
Abstract
Public health insurance eligibility for low-income adults has improved adult economic well-being. But whether parental public health insurance eligibility has spillover effects on children’s health insurance coverage and family health-related financial well-being is less understood. We use the 2016 to 2020 National Survey of Children’s Health (NSCH) to estimate the effects of Medicaid expansions through the Affordable Care Act (ACA) for parents on child health insurance coverage, parents’ employment decisions due to child health, and family health-related financial well-being. We compare children in low-income families in states that expanded Medicaid for parents after 2015 to states that never expanded in a difference-in-differences framework. We find that these expansions were associated with increases in children’s public health insurance coverage by 5.5 percentage points and reductions in private coverage by 5 percentage points. We additionally find that parents were less likely to avoid changing jobs for health insurance reasons and children’s medical expenses were less likely to exceed $1000. We find no evidence that the expansions affected children’s dual coverage and uninsurance. Our estimates are robust to falsification and sensitivity analyzes. Our findings also suggest that benefits on children’s medical expenses are concentrated in the families with the greatest financial need.
Keywords
Public health insurance eligibility for low-income adults has improved adult economic well-being.
We examine if parental public health insurance eligibility has spillover effects on children’s health insurance coverage and family health-related financial well-being.
Our study demonstrates the benefits of public health insurance expansions for families with children and suggests that the benefits of lower children’s medical expenses may be concentrated in the families with the greatest financial need.
Introduction
Prior to the Affordable Care Act (ACA) Medicaid expansions, 36% of families experienced health-related financial burdens, such as problems paying medical bills. 1 Health-related medical expenses comprise a substantial portion of a household’s expenses and can pose a significant financial burden on families, 2 particularly those with children and low-incomes.1,3 Health-related burdens can also restrict adults’ ability to change jobs due to preexisting conditions or need to maintain employer sponsored health insurance coverage, a phenomenon known as job lock.4,5
The Medicaid program has long offered public health insurance coverage to very low-income adults. Before the ACA, affordable health insurance coverage options were limited for low-income families ineligible for Medicaid. The ACA provided federal funds to states to expand existing Medicaid eligibility to nonelderly, non-disabled adults with incomes below 138% of the federal poverty line (FPL). Additionally, the ACA marketplaces enabled uninsured adults without employer sponsored insurance to purchase insurance with income-related subsidies. The effect of these Medicaid expansions has been studied extensively, with evidence that they improved adults’ healthcare coverage and access, finances, and health.6-9 Specifically, the expansions reduced healthcare related strain, 10 out-of-pocket expenses for medical care,11-13 medical bills, 14 and the probability of bills going to collections. 15 The expansions also reduced unpaid bills and general debt, prevented delinquencies, and improved credit scores,16,17 and reduced the use of payday loans15,18 and fringe banks. 19 The expansions also improved housing and food security.20-22
The existing literature has primarily focused on “childless adults” (i.e., those without dependent children). However, the ACA Medicaid expansions also changed eligibility thresholds for low-income parents and is credited with reducing uninsurance rates among parents from 18% in 2013 to 11% in 2017. 23 The changes to the Medicaid program for parents varied across states due to different state-level income thresholds prior to the ACA. Among the 3 expansion states examined in this study, the income eligibility limits for working parents for Medicaid pre-ACA as percent of the FPL were: 24% in Louisiana, 52% in Virginia, and 105% in Maine. Following the ACA Medicaid expansions, the income eligibility limit increased to 138% FPL in each of these states.
The goal of this paper is to determine whether these expansions in Medicaid eligibility for parents impacted their children’s public health insurance coverage and their families’ health-related employment decisions and financial well-being. We contribute to the existing literature by (1) focusing specifically on parents, (2) examining employment decisions specifically due to child health reasons and child-specific medical expenditures, and (3) providing evidence on late Medicaid expansion states. We use child-level data from the National Survey of Child Health (NSCH) 47 to compare Medicaid-eligible households in 3 late expansion states (i.e., those that expanded between 2016 and 2019) to those in non-expansion states. a The strength of the NSCH is that it provides children’s health insurance coverage status, precise income measures, and detailed measures of families’ healthcare costs and decision making. We examine contextual measures of health-related financial well-being, including parent employment changes due to health issues or insurance (i.e., job lock) and high child medical costs.
