
Abstract
North-South partnerships have been identified as one way of solving some of the challenges in health sectors globally. Norway and Malawi have one such partnership in trauma and emergence care. Lack of trauma care and emergency medicine is a major public health concern worldwide. This results in substantial loss to individual, families, and society. The study follows this partnership between Norway and Malawi, investigating on its socio-cultural benefits, and on how this contributes to the health professionals’ cultural competence. A qualitative case study was chosen for this study, 20 semi-structured interviews were conducted with health professionals and coordinators of the program. Interviews were conducted digitally using platforms such as Zoom and WhatsApp. Interviews were collected between the period of December 2020and February 2021. We found out that exchange participants from both countries largely reported positive experiences. Their experiences centered around their interactions and encounters with patients, patients’ relatives, and colleagues at host institutions. Participants reported a better understanding on health seeking behaviors in different contexts, the importance of communication with both patients and colleagues, and teamwork. In addition, the study revealed the importance on perceptions around identities such as race and gender and how these impact on health professionals’ interactions with patients. We also found out that although working in a different socio-cultural environment was reported as challenging, it was experienced as enriching and rewarding in terms of building and developing cultural competence. The study concludes that North-South health professionals exchange partnerships can be a viable vehicle for developing and naturing cultural competence in health professionals, however, such programs need to invest in preparing the exchange participants to be ready for the challenges that lies ahead in host institutions and countries.
Keywords
We know that partnerships are central in addressing the pressing challenges we face in global and public health, and we also know that partnerships can contribute to social-cultural aspects of care.
Our research focuses on the socio-cultural benefits of health exchange programs and not the traditional subject of technological and expertise contributions of such partnerships.
The research is significant because it shows evidence that health exchanges programs can be beneficial to both countries in the global south and north, which is a significant move away from the belief that such partnerships largely benefits countries in the global south as they gain technology and expertise in trauma and emergency care. Countries like Norway who are in the wave of multiculturalism benefit from such programs in building and strengthening the cultural competencies of their health professionals.
Introduction
This article explores the contribution of North-South partnerships in the building and strengthening of cultural competence in health professionals. The study uses a case of trauma and emergency care professionals on an exchange partnership between Kamuzu Central Hospital (KCH) of Malawi and Haukeland University Hospital (HUH) of Norway to elucidate on this phenomenon.
Lack of trauma care and emergency medicine is a major public health concern worldwide which results in substantial loss to individuals, families, and society.1,2 According to WHO 2 the unavailability of proper trauma care and emergency medicine results in health conditions that account for more than half of deaths in low- and middle-income countries including Malawi. In sub-Saharan Africa, trauma is a leading cause of mortality in people less than 45 years. 3 Due to unavailability and inaccessibility of emergency medicine and trauma care, post-traumatic stress disorder, and disabilities become a major public health burden. 4 It is estimated that 45% of deaths and 35% of disabilities related to injury 5 can be addressed by developing comprehensive trauma and emergency care systems which unfortunately remain out of reach for many people in low-and middle-countries. 6 This challenge is seriously compounded by the lack of a competent health personnel, both with regards to medical and professional training and in relation to the understanding of social and cultural factors which play a significant role on whether people decide to seek care or not. This lack of social, cultural, and other competencies in health professionals, creates an even bigger barrier not only to comprehensive quality health care provision, but also to efforts to reduce mortality.7,8
In recent global health interventions, there is recognition that sustainable action requires both local collaboration and global partnership efforts in all areas, including in trauma care and emergency medicine.9-11 The exchange partnership by Malawi and Norway thus, need to be seen as complementary to already existing global efforts.
While this partnership between Malawi and Norway is largely defined in terms of technological and expertise exchange,12,13 which in this understanding and strict definition makes this partnership more beneficial to Malawi than Norway, the partnership can also be seen in terms of socio-cultural benefits to the health professionals as working in a different social and cultural context can contribute to strengthening their cultural competence. Culturally responsive and sensitive health systems are now being significantly considered as central in solving inequalities in health care provision. 14 In the context of Norway, this is a dimension where the country can also significantly benefit from such North-South partnership as Norway until recently has been a largely homogenous country. 15 While multiculturism is slowly becoming a norm in Norway, the transition requires all its sectors, including the health sector to have culturally competent professionals to meet the needs of a diverse population.
Different approaches to ensuring culturally sensitive health systems and practices are suggested within the existing literature. For example, some scholars further describe these in the context of cultural humility, 16 cultural safety and cultural competence. 14 All these suggests deeper recognition and inclusion of socio-cultural factors, the indigenous communities, and a large growing diverse and multicultural population. This study therefore aims to investigate on how North-South partnerships can contribute to the strengthening of cultural competence in health professionals.
Theoretical Frameworks
The study used the cultural competence model 17 in examining the socio-cultural components of the health collaborative partnership. The models allow for a deeper exploration of how participants’ encounter and dealt with a different socio-cultural context and how these experiences shaped and contributed to their cultural competence.
Cultural competence is an ongoing process in which health care providers continuously strive to achieve the ability to understand and work effectively within the cultural context of individuals, families, communities and countries. 17 Culture is defined here as values, beliefs, customs, traditions, patterns of thinking, norms, and mores of individuals or populations 18 and health professionals’ ability to work in these diverse socio-cultural realities and with people of diverse backgrounds is what is referred to as cultural competence. In this study, the health collaborative exchange between Kamuzu Central Hospital and Haukeland University Hospital is one of many efforts in the global context to enhance the cultural competence of health professionals.
