costs in the implementation of palliative care programs by health insurance companies and health care provider centers; no budget allocations by health providers and health insurance companies for the provision of palliative care; lack of knowledge by health insurance companies and society in general about the impact of palliative care on users’ health, restrictions on access to services for a population with low income; economic difficulties of patients and families, many of them from rural areas and in high vulnerability, and acts of corruption in the health system that affect the efficient and transparent management of resources.
“. . . patients in the subsidized regime will always have more limitations. They can have their palliative care appointment in 2, 3, 4 months, but it is not authorized, or it is authorized but there is no a health care provider center that can give it” (E6. Professional association of palliative care, Center node).
Education
Education involved the inclusion of palliative care content in undergraduate medical and nursing programs and the availability of postgraduate education in medical-surgical specialties for palliative medicine and advanced education in nursing, psychology, and social work. 20
“(. . .) I think that there is a lack of knowledge about palliative care among not only patients and family members, but also the health group, and even the administration and the people who organize the political part, like mayors and governors” (E11. Health professional, Orinoquia node). “. . .In the regions, professionals feel they don’t have enough knowledge to provide care and don’t have the medications. Doctors still have as a barrier the fear of prescribing opioids” (E13. Health professional. Bogotá).
The final version of the social map was derived from the results of the 3 study’s stages and the regional maps for each node (Figure 1).
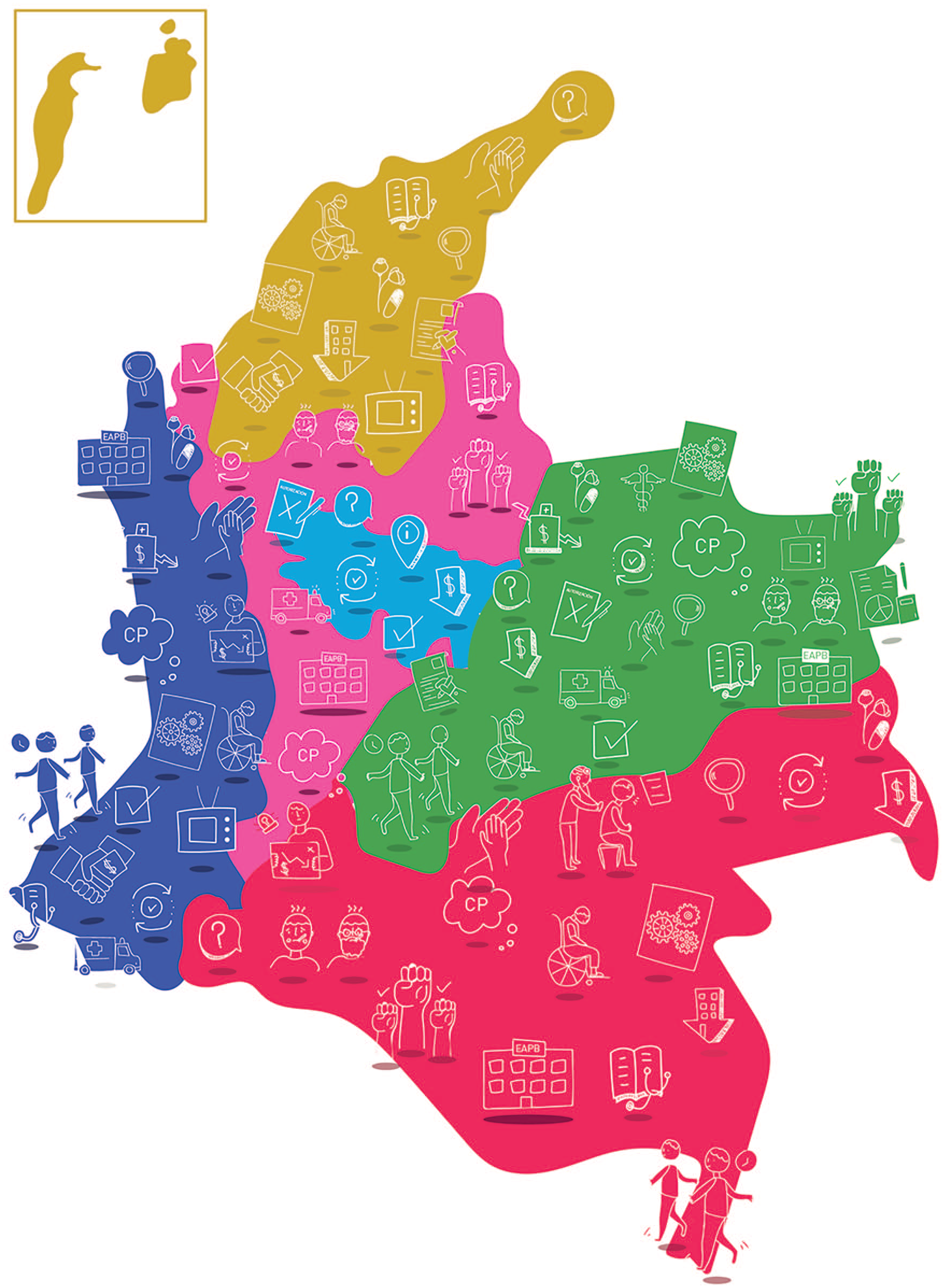
Social map of access barriers to palliative care in Colombia.