Consistent with previous research, 24 we find that the Medicaid expansions for low-income parents were associated with increases child public health insurance coverage. Our estimate is remarkably similar to previous research, documenting increases of 5.6 percentage points (or about 8.5%) compared to Hudson and Moriya’s 24 estimate of 5.7 percentage points (8.1%). In contrast to their findings of no significant change in private coverage, however, we find evidence of crowding out private insurance; children’s private insurance coverage declined by 4.9 percentage points (30%).
As a new contribution to the literature, we also find a reduction of about 4.5 percentage points (roughly 55%) in the likelihood that parents avoid changing jobs for reasons related to health insurance. Finally, we find the likelihood of a child’s out-of-pocket medical expenses exceeding $1000 is 4 percentage points lower, a 70% decline, suggesting the benefits of children’s health-related financial expenses are concentrated in the highest medical expense population. We do not find significant effects of the ACA Medicaid expansions on a child having both private and public insurance (dually covered) or being uninsured. Taken together, these findings demonstrate the spillover effects of the Medicaid expansions to children’s health insurance coverage, parents’ employment, and family financial well-being.
Background
A primary goal of health insurance is to smooth the financial risk associated with poor health outcomes. There are several potential mechanisms through which the ACA Medicaid expansions may influence health-related financial well-being among families. First, expanding public health insurance programs to parents has been shown to increase health insurance coverage of both parents25,26 and children through “welcome mat” effects.24,25 Health insurance rates among children have steadily increased over the past several decades in response to state expansions of coverage for children through Medicaid and the Children’s Health Insurance Program (CHIP). 27 In 2016, at the start of this study, 95.5% of children in the U.S. had public or private health insurance. 28 Yet, research has shown that the Medicaid expansions increased public health insurance coverage for children who were already eligible for coverage, but not yet enrolled. 24 Public health insurance expansions may also crowd out private insurance coverage due to Medicaid’s substantially lower premiums and copays than private insurance, which may improve the financial well-being of low-income families.
Research has documented the financial benefits that come with health insurance coverage.10,14 Indeed, the ACA expansions have reduced financial burdens of healthcare costs among families with children.26,29,30 For example, Wisk and colleagues 30 found that low- and middle-income families who were eligible for Medicaid and insurance subsidies through the ACA Medicaid expansions experienced greater reductions in healthcare–related financial burden after the ACA was implemented compared to families with higher incomes. They were unable to account for state-specific ACA Medicaid expansion policies, however. Similarly, McMorrow and Kenney and colleagues26,29 found that low-income parents reported fewer problems in paying family medical bills due to expanded Medicaid coverage.
Second, the documented improvements in health among beneficiaries of the ACA Medicaid expansions may indirectly have implications for financial stability. For example, the expansions have been linked to adults’ physical health,14,31 including parents,26,32 and behavioral health.33-36 Bullinger 37 also finds improvements in child support payments. Together, this literature implies that the expansions created more financial security and stability among low-income parents.
Third, the ACA Medicaid expansions may have benefited adults by reducing job lock.4,5 With a few exceptions,38,39 research on adults (not parents specifically), however, has largely found that the ACA expansions did not result in changes in employment, job switching, or reduced work hours.38,40-43 Previous Medicaid expansions for parents during the 1990s have been linked with reductions in job, 44 though no known research has examined this question among parents in relation to the ACA expansions. The distinction between adults and parents may be important since parents have unique motivations for seeking certain types of employment and schedules due to caretaking responsibilities.45,46 Understanding whether parents are more sensitive to changes in health insurance eligibility because of the ACA in comparison to prior expansions (e.g., Hamersma and Kim 44 ) is important for policy.
Taken together, evidence shows that the ACA Medicaid expansions had positive benefits for adults’ financial well-being,6,7 however less research exists explicitly on adults with dependent children. Among these parents, there are similar and unique mechanisms through which the expansions may have impacted health-related financial well-being, including changes in child health insurance coverage, child health related costs, and employment changes. We contribute to the existing literature by examining the effects of parental public health insurance eligibility on child health insurance coverage, parents’ employment decisions due to child health reasons, and family health-related financial well-being.