The cultural competence model consists of 5 dimensions, which are: cultural awareness, cultural knowledge, cultural skill, cultural encounters, and cultural desire. 17 Cultural awareness refers to self-awareness on one’s own cultural views and the impact it can have on self and biases on the worldview. When one is not aware of the influence of one’s own cultural or professional values, there is risk that a health provider may engage in cultural imposition. 17 Cultural knowledge involves seeking and obtaining a sound educational foundation about diverse cultural and ethnic groups, 17 health professional exchange programs as the one examined in this case study could be seen as one such modality to achieve this competence. Cultural skill is the ability to collect relevant cultural data regarding a patient’s presented problem as well as learning to accurately perform a culturally based assessment.17,19 Cultural encounter and cultural desire are centered on encouraging health care professionals to directly engage in cross cultural interactions and feel motivated to learn, understand and apply cultural knowledge to the improvement of health care provision. 17 The model of cultural competence is useful in this study to understand the experiences of the health professionals in the health exchange partnership presented, the model will help to illuminate on the experiences and encounters of health professionals in a different socio-cultural context.
Methods
Study Setting
The study followed an exchange program for health professionals which is run and coordinated by the Norwegian Agency for Exchange Cooperation (NOREC). 20 NOREC is in Førde, Norway. The exchange program involved Kamuzu Central Hospital (KCH) in Lilongwe, Malawi, and Haukeland University Hospital (HUH) in Bergen, Norway. The exchange program between KCH and HUH represented a typical exchange of health professionals between development partners in the Global South and North. The 2 hospitals are part of very different health systems, one being in a low-income and another in a high-income context. The countries are also different in terms of social and cultural aspects. This study focuses on these socio-cultural aspects in this North-South partnership and on how such partnerships can be beneficial to health professionals in terms of strengthening their cultural competence in care giving. It is therefore against this background that KCH and HUH exchange program was chosen to be a case study to illuminate on this phenomenon.
Study Approach and Design
The study used a qualitative case study design. This was the most suitable design because the study followed a single case of a collaborative health partnership between Malawi and Norway in the attempt to understand how such partnerships enhance the cultural competence of health professionals. A case study aims for a holistic description and analysis of a case which can be a program, an institution, a person, a process, or a social unit. 21 This design therefore allowed us to have a detailed and in-depth understanding of the study phenomenon. From an epistemological standpoint the study is rooted in social constructivism, 22 where emphasis is on co-creation of knowledge together with the study participants. In this view the article presents a detailed in-depth experience of the participants as illustrated with direct extracts in the results section.
Data Collection
Data collection for the study was done between December 2020 and February 2021. Twenty semi-structured interviews conducted digitally constitute the data used for this article. The digital option using platforms such as Zoom, and WhatsApp were used as data was collected in the middle of COVID-19. It was the participants who chose the digital platforms that were suitable for them. The recruitment of the participants was facilitated by program coordinators at all the 3 institutions. Hence the program coordinators besides being participants in this study, they also acted as gatekeepers in the recruitment process. 23 However, consent was sought for from each and every participant. The duration of the interviews was about 1 hour.
Of the 20 interviews, 15 were originally used as data in the first authors’ master thesis, 13 while the additional 5 were analyzed to add and broaden the scope and depth of this article. The interview method was used because of its conversational nature, as Brinkmann and Kvale contends, when you want to understand people’s experiences with specific phenomenon, the best way is to talk to them. 24 In this study, we wanted to have an in-depth understanding on how health professionals’ experiences during an exchange program contributed to their cultural competence. This, therefore, made the interview method very suitable and in line with the study objective. An interview guide was used, exploring the health professionals’ expectations and experiences at host institutions with both colleagues and patients, as well as their experiences in this different social cultural context. The interview guide was open-ended and explorative to allow the participants to express themselves such as the tradition when using semi-structured interviews.
Participants in this study were drawn from health professionals, constituting mainly physiotherapists, radiographers, radiologists and nurses from both Malawi and Norway. Study participants also included key informants constituting the project coordinators from NOREC, Haukeland Hospital and Kamuzu Central Hospital. Of the 20 participants 13 were exchange program participants, while 5 were program coordinators. Two of the research participants were in both categories, that is, they had experiences as exchange participants and as coordinators of the program. With regards to gender, 12 were female and 8 male and their ages ranged from 26 to 57. Table 1 gives an overview of the study participants.
Overview of Participants.

These categories of participants were purposively selected in line with the study aim. Purposive sampling allows for the selection of participants with the right knowledge and information on the study phenomenon. 25 The categories we selected did not only enrich our data but also allowed us to triangulate our data. Triangulation of research participants helped us in enhancing the trustworthiness of this study. We required, as an inclusion criterion that health professionals need to have been stationed in the host country for not less than 6 months to significantly contribute to the experiences around the exchange and having had enough time to interact with the local colleagues as well as patients and communities from a different socio-cultural context. We stopped collection data when no new information was coming from additional interviews, that is, when we had reached saturation.