As an example of a regional map, Amazonia node’s map is presented in Figure 2.

Social map of the Amazonia node.
For an illustration of how the social maps evolved throughout the stages, see Supplemental Material 2.
Discussion
The social mapping approach allowed us to identify 27 barriers to access to palliative care in Colombia and design a social map for the country and each region to allow stakeholders to have a better understanding of palliative care. Social mapping can be used to inform the public, decision-makers, and health authorities at the national and regional levels about the problems identified in the regions and help them design strategies to reduce the gap in access to palliative care services.
The current situation of the Colombian health system affects the stakeholders’ actions so that health issues impact the development of public policies and access to palliative care, especially in peripheral and rural areas. Although Colombia has had public policies and a regulatory framework for palliative care for some years, health insurance companies have not yet taken sufficient actions to guarantee palliative care services and the availability of opioid medications in large parts of the country. 8 Consequently, stricter enforcement of the existing laws on palliative care is a priority.3,21 In Colombia, there are barriers for patients and families to whom palliative care is fragmentarily delivered. Therefore, comprehensive, multidisciplinary, culturally adapted, and more collaborative approaches are required to provide quality care.22-24
In the regions, health care services are concentrated in central and urban areas, 8 and medical specialties, such as palliative care, are scarce in peripheral areas and nonexistent in rural areas classified as “red zones” where there are no medical supplies or health personnel safety is at risk. 22 Besides, professionals usually turn down offers to occupy available positions in dangerous zones. 23 This is why health insurance companies should improve health care coverage, and the government should formulate strategies to improve health personnel’s safety in remote rural areas.
Other barriers such as the general lack of knowledge about palliative care, poor research in the field, the lack of formal education in palliative care for health professionals, and the lack of joint work between associations, patient organizations, and the community, in general, hinder meeting the patients’ palliative care needs. However, the barriers identified here are like those reported in other countries.3,24
Poor knowledge about palliative care, low dissemination of palliative care information, few patients’ support networks, and little research on palliative care have led to poor public understanding and awareness of what palliative care is. 25 This situation affects the availability of palliative care, 26 weakens community support, and prevents people from acknowledging palliative care needs.
Regarding education in palliative care, the stakeholders considered strengthening education critical to consolidating palliative care. Although the information about palliative care in Colombia has increased in recent years and contributed to advances in public policy, further action is still required. In this regard, Knaul et al 27 affirm that education of primary care providers is essential to expand access to palliative care. According to these authors, 27 health professionals, policymakers, academic institutions, and non-governmental organizations need to promote access to palliative care in both the media and policy circles; other studies’ results23,24,27 support their affirmations.
Some of the recommendations from this study include training and raising awareness of palliative care by learning about the experiences of each region, strengthening education in palliative care for health professionals, providing comprehensive services to address palliative care (involving social, emotional, family, and spiritual needs), strengthening support programs for patients and caregivers in remote areas, improving access to information on palliative care for patients and families, and strengthening e-learning for professionals and the community on palliative care.
Other recommendations included involving the community and health professionals in creating support networks and promoting work with the media to make palliative care visible locally and nationally. Academia, patient associations, palliative care organizations, and scientific societies should also collaborate and promote cost-effectiveness studies to demonstrate the impact of palliative care on reducing social and health system costs. Strengthening palliative care in primary health care and implementing risk management (outpatient and home care promotion) are also some pending tasks.