Methods
Data
We use the 2016 to 2020 waves of the National Survey of Children’s Health (NSCH). 47 The NSCH is a nationally representative survey of households with children aged 0 to 17 directed by the Health Resources and Services Administration’s Maternal and Child Health Bureau. 47 The repeated, cross-sectional survey includes robust information on children’s health and well-being including health insurance coverage, healthcare access, and medical costs, as well as household income and state of residence. We pair child-level data from the NSCH with state-level Medicaid policies from Kaiser Family Foundation 48 to determine parental eligibility for Medicaid through the ACA.
Sample
Due to the available data in the NSCH, we first limit the analytic sample to children residing in states that expanded between 2016 and 2019 and states that had not expanded by 2020. We exclude children in states that expanded prior to 2016 to avoid potential dynamic effects of the expansions from those earlier expanding states. b
The parental eligibility thresholds for Medicaid differed across states prior to ACA, as well. Therefore, we next limit the sample to children in households with incomes below their time-variant, state-specific eligibility thresholds to precisely capture children in households who would have been newly affected by the ACA Medicaid expansions. c For example, in Virginia, parents whose household income was less than 38% of the FPL were eligible for Medicaid prior to the ACA expansions. In Maine, the threshold was much higher pre-expansion: 105%. Upon expanding their Medicaid programs through the ACA, all adults whose household income was less than 138% of the FPL became eligible. Most non-expansion states had eligibility thresholds below 50% FPL. Therefore, before the expansion, households with incomes below these thresholds are in the sample, while after expansion households with incomes below 138% FPL are in the sample in expansion states. In non-expansion states, the sample consists of households with incomes 102% FPL or less (depending on the state and year, see Figure 1). In Supplemental analyses, we test the sensitivity of the results to alternative samples.

Conceptual Map of Treatment and Comparison Groups.
Measures
We focus on 2 sets of outcomes in this study: (1) health insurance coverage for children and (2) family health-related financial wellbeing due to children’s healthcare use. All measures are at the child-year level from the NSCH data.
Health insurance coverage
In each year of the survey, parents are asked how the child is currently insured. We code this measure as 4 mutually exclusive binary indicators (publicly; privately; both publicly and privately; or not insured) equaling 1 if the parent responded yes (Yes = 1; 0 = No). d
Health-related financial wellbeing outcomes
We use 2 measures to assess family’s health-related, financial outcomes. Each year of the survey, parents reported (a) whether they or other family members avoided changing jobs because of concerns about maintaining health insurance for the focal child in the last 12 months (Yes = 1, No = 0); and (b) their out-of-pocket medical costs for the child’s medical, health, dental, and vision care in the past 12 months in 5 categories (1 = $0, 2 = $1-$249; 3 = $250-$499, 4 = $500-$999, 5 = $1000-$5000, 6 = More than $5000). e Following previous literature on the topic,49-52 we recoded this variable to a binary indicator (1 = $1000 or more; 0 = Less than $1000). f
We also adjust for several child- and family-level covariates (sex, race/ethnicity, and others) guided by past literature linking children and parents’ health insurance status. 53 We also adjust for several state-level time-varying characteristics (e.g., unemployment rates, Earned Income Tax Credit rates, and others) that may differentially affect the outcome measures across states (see Table 1 and Appendix A for a description of control variables).
Descriptive Statistics.

Source. NSCH 2016 to 2020.
Note. Sample consists of households with incomes at or below their state’s parental eligibility thresholds. Descriptive statistics are not weighted due to limits on the analytic sample.
Statistical Analysis
Originally, the ACA required all states to expand Medicaid to all adults below 138% of the FPL. However, in 2012, the Supreme Court allowed states to opt out of this requirement. As a result, to date, 39 states including Washington, D.C. have expanded Medicaid, a largely political decision. 54 Most states expanded in 2014, though some expanded later. We restrict our analysis to states that expanded in 2016 or later and those that did not expand at all due to lack of comparable NSCH data prior to 2016. See Appendix B for the timing and expansion status for these states.