Data Analysis
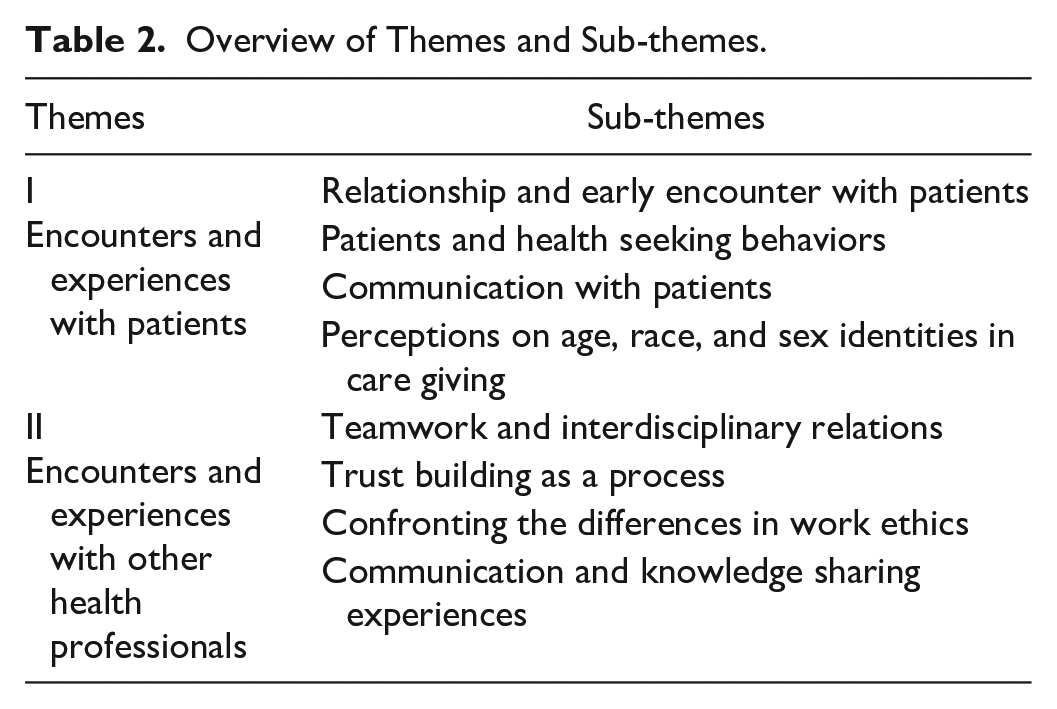
All interviews were conducted in English and voice-recorded, after permission was sought for and granted by the participants. After the data collection process, interviews were transcribed and the analysis began in NVivo 12, using thematic analysis. 26 Following the 6 steps of Braun and Clarke’s 26 thematic analysis helps in enhancing the credibility and dependability of our study findings, which contributes to the academic rigor of the study. The transcripts were subjected to a thorough review by both authors before the coding exercise began. The first few interviews were coded separately and then the authors discussed the coding framework. Themes that emerged during this process constitutes the results of this study. Table 2 gives an overview of the themes and sub-themes.
Overview of Themes and Sub-themes.
Research Ethics
Ethical clearance was sought and granted in Norway by the Norwegian Centre for Research Data (NSD) approved number 434310. In Malawi research clearance was not required as interviews with participants who were in Malawi was done digitally and we did not physically travel to Malawi for data collection. Permission to conduct the research was also sought for and granted by Haukeland Hospital (Norway), Kamuzu Central Hospital (Malawi) and NOREC (Norway). Participation was voluntary. Most of the participants gave written consent while in few cases consent was given orally. Informants were assured of the highest possible levels of confidentiality and anonymity. We have depersonalized and de-identified the research participants by giving them pseudo-names.
Results
In this section we will present the study findings. Two main themes emerged which are experiences and encounters with patients from a different socio-cultural context and encounters and experiences with other health professionals from a different socio-cultural context. Under these 2 emergent themes, there are several sub-themes (see Table 2). We used these sub-themes to organize and represent our results.
Encounters and Experiences With Patients
Participants had encounters and experiences with patients from a different social and cultural settings and they reflected on how these encounters impacted on their relationships and their roles as care givers. Sub- themes that are presented in this section are: relationships and early encounters with patients, patients health seeking behaviors, communication with patients and lastly perceptions on age, race and gender identities in this care giving context.