Future research should confirm the barriers to access to palliative care identified in this study through quantitative research and encourage the empowerment of patients and communities as strategic actors in palliative care development and policymaking.
This study included a significant number of participants from different regions and involved different palliative care stakeholders in identifying access barriers to palliative care. This study provided an opportunity to strengthen the voice of palliative care stakeholders and increase their impact as advocates to improve access to palliative care. This study had some limitations, however. Firstly, social mapping construction was initially planned to be carried out in face-to-face meetings, bringing together stakeholders and researchers in a community-building activity. Given the COVID-19 pandemic, methodological adaptations of the study had to be made using online tools and strategies that may have affected the participatory approach. Finally, the electronic survey used in stage 2 was not validated, or pilot tested. It was only an online tool used as a feedback strategy that was part of the methodological adaptations mentioned.
Conclusions
This study identified 25 barriers to access to palliative care in Colombia. The identified barriers are the limited availability of medications, stakeholders’ poor knowledge of regulations, limited formal education in palliative care, few patients’ support networks, patient care fragmentation, few specialized programs of palliative care, and mistaken beliefs about palliative care.
Knowledge about palliative care can open up opportunities to overcome the barriers identified in this study, directly impacting palliative care access. Stakeholders’ diverse perspectives and opinions were crucial to understanding the current situation of palliative care in Colombia and its challenges in terms of public policy that can equitably impact the country’s regions. Improving palliative care education in Colombia could help to improve the vitality, funding, public policies, service provision, and medicines of palliative care; education in palliative care could be the key to strengthening palliative care in Colombia.
Supplemental Material
sj-docx-1-inq-10.1177_00469580221133217 – Supplemental material for Barriers to Access to Palliative Care in Colombia: A Social Mapping Approach Involving Stakeholder Participation
Supplemental material, sj-docx-1-inq-10.1177_00469580221133217 for Barriers to Access to Palliative Care in Colombia: A Social Mapping Approach Involving Stakeholder Participation by Lina María Vargas-Escobar, Miguel Antonio Sánchez-Cárdenas, Angie Carolina Guerrero-Benítez, Vilma Katherine Suarez-Prieto, Jenny Rocío Moreno-García, Ángela María Cañón Piñeros, Luisa Fernanda Rodríguez-Campos and Marta Ximena León-Delgado in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580221133217 – Supplemental material for Barriers to Access to Palliative Care in Colombia: A Social Mapping Approach Involving Stakeholder Participation
Supplemental material, sj-docx-3-inq-10.1177_00469580221133217 for Barriers to Access to Palliative Care in Colombia: A Social Mapping Approach Involving Stakeholder Participation by Lina María Vargas-Escobar, Miguel Antonio Sánchez-Cárdenas, Angie Carolina Guerrero-Benítez, Vilma Katherine Suarez-Prieto, Jenny Rocío Moreno-García, Ángela María Cañón Piñeros, Luisa Fernanda Rodríguez-Campos and Marta Ximena León-Delgado in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-2-inq-10.1177_00469580221133217 – Supplemental material for Barriers to Access to Palliative Care in Colombia: A Social Mapping Approach Involving Stakeholder Participation
Supplemental material, sj-jpg-2-inq-10.1177_00469580221133217 for Barriers to Access to Palliative Care in Colombia: A Social Mapping Approach Involving Stakeholder Participation by Lina María Vargas-Escobar, Miguel Antonio Sánchez-Cárdenas, Angie Carolina Guerrero-Benítez, Vilma Katherine Suarez-Prieto, Jenny Rocío Moreno-García, Ángela María Cañón Piñeros, Luisa Fernanda Rodríguez-Campos and Marta Ximena León-Delgado in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors thank participants and colleagues for their active support during this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Open Society Foundation [grant number OR2019-64290].
Ethical Considerations
This study was approved by the Institutional Review Board at Universidad El Bosque (UEB-2019-536). Informed consent was sent via e-mail to all participants to read and sign. If any query was raised concerning the study, it was answered by e-mail. The confidentiality of the participants was respected by using codes and no personal identifiers. Confidentiality risks of participating in the nominal group were disclosed to the participants in the informed consent as it could not be ensured that other participants would not share or disclose information after the session.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.