We use this variation in the state-level ACA Medicaid expansions between 2016 and 2020 to identify the effect of parental Medicaid eligibility on children’s health insurance coverage and parents’ health-related financial wellbeing. We compare changes in outcomes between eligible parents residing in states that expanded to eligible parents in states that did not expand using a difference-in-differences (DD) approach. Therefore, we compare eligible parents in the expansion states to always eligible parents in the comparison group. See Figure 1 for a conceptual description of the treatment and comparison groups. g
Specifically, we estimate the following baseline linear probability model using OLS estimation h :

Where Yisy is the outcome for child i, living in state s, during year y. Expansionsy = 1 if child i lives in one of the 3 states that expanded between 2016 and 2019 (Louisiana, Virginia, and Maine), and 0 if the child resides in a non-expansion state. For non-expansion states, the pre-ACA parental income eligibility threshold is also the contemporaneous threshold.
Because the analytic sample is made up of only 18 states, we cannot rely on standard clustering of the standard errors at the state level. 55 The standard errors will be artificially low, leading to over-rejection of the null hypothesis of no effect, thereby finding an effect when there is none. Instead, we implement a wild cluster bootstrap with 1000 replications, which provides more reliable standard errors for inference when there are too few clusters.56-60
Results
Descriptive Statistics
Table 1 reports the means across treatment and comparison states, before and after expansion (years 2019-2020 for non-expansion states). The DD approach we employ relies on changes in trends across these 2 groups to isolate the effects of the policy; therefore, the differences in levels across these groups of states are not problematic per se. In Figure 2, we visually present the raw trends in the primary outcomes of interest between 2016 and 2020 comparing expansion states by date to non-expansions. i These trends are approximately similar.
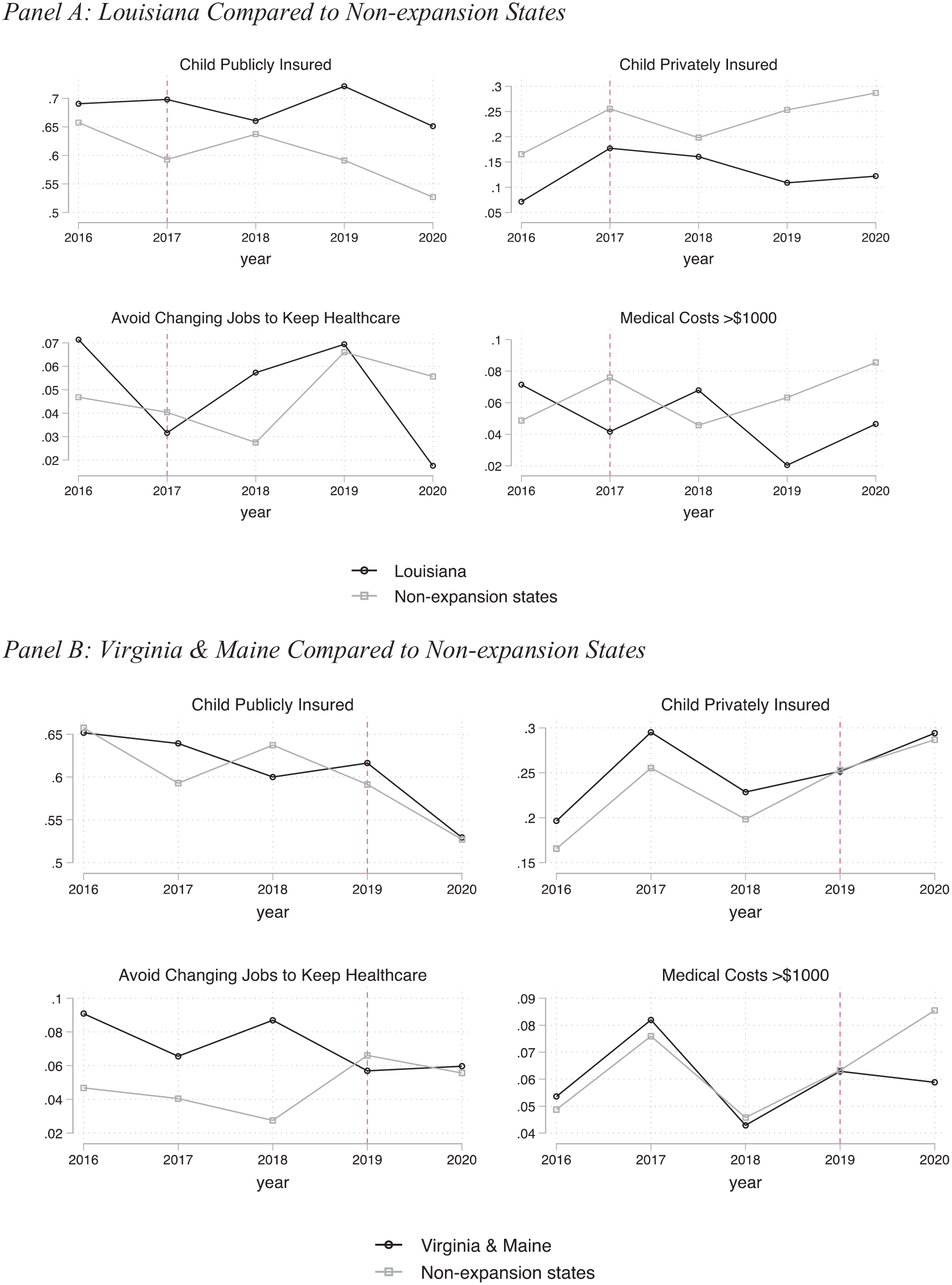
Raw trends in outcomes: Panel A: Louisiana compared to non-expansion States and Panel B: Virginia and Maine compared to non-expansion States.