Relationships and early encounter with patients
Most of the health professionals from both Norway and Malawi reported a generally accommodative and productive relationship with patients during care giving in their host countries. One of the participants noted: “I was welcomed and accepted by the patients. It was very nice when you come in the morning, and all the relatives and patients are very happy to see you, they all greet you. They show a good spirit even though they had these serious burns and in a lot of pain, but the communication was nice and that was a good experience.” (Hege- Exchange Participant from Norway)
The cultural dimension in the relationships between the patient and the health professionals was a recurring discussion issue throughout the data collection period. Most of health professionals from Malawi found Norwegian patients to be more expressive than the patients they are used to. According to Chikondi, the relationship with Norwegian patients was flatter and more business-like and, in her words, patients “were more like clients.” Norwegian patients were therefore perceived more expressive, exhibiting freedom to make decisions or at least get involved in the decision-making process. This was a movement away from the traditional patient-caregiver paternalistic relationship which participants from Malawi were used to. As exemplified by the following extract: “There is what we call paternalism in health care, this is when health care professionals have more control over patients. You can see this difference in control on patients among health care professionals in Norway and Malawi. The more we are moving is that direction of being less controlling the more patients have more opportunities to make decisions themselves”. (Tionge- Exchange Participant from Malawi)
In the case of Malawi, hierarchy and respecting authority or expert power is a socio-cultural element that shapes and forms the bases of relationships. Consequently, Norwegian health professionals found Malawian patients as mostly reserved, quiet, and humble: “The patients were mostly quiet even if they had serious injuries. The guardians were also very quiet, not complaining and there was very little questions asked at least to me. . .maybe they were just being humble in meeting health professionals in the hospital. I think what is different from Norwegian relatives and patients is that they are more forward, and more aware of their rights”. (Rebekka- Exchange Participant from Norway)
Malawian patients’ humility in traumatic situations is also recurring in the findings. Most Norwegian participants experienced minimal display of emotions by the Malawian patients and their relatives in a hospital setting. Norwegian health professionals thus reported different experiences on how patients and their families communicated and expressed emotion, grief, or pain when facing traumatic health conditions and this made it difficult for them to know how to act and on what was the appropriate response in such situations. One NOREC coordinator shared his experiences on this while orienting and interacting with exchange participants: “Exchange participants have meetings and a program organized before they go to host institutions. Part of this is to prepare them, sometimes previous participants come to these meetings to share their experiences. Thinks like difference in conduct and how patients express themselves, things like how relative come into the picture and things like how patients are aware of their rights always come up. This is to prepare exchange participants, but you know preparation can never be enough”. (Erik- Coordinator, NOREC)
Erik here is touching on many issues including on how patients’ interactions with health professional could be influenced by socio-cultural factors. While on one hand the politeness and respectful nature of Malawian patients was generally interpreted as lack of understanding of their rights by study participants, on the other hand, Norwegian patients were described as “more forward” and aware of their rights, there could be a more complex and nuanced socio-cultural explanation for this. This explanation revolves around how authority, power and influence is interpreted in these 2 different settings.
Patients and health seeking behaviors
Participants reported that they noticed more severe and advanced health cases in Malawi compared to Norway. This was reported by both participants from Norway and Malawi. It was reported that patients visited the hospital when they were too sick or when the diseases were at an advanced stage in Malawi. Although Kamuzu Central Hospital is a referral hospital and severe cases are expected but so is also Haukeland University hospital. In this case the level of the hospital does not explain why in one context health cases were severe.
Malawian participants understood some people in the context only seek care from health facilities after they have tried other options available to them, which may include traditional medicine, herbs, religious inquiries, and other related home remedies. Additionally, to these other options, there are many health systems factors and non-health systems factors that hinder people in such contexts to access health care. In Norway on the other hand people generally use health facilities as the first point of inquiry and resultantly reduces chances of cases to become severe. One of the participants from Malawi succinctly summed up some of these differences between Malawi and Norway and Kamuzu Central Hospital and Haukeland University Hospital respectively: “These two hospitals are different, of course they are all referral hospitals but when you look at the population of Norway, it is about 5 million people, and those people are very rich. However, when you look at KCH, it is a referral hospital but there is no complete and functional district hospital in Lilongwe, so KCH still handles even primary, secondary, and then tertiary cases. Most of the cases that are supposed to be handled by lower-level health facilities, are still handled by KCH. We see almost every patient at KCH unlike HUH which is practically a referral hospital. Even if a staff member is injured there at HUH, they will even get care from a lower-level facility and only treated at HUH when it’s necessary. This is so because HUH is a referral hospital, and only deals with referral cases those that had been booked unless if it is like a real emergency. That is why I saw that there they were more organized but here in Malawi almost everything goes, there is no organization at all, there is no control”. (David- Exchange Participant from Malawi)
Although severe medical cases were experienced more in Malawi, it was also reported that a few cases of severely delayed medical conditions were also recorded in Norway. In the Norwegian setting such severe cases were associated with individuals or families with immigrant background, especially those still familiarizing with the Norwegian health system or those who are undocumented or lack proper documentation. It was also noted that such cases of delays to seek care was also prevalent among the Norwegian natives who were living alone, had minimal social contact, or marginalized in some ways. Hege, however noted that some Norwegian patients do not seek care because they are just reluctant or do not want to follow proper medical advice, despite that this advice is readily available: “When providing care to Norwegians you must really emphasize the need to follow instructions and you must follow up on them closely when they are not doing the exercises for rehabilitation. They have so much information at their disposal and individual choices to make. It is easy for Norwegian patients because they have more following up, they can come to outpatients’ clinics often”. (Hege- Exchange Participant from Norway)
Health professionals encounters with severe health cases gave them some more insight and understanding on difference in health seeking behaviors which could be explained largely by socio-cultural and environmental conditions.
Communication with patients
Language and communication reportedly brought different cultural tension between patients and health care professionals. For most of the health professionals, language influenced significantly how they communicated, interacted with and understood patients’ conditions. Some of the Malawian participants were afraid on their first encounters with Norwegian patients, however, as reported by below, they found it easy to communicate with most Norwegian patients in English: “I experienced very smooth interactions especially when the supervisor allocated me English speaking patients. I did not expect such a smooth experience because I thought patients would not allow me to see them upon discovering that I was a Malawian who just came on an exchange program and that I was going to be their physiotherapist. On the contrary they were so excited that they were going to be examined by someone new. So, on that part I found it exciting, it would have been very hard if it was the other way around”. (Chifundo- Exchange Participant from Malawi)
On the contrary, some participants found language to be a significant barrier. This was mainly in situations where they needed to act independently and in cases where they wanted to understand a patient’s condition and or give a patient some instructions: “Interacting with patients from outside of Lilongwe was quite hard. While I could not speak Chichewa, not all Malawian patients could communicate in English and that made it difficult for me to know if they were in pain or whether they had understood my instructions”. (Maria- Exchange Participant from Norway)
Langa had a similar experience to Maria where language became a barrier unlike Chifundo who was in a situation where he was allocated mainly English-speaking patients. Unlike Maria who was struggling with language in executing her duties, Langa even felt rejected by patients at times: “Language was a serious barrier and I felt rejected because sometimes patients preferred Norwegian nurses to me. This is so because they felt more comfortable in expressing themselves in their local language”. (Langa- Exchange Participant from Malawi)
Perceptions on age, race, and sex identities in care giving
Results show that age, race, and sex identities of both the patients and the health professionals significantly contributed to the relationships and care giving in the hospital setting. Some of the Malawian health professionals as shown in the extract from a program coordinator below, reported some marked skepticism from the elderly patients in the Norwegian context compared to the younger ones: “What we noticed is that some health professionals on exchange struggled to connect due to age differences between then and the patients. In some cases, at HUH we had visiting colleagues and patients with wide age differences. Older patients were likely to be more uncomfortable to be attended by a colleague from Malawi, while the younger patients who are well travelled and you know listen to American music, shows a general openness to our visiting colleagues. So, level of exposure seems to play a role too.” (Elin- Coordinator, HUH)
On the other hand, the Norwegian health professionals who were in Malawi were experiencing the opposite. It is reported that patients and their relatives seemed to trust the Norwegian health professionals more than the local ones and ideally keen to get services and advice from the Norwegian professionals. Maria, one of the participants from Norway find this challenging, especially in circumstances where her Malawian colleagues were even more qualified than her. It was difficult for her because after the clear show of preferences by patients and their relatives, she had to still redirect them in certain circumstances to more qualified local Malawian professionals: “I had a few challenges with that, at the hospital here in Malawi, when everyone sees a health professional from abroad with the medical coat, they think you are a doctor. Some patients came to me and asked if I could do their examinations. I said No, I cannot do that, when I told them that my colleagues are much better than me at this; they did not believe me”. (Maria- Exchange Participant from Norway).
While age and race here could be seen as something that negatively influenced the perceptions of patients in both contexts, Chikondi, a female and young health professional in her thirties from Malawi was elated to notice that in Norway both her age and gender were not seen as something that determined her competence or expertise. In this case, Chikondi felt welcomed and appreciated as a professional, something she struggled with in her home country Malawi where her competence and expertise is predicated on gender and age: “When I am attending patients back home (in Malawi), some of them even refuse treatment by just looking at my appearance as a young female health care worker. They opt for older people to treat them which is different from Norway. Patients did not really look at how old I was or how young I was looking; they just came to get the help. This was more assuring and very encouraging to come across patients who were elderly and were very willing to get help from me, it was very encouraging and very assuring”. (Chikondi- Exchange Participant from Malawi).
This could be based on that in Malawi, age and gender carry some socio-cultural meanings related to authority and power with younger people expected to give respect and authority to the elderly and where equally women are expected to show some respect to men. Chikondi being both female and young, would ideally make her position as a professional more questioned and scrutinized. This in the process affected her in discharging her professional duties.
Encounters and Experiences With Other Health Professionals
This section will present sub-themes which are under this main theme on encounters and experiences with health professionals from a different socio-cultural context. These sub-themes are teamwork and interdisciplinary relations, trust building as a process, confronting the differences in work ethics, and communication and knowledge sharing.
Teamwork and interdisciplinary relations
Participants interaction with management, and other health care professionals at their host institutions and this proved significant in shaping their experiences and competencies. In order to integrate at their new workspaces, participants had to learn new routines, interact with others as well as learning and understanding a new organizational culture: “Whilst working with other health professionals in Malawi I realized that I could not go there and tell them what to do, I needed to know the system and it takes time to know how your new teammates operate. You may think that you understand the system after a couple of weeks or months but then realize later that there are things happening that you are not aware of, important things that keeps the system going. Then you find that you are not yet part of the system because things were going on in Chichewa and I was not being involved. So, I realized and learned earlier that I just know a little about the system, and therefore, it was difficult to give advice about the system that I did not know. Due to this lack of local knowledge of the system, I had to cooperate closely with my coworkers to help me know and understand the system and only after this, I was able to meaningfully contribute”. (Hege- Exchange Participant from Norway)
Participants from Malawi too were willing to participate and learn in teams at HUH. They benefited in learning new ways of doing things and a new work culture. It was particularly important for majority of them to feel that their expertise was also valued even in the Norwegian context: People are curious to understand how others do their work, Norwegian health professionals also helped me to understand how things are done in their context, especially also those coming from HUH coming to KCH were also trying to adapt to our way of doing things. They understood that they cannot change everything, they needed to understand that we have our way of doing things under limited resources. For them to be able to help us doing our work, they needed to know where to start from. They needed to better understand how we think, and this is what they have learnt, I think. (Jacob- Exchange Participant and Coordinator, Malawi)
It emerged that the need to understand the context was important for participants to meaningfully contribute at their new workstations. There was a lot for participants to learn, including diseases and illnesses they were not familiar with or used to handle. In this regard, teamwork was important. All exchange participants emphasized the need for an effective way of communicating and the need to be accommodating to different ways of doing things and divergent views on issues.