Effects of the Expansions on Child Insurance Coverage, Parents’ Employment Decisions, and Family Health-Related Financial Well-being
We present the main results in Table 2 with each column of each panel corresponding to a different regression, as specified in equation (1). We report the coefficients of interest (
Full Analytical Sample of Children.

Source. National Survey of Children’s Health, 2016 to 2020 47 ; Kaiser Family Foundation. Sample consists of children in households eligible for Medicaid according to state income thresholds.
Notes. P-values in parentheses, significance stars omitted due to differences in analytical standards. Wild bootstrap P-values < .10 are bolded. Expansion = 1 if child’s state expanded Medicaid between 2016 and 2019, and the survey year = post expansion. Expansion = 0 if child’s state never expanded, pre-expansion for expansion states, and for 2020 expansion states (Utah and Idaho). Early, on-time, and other late expanders that expanded before 2016 were dropped. Regressions adjust for child’s sex, race/ethnicity, and age, whether child is less than 6 months of age, whether there are 3 or more children in the household, mother’s marital status, education level, and employment status, and whether the household speaks English as first language, state unemployment rates, state Earned Income Tax Credit (EITC) rates, whether EITC is refundable, state minimum wages, and the maximum Temporary Assistance for Needy Family (TANF) and Supplemental Nutrition Assistance Program (SNAP) combined benefits for a family of 3. 99% of publicly insured children are covered by Medicaid or CHIP.
Next, we observe a similarly sized absolute decrease in children’s private health insurance coverage: 4.9 percentage points. Because of the smaller base, however, this relative change is much larger: about 30% (P < .10). This finding suggests a crowd-out of private health insurance by public insurance. We do not observe any statistically significant effect of parental Medicaid expansions on dual insurance coverage (both private and publicly insured children) or on uninsurance.
Panel B shows the results for the medical-related financial well-being measures (job lock and high medical expenses). We find that parents are 4.6 percentage points (or about 55%) less likely to avoid job changes due to worries about losing employer-provided health insurance for their child (P < .10). Finally, the estimate is negative and statistically significant for children’s out-of-pocket medical costs exceeding $1000 a year implying decreases in the likelihood of families experiencing very high healthcare costs related to children. Specifically, we observe a 4-percentage point decrease in the likelihood of incurring medical costs for the focal child that exceeds $1000, which represents an approximately 71% decrease relative to the mean of 6% (P < .10). This large effect may suggest that the largest financial benefits of the expansions are concentrated among families with the greatest healthcare expenses. k
Sensitivity Analyses
We conduct a falsification test on a group of children unexpected to be affected by the ACA’s Medicaid expansions that targeted low-income families. Specifically, we estimate our baseline model specification (1) on children from households with reported income equal to or greater than 400% FPL. As expected, Table 3 shows no significant change in children’s public insurance coverage or other health-related financial wellbeing outcomes for this group. The magnitude of the coefficients is also close to 0 for all outcomes, which bolsters confidence in the baseline results. Our results are also robust to alternative sample construction and model specifications (see Appendix D for Supplemental analyses).
Falsification Test: High-Income Sample of Children (≥400 FPL).

Source. National Survey of Children’s Health, 2016-2020 47 ; Kaiser Family Foundation. Sample consists of children in households with incomes > 400% FPL.