Trust building as a process
While understanding and respecting the collaborative context was essential for teamwork, participants from both KCH and HUH reported that mutual trust was significant in them thriving in their new workspaces and contexts. Trust building was seen and defined as a process and not an event and this was important in establishing rapport between teams. Most of the participants from and in both contexts felt that they were shown more trust when they demonstrated a willingness to learn and commitment to their work. In the event of building this trust, participants reported full commitment and a willingness to learn was always preceded by some level of skepticism: “When you go into a new context you need to show and demonstrate that you are willing to listen and to learn. You don’t go there and say I know everything. You need to build trust with others and when you do that people start to feel comfortable with you. They start to include you in their events, activities, and issues. They start to tell you things and you become part of their team. It is like that, and this is my approach”. (Marte- Exchange Participant from Norway)
This shows that gaining trust was something that participants invested time in. Trust was not given and not an event but negotiated and re-negotiated in the process. However, most of Norwegian participants felt that it was much easier for them to be trusted and integrated into the system because they had the “expert” knowledge needed in Malawi’s trauma care department, and they also had knowledge on using advanced medical equipment. Regardless, there was a need for a careful balance between sharing this knowledge and respecting the Malawian systems and ways of doing things.
Confronting the differences in work ethics
Experiences of existing differences in professional and work ethic between Malawian and Norwegian participants were seen to initially creating cultural misunderstandings and clashes. However, these were later transformed into opportunities to learn and understand the context even beyond the hospital setting. Participants from both KCH and HUH struggled to cope with differences in work culture in relation to time management, structure of meetings, reporting for work and general job execution. Norwegian participants who were in Malawi reported being frustrated by the slow and casual approach to work in Malawi, while the Malawians in Norway experienced an unfamiliar work culture that was more structured, time conscious and where meetings were very common comparatively. All these situations frustrated participants in both contexts. For instance, participants such as Rebekka reported facing challenges in adjusting to the working culture: “In Norway, we have working hours and we keep them. I struggled a lot in Malawi because there are working hours but occasionally people don’t meet them. They may report to work at different times, or you may not even know where they are during hours where they are expected to be working. The more you understand their system, it becomes better but some of these things you may not get it”. (Rebekka- Exchange Participant from Norway)
Many from the Malawi on the other hand felt that there were too many schedules, deadlines, reporting and team meetings in the Norwegian work culture: “One thing is that there was many meeting in Norway. In these meetings same things were discussed almost every week. This is something I am not used to from Malawi, we do not have many meetings as they do. Sometimes you try to get used to it, but sometimes it is overwhelming” (Tionge- Exchange Participant from Malawi)
While the Malawian participants were frustrated with the Norwegian work culture, especially in terms of many meetings, deadlines, and reporting, they also felt it was an effective way to assure that there was teamwork and that each individual delivers on their work tasks.
Communication and knowledge sharing experiences
Communication emerged as one of the most important issues in the interviews, communication was referenced in at least 3 ways, that is, in terms of language of instruction, social relationships, and cultural interpretation. Most of participants in both contexts reported effective communication when using English language, as vernacular languages in both contexts were perceived as major barrier for effective communication. However, Malawian participants were relatively affected by this more than the Norwegian participants. It was reported that people in Malawi, including patients, whenever they can they were much more willing to speak in English than people in Norway: “The thing is that I was lucky in Lilongwe because many people speak English. I think they learn it early and are confident to speak it whenever they can. On the other hand, Norwegians generally want to avoid speaking in English whenever they can. I will also avoid English whenever I can, so maybe the Malawians faced this language challenge in Norway. The languages (Norwegian and Chichewa) are not relatable in any form, making it more difficult”. (Marte- Exchange Participant from Norway)
Tionge agrees with Marte, he expressed that he felt as if he was an intruder in the Norwegian context. This was compounded by the fact that in the Norwegian work culture as stated above, meetings are quite often, and these are conducted in Norwegian: “I did feel like an intruder, you are in a situation where people are communicating in a language you do not understand. In meetings, you may ask someone sitting next to you to help with interpretation but then you can find that you are now disturbing someone. I ended up stopping attending these meetings because it was not helping me in any way”. (Tionge- Exchange Participant from Malawi)
In general, therefore, language was reported by most participants as a constraining factor. This was also noted by the project coordinators at both hospitals and NOREC as an issue they know and a matter that requires attention. The duration of the exchange, however, could be challenging for participants to develop linguistic competence in the language of a host nation.
Discussion
This discussion section focuses on the main issues that emerged in the results section from the 2 main themes presented. The cultural competence model is used to illuminate on these issues. The discussion will also be situated into the current literature in this study area.
Encounters and Experiences With Patients as Significant in the Building of Cultural Competence
Encounters and experiences with patients from different social and cultural settings emerged as a major theme in our findings, these early encounters and experiences impacted on how participants developed relationships with patients in the host country and on how they disposed of their duties as health professionals. These encounters greatly shaped their exchange experiences and consequently their cultural competence.
Most of the health professionals from Malawi found it easier to interact with patients from Norway because the patients took a participatory role in their own treatment. There was a consensus that the patient and health worker relation was flatter and less paternalistic in Norway compared to Malawi, and this is also reported in other studies.27,28 Participants from Norway were not used to patients that seem to question less and agrees with almost everything advised by health professionals.
This, however, could be explained by the different structures of these 2 countries. Norway can be classified as having an individualistic outlook and pursues libertarian values where individual freedoms find more expression. 29 Malawi on the other side can be classified as a country pursuing egalitarian values, where communal living and respect for authority find more expression. 13 These different set-ups in terms of the structures and hierarchies of authorities can be explained within the cultural encounter dimension of the cultural competence model. Health professionals need to be aware of how the societies they practice are organized because this also influence on how they interact with patients, patients’ relatives, colleagues, and communities around. Understanding external factors within health settings is important in health care, including the governance culture and structures. 30
Another important finding of our study is based on differences in health seeking behaviors in the 2 different contexts. Severe and advanced health cases were reported in Malawi compared to Norway. While this may not be a very surprising findings given many various health systems challenges in Malawi, 12 the Norwegian participants were able to learn that there are other important social, cultural, and religious factors that may contribute to the health seeking behaviors of patients. Some people in the Malawian context only seek care from health facilities after they have tried other options available to them, which may include traditional medicine, herbs, religious inquiries, and other related home remedies. 31 In Norway on the other hand people generally use health facilities as the first point of inquiry, therefore with regards to health seeking behaviors, participants from both countries learned from these differences, some of which are socially and culturally informed and founded. For Norwegian participants, these experiences are particularly important as Norway is slowly becoming a multicultural country, 32 hence having experiences with patients in different contexts enhances their cultural knowledge and competence.
The identities such as gender, and race also proved to be contributory to the experiences and encounters of participants with patients. Race especially in the context of Malawi a country that has a recent history of colonialism, defines power hierarchies and dynamics. 33 It is this that perhaps explains why patients and their relatives preferred to be treated and to take instructions from a white, health professional, Maria, even when she felt that she was less qualified than local professionals. In Malawi as with many other countries in Southern Africa, which experiences vices of racial segregation, discrimination and apartheid, 34 as settler colonies, still by and large suffers from a racial inferiority complex where a white person is perceived and considered as more skilled and knowledgeable. 35 When going in such contexts, health professionals need to be aware of these deep-seated biases, which at face value may just appear as a preference.
Additionally, the results also show that older Norwegians seem not to prefer to be treated by professionals from Malawi, while language may partly explain this, it can also be identified and defined in racial terms. Norway has been largely a homogenous country until recently, and in this new process of multiculturalism, older generations may not be used to receive essential services from people of color and races. This too is not just a preference, but something to be interpreted as some deep-seated racial biases. 36
Gender as also another identity, was reported to have influenced how health professionals are perceived with regards to the discharging their duties. Chikondi felt that in Norway the fact that she was young and female, seemed not to affect the way she interacted with patients in any way. This is contrary to her experiences in her home country of Malawi where being young and female serve as a disqualification of skills and knowledge. This could be explained by how these 2 countries stand in terms of gender equality and the empowerment of the girl child. Norway is largely used as an example of countries with gender equality, 37 while Malawi has some long way to go in this regard. 38 This shows that participants in this study were aware that various identities influence how they are perceived in care giving and in interacting with their patients and colleagues.
Encounters and Experiences With Other Health Professionals as Contributory to the Building of Cultural Competence
Our study results show participants’ cultural awareness in respecting their host institutions’ systems, conditions, and contexts. Participants cultural awareness of differences in context helped to build trust and respect, and resultantly reduced tensions and promoted synergy in the collaborative exchange. Some of the Norwegian health professionals reported being more motivated to provide medical advice to Malawian health professionals in instances where they actively showed commitment to shared learning. In the same vein, the Norwegian participants were also aware that their experience in relation to their technological advancements in the field of emergency medicine would possibly undermine the local knowledge of Malawian health professionals, unless they adopted a participatory, accommodative, and respectful training approach. This demonstrates that cultural awareness can foster common understanding and enhance the cultural competence of health professionals.
Results also demonstrates Malawian health professionals were more willing to be receptive to the education and training from Norwegian health professionals when they felt their local approaches to trauma care and emergency medicine were being respected and appreciated. For professionals from both settings to establish a common understanding, it had to start by acknowledging their biases and confront them. Previous studies show that if not carefully and intentionally designed, cross cultural learning experiences and partnerships have the potential to reinforce bias, stereotypes, paternalistic actions, and a superior-inferior dichotomy.39-42 In this study as the results has demonstrated, exchange participants were largely aware of their biases both at professional and individual level and therefore were aware that such exchange collaborative programs could lead to cultural imposition and power domination.17,43 For example, we have heard Marte and Hege expressing that they realized early that they needed to respect and understand the Malawian ways of doing things first in order for the Malawians to pay attention to their contributions. This awareness is important because it minimizes instances of cultural imposition.