Note. P-values in parentheses, significance stars omitted due to differences in analytical standards. Wild bootstrap P-values < .10 are bolded. Expansion = 1 if child’s state expanded Medicaid between 2016 and 2019, and the survey year = post expansion. Expansion = 0 if child’s state never expanded, pre-expansion for expansion states, and for 2020 expansion states (Utah and Idaho). Early, on-time, and other late expanders that expanded before 2016 were dropped. Regressions adjust for child’s sex, race/ethnicity, and age, whether child is less than 6 months of age, whether there are 3 or more children in the household, mother’s marital status, education level, and employment status, and whether the household speaks English as first language, state unemployment rates, state Earned Income Tax Credit (EITC) rates, whether EITC is refundable, state minimum wages, and the maximum Temporary Assistance for Needy Family (TANF) and Supplemental Nutrition Assistance Program (SNAP) combined benefits for a family of 3. 99% of publicly insured children are covered by Medicaid or CHIP.
Discussion
In this paper, we examine the short-term effects of expanding public health insurance eligibility for low-income adults on children’s public health insurance coverage, parents’ employment decisions, and low-income households’ health-related financial well-being as it relates to their children. We use data on children from low-income families to isolate a targeted sample of children whose parents were eligible for Medicaid through the ACA’s Medicaid expansions beyond 2015. These data provide detailed measures of child health insurance coverage and health-related financial well-being, enabling us to examine several specific mechanisms highlighted by theory and prior research.26,61-63 We contribute to the existing literature, which has primarily focused on “childless adults,” to understand the implications of the ACA Medicaid expansions on the health-related financial well-being of families with children.
First, we found that the ACA Medicaid expansions for low-income parents between 2016 and 2019 were associated with increases children’s public health insurance coverage by 5.6 percentage points (about 8.5%). Our findings are consistent with past literature on the welcome mat effects of public health insurance expansions for adults for already eligible children.24,64 Specifically, to put this in context with prior work, using data from the American Community Survey, Hudson and Moriya 24 estimate a welcome mat effect of 5.7 percentage points (8.1%) for children as a result of the ACA expansions to adults. l In contrast to Hudson and Moriya & Moriya, 24 however, we find stronger evidence of public health insurance crowding out private insurance; children’s private insurance coverage declined by 4.9 percentage points (30%). These results call for an ongoing monitoring and research of public and private coverage options among low-income families and their associated trade-offs as suggested by prior literature. 65 Findings imply that policies that expand parents’ public health insurance eligibility can have a significant impact on children’s health insurance coverage, and that these effects extend to late-expansion states.
Second, we find that the expansions lowered the financial burden of low-income families by reducing parental job lock and out-of-pocket medical costs for children’s healthcare. Specifically, the ACA Medicaid expansions for low-income parents reduced the likelihood that parents avoid changing jobs for reasons related to health insurance by about 4.5 percentage points (roughly 55%). This finding is consistent with Hamersma and Kim 44 who examine earlier Medicaid expansions for parents. It differs, however, from other work using ACA insurance policies. For example, Callison and Sicilian and Sicilian 38 find mixed effects of the expansions on labor market outcomes based on race/ethnicity and gender. When examining the ACA’s young adult mandate, Bailey and Chorniy 40 find no effects on job lock while Kofoed and Frasier 39 show reductions in job lock among enlisted soldiers in the U.S. Army. These differences suggest that parents are more sensitive to changes in health insurance eligibility when it comes to job mobility.
Finally, these expansions reduced the likelihood of these families incurring high ($1000 or more per year) child medical costs by 4 percentage points. Health-related financial burdens are notable among low-income families.1,3 Previous research has documented that the ACA expansions reduced healthcare related financial strain, 10 yet this research was not specific to parents nor to child medical costs. Additional research focusing on households with children found the ACA reduced healthcare-related financial burden, 30 but was unable to separate the role of Medicaid expansions from other health insurance provisions (e.g., the ACA marketplace) or child medical expenses from other household members. Our findings suggest that there were financial benefits for low-income families in late-expansion states through reductions in high child medical bills, and that these financial burdens are lowered primarily for high medical expense households. The results suggest that policies that expand low-income parents’ public health insurance eligibility may reduce parents’ high child medical expenses, especially among families with higher expenses.