The study illustrates the importance and impact of cultural knowledge when building a foundation for team collaboration. Health professionals in their local contexts, were key in bridging and building cultural knowledge and skill in health care at both KCH and HUH. For example, most of the exchange participants were very much aware that they needed to use their local colleagues as a resource to learn and acquire knowledge. This local knowledge varied from familiarization with the disease profiles of each context, to familiarization with local institutional routines.
The study has demonstrated the importance of communication, and the more participants managed to communicate effectively, the more they understood the local context better, including sociocultural context around them. To the contrary, participants also struggled to cope in cases where they did not have local colleagues to consult from. According to a review study by Lin et al from China, it emerged that the application of cultural knowledge to clinical care was important but depended on how each health professional interpret the cultural sensitivity of their tasks which depended on their knowledge. 44 In a study from a Kenyan and USA health partnership program, participants reported being able to observe the cultural knowledge, and skill that their working partners possessed and use these in performing their own duties as well in these new environments. 41 In this study, some few participants, in both contexts, felt frustrated, neglected, and abandoned. This frustration could be explained by the fact that these participants felt that they did not have had opportunities to acquire relevant knowledge and skills to develop their cultural competence in the host country.
Participants actively showed a great desire in enhancing their knowledge, skills, and competencies. One striking example is related to how the participants cope with the language challenge, which is a known barrier for effective communication, 30 interaction and in the execution of work tasks. However, because the desire to learn was there, many of the participants resorted to resourceful strategies of using their colleagues as resources in solving the language puzzle while others utilized information technologies and online learning platforms.
Learning to work in a different social cultural context with different work ethics and work culture also emerged as one of the most important findings for this study. Participants reported both positive and negative experiences around this. The differences in professional and work ethics were seen initially as creating cultural misunderstandings and clashes, and hence acted as a barrier for teamwork and learning. However, these were later transformed into opportunities to learn and understand the context even beyond the hospital setting. Differences in relation to time management, punctuality, the culture of meetings and general job execution, proved to be conflictual in terms of work values and norms. While Norwegian participants expressed frustrations about the work culture in Malawi as they experienced it as driven by a slow and casual approach, the Malawian participants were equally frustrated by the Norwegian work culture, which they experience as demanding, inflexible and offers less autonomy to individuals. These findings relate to literature on work cultures between western and non-western societies and the philosophies of time management. 41
This study demonstrates the importance of social and cultural factors in care giving. Accounts from our study participants who had participated in a health professional exchange program showed that such exchanges can help greatly in equipping health professionals with skills they need in an ever changing and multicultural global world. The study demonstrated that health professionals in our study learned a lot from this exchange. Their experiences were largely positive but also negative in some case, however, all these experiences contributed meaningfully to their cultural competence in providing health care.
Study Limitations
The study was conducted in a limiting environment due to the COVID-19 pandemic. Due to this we had to alter original plans of collecting data through face-to face interviews to digital means. Using digital platforms such as Zoom and WhatsApp to collect data, might have limited the way we interacted with our participants. In face-to-face situation, it is easier to pick up nonverbal cues while in digital options these could be lost. Additionally, the first author wanted to travel to Malawi for data collection, but it was not position due to restrictions in traveling during this period. Furthermore, the study used purposive selection of participants, although it is a strength in qualitative research, by selecting the participants we defined and identified to have necessary knowledge on the study phenomenon, we might have in the process missed other potential participants that could have enriched the study in other ways. The sample size for the study is 20, no power calculation was used to estimate this sample number. In general, in qualitative research, we aim for saturation, and in the case of this study, we stopped data collection when no new information was coming from additional interviews. This could also be seen as a possible limitation of this study.
Conclusion
The study demonstrates the importance of collaborative exchange programs in building the cultural competence of health professionals. Both participants from Malawi and Norway largely reported positive experiences in their host institutions. Their experiences centered around their interactions and encounters with patients, patients’ relatives, and colleagues at host institutions. Participants reported a better understanding on health seeking behaviors in different contexts, the importance of communication with both patients and colleagues, and teamwork. In addition, the study revealed the importance on perceptions around identities such as race and gender and how these impact on health professionals’ interactions with patients and care provision. Furthermore, it emerged that although working in a different socio-cultural environment was challenging, it was experienced as enriching and rewarding in terms of building and developing cultural competence. To this end, the study concludes that North-South health professionals exchange partnerships can be a viable vehicle for developing and naturing cultural competence in health professionals, however, these programs need to also invest in preparing the participants to be ready for the known challenges that lies ahead in host institutions and countries, some which have been highlighted in this study.
Future Research and Directions
The study has highlighted on the importance of social cultural aspects of care and specifically the role that North-South health partnerships can play in building the cultural competence of health professionals. Going forward, it can be interesting to investigate how new emerging theoretical concepts in this field such as cultural safety and humility can also contribute to the understanding of this socio-cultural and contextual dimension of care.
Footnotes
Acknowledgements
We thank all the informants and participants in this research for their valuable insights.
Author Contributions
The authors of this manuscript all made substantial contributions to the acquisition and interpretation of the data, drafted, and revised the manuscript, (and approved this version of the article to be published in INQUIRY: The Journal of Health Care Organization, Provision, and Financing).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article