Limitations
We use a quasi-experimental design to estimate the effect of adult Medicaid eligibility rather than a random assignment experimental design. There may be omitted, time-varying variables that are correlated with both our financial well-being outcomes and whether a state expanded their Medicaid program. We use strategies to reduce this concern, including the use of a control group of states, state and wave fixed effects, and adjusting for child- and family-level covariates and state-level time-varying characteristics. We also estimate several alternative sample construction and model specifications (including wild cluster bootstrap methods), and multiple placebo checks.
Similarly, robust, closed-form, power formulas for observational studies, such as the quasi-experimental DD analysis we conduct in this study, are not readily available. 66 We conducted a post-hoc power calculation using emerging guidance 67 and find that we are sufficiently powered to estimate minimum detectable effect size (MDE) in the ballpark of what prior literature shows. m
Finally, all measures used in this study are self-reported. As an example, respondents may misreport public health insurance coverage as private. In this case, we also examined dual enrollment and uninsurance, but future research should examine more objective measures of families’ health-related financial well-being. Lastly, we have between 1 and 3 post-expansion waves in the dataset, varying by the state. Therefore, our results reflect only short-term effects. Further research should examine the long-term effects of the ACA Medicaid expansions on parents and their families.
Conclusions and Implications
Our findings indicate that the ACA Medicaid expansions had important positive benefits for parents and children. Households experienced less parental job lock due to child health reasons and lower medical financial burden, particularly among high medical expense children. Our study adds to the accumulating evidence of the role of public health insurance expansions on health-related financial well-being,3,6 and highlights the “missed opportunities” 26 for low-income parents in non-expansion states.
Furthermore, recent research has shown that many states that expanded Medicaid under the ACA were able to do so without substantial increases in administrative spending. 68 Indeed, studies are uncovering other benefits for hospitals in states that are yet to expand, which include potential savings from lower costs of treatment and reduced costs of uncompensated care attributed to uninsured patients. 69
Finally, research has documented the long-run benefits of health insurance coverage70-73 and household financial well-being 74 for children’s health and developmental trajectories. This study suggests that it might be better late than never when it comes to states adopting the ACA Medicaid expansions, given that positive benefits might continue to accrue into the future.
Footnotes
Appendix A: Description of Covariates in Analysis
Appendix D. Supplementary Analyses
The main analytical sample consists of only children in households whose parents were eligible for Medicaid based on their state’s income thresholds. Though inclusion in the sample is based upon state Medicaid policy decisions (rather than individual characteristics), one potential concern in using this approach is if any observable effects are driven by changes in sample composition across time and within state. In other words, we want to be certain that any observed effects are only because of the change in the eligibility threshold (% FPL) in the expansion states at the time of the expansion. Therefore, we perform a robustness check where we include in the sample children in households with incomes between state-specific thresholds and 138% FPL in control states in 2019 and 2020 (i.e., households between 50 and 138 in most control states). This exercise tests whether including slightly higher income households in the treatment states post expansion is driving the effects. Appendix D1 shows a conceptual figure of this sample construction. Appendix D2 erports the descriptive statistics for this alternate sample, and Appendix D3 reports the results. The results are slightly attenuated, though substantively the same. These findings offer evidence that the observed effects are not due to differences in people at the newly eligible thresholds, but rather due to the state-specific policy changes.
Next, Utah and Idaho both expanded their Medicaid programs to 138% FPL with enrollment beginning in January 2020. In the main results, we treat them as non-expansion states since some outcomes inquire about the past 12 months and effects would likely be attenuated for the questions asking about current status (e.g., child health insurance coverage). In a robustness check, we drop these 2 states entirely. As seen in Appendix D4, this decision is not consequential for the results. The coefficient estimates are nearly identical, though slightly less precise. The reduction in precision is likely due to dropping 2 out of 18 clusters in the wild cluster bootstrap.
Finally, to examine if a single expansion state has a stronger influence on the average effects, we perform a “leave one out” analysis. Specifically, we drop observations from each expansion state from the analysis sequentially to determine the sensitivity of the results. These results are in Appendix D5. Due to limited statistical power, the effects are imprecise. However, the point estimates are consistent across all models providing suggestive evidence that the benefits were widely shared in each of these late-expansion states.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.