
Abstract
Earlier research on the novel coronavirus (COVID-19) mainly focused on fear and its psychological impact on frontline health workers. However, the uncertainty of COVID-19, job insecurity and its effects on non-frontline employees’ perception of their well-being is rarely explored. This study aims to assess the relationship between subjective well-being and the fear of the COVID-19 outbreak. Furthermore, this study explores how employees’ awareness of their job insecurity influences this relationship. Structural Equation Modelling (SEM) and Confirmatory Factor Analysis (CFA), and Spearman’s correlation analyses were used to examine the significance of the relationships between fear of COVID-19 and subjective well-being and the moderating role of job insecurity in this relationship. The findings indicate that greater fear of COVID-19 is associated with a lower level of perceived subjective well-being. However, a higher perception of fear of COVID-19 and its interaction with job insecurity are associated with a higher risk of employees’ well-being. Our study highlights the factors such as fear of COVID-19 and job insecurities that undermine their well-being. Our study provdies practical implications for employees’, managers, and healthcare policymakers to adopt effective strategies to reduce stress among employees. These recommendations include using practical tactics to safeguard the employees health and jobs while effectively coping with the pandemic.
During the first wave, the fear of COVID-19 adversely affected the health care professionals, and their well-being was seriously affected; even suicide was reported among young doctors in Pakistan. The severity of the third wave, its fatal outcomes, a burden on the healthcare system, and the devastating situation in neighboring country India are some reasons that are creating hype of fear among the nurses of Pakistan. Nursing employees dealing with natural disasters, stress episodes, and operational risk events are more prone to stress that is heinous to their well-being.
This study contributes to the contemporary research on mental health and that COVID- 19 literature. This study also contributes to the well-being and COVID-19 pandemic literature in the case of healthcare literature. Finally, this study will also provide some very useful and practical implications for nursing staff heads and health care policymakers to mitigate their fear and boost their well-being.
Management and Policy Makers 1. Management should be visible and approachable to the nursing staff. From time to time, asking how staff are feeling may help and boost their morale. 2. Communication has very useful results. Regularly communicate with staff. When face to face contact is not possible, a concise and clear email may serve the purpose. Acknowledge the nursing staff’s needs, boost their confidence, show empathy, and value their contribution to helping COVID-19 patients. 3. Indicate to staff that their well-being is the priority of management. Implement mandatory work breaks and effective monitoring, and ensure there is individual and team support for each staff member. 4. Plan for shifts of nursing staff. Rotate their duties from high stress to low stress. Partner experienced and inexperienced nursing colleagues, and make sure there is a supportive culture. 5. Remove non-urgent and unnecessary business to reduce the workload and alleviate the staff burden. 6. Provide training for traumatic situations; convey the factual and coping skills necessary for potential mental health issues.
Background
The outbreak of the COVID-19 started in Wuhan City, Hubei, a central province of China, in mid-December 2019. 1 The World Health Organization (WHO) declared a novel coronavirus pandemic as a public health emergency of international concern at the end of January 2020. 2 The threat of a third wave of the COVID-19 affects all areas of the planet. Vieira, Franco, Restrepo, Abel 3 document that, practically, stress is inescapable in this dramatic, terrible condition. Besides severe threats to lives and physical health, people face psychological disorders such as anxiety, depression, and panic disorder.4-9
The life and well-being of the masses are seriously affected by the fear of infections from the COVID-19 pandemic. Specifically, the public’s well-being is being even more undermined by the psychological impact of COVID-19: strict isolation measures, discontinuation of educational and recreational activities, and pressure on existing healthcare facilities.
10
The frontline workers such as healthcare staff, personal and home care aides, paramedics, and police are among those who face the highest risk of becoming physically ill and also facing severe mental pressure.11-15 However, the COVID-19 pandemic’s trauma is not limited to frontline workers. Employees in service sectors that involve physical contact with other people, such as cashiers in grocery stores, couriers, and banks, also face elevated risks. This study aims to analyze the relationship between the subjective well-being of employees working in the nursing sector of Pakistan and the fear of the COVID-19 outbreak and to explore how employees' job insecurity due to the ongoing economic crisis from COVID-19 influences this relationship, as shown in Figure 1. Conceptual model.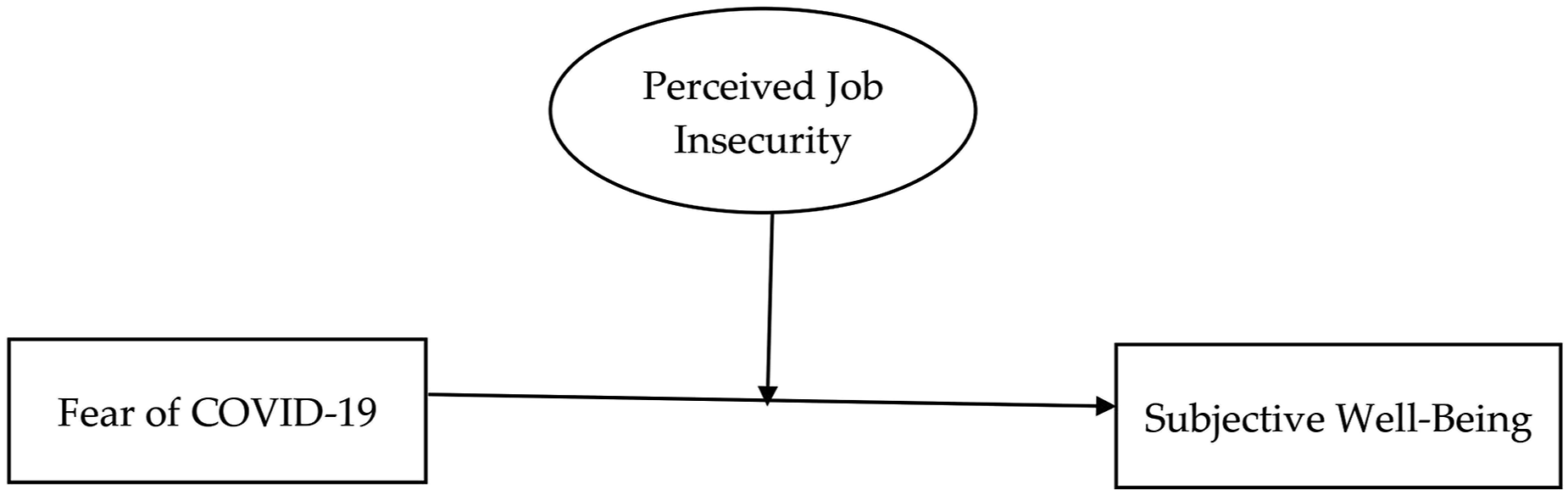
In Pakistan, the COVID-19 outbreak occurred late February 2020 due to refugees returning from Iran. The first 2 waves have significantly disrupted the masses in Pakistan. Now, the country is facing the third wave of the pandemic. As of 2nd July 2021, the total number of patients is more than eight hundred and twenty-nine thousand. Furthermore, there have been more than eighteen thousand deaths, out of which the death count of nurses and paramedics is estimated to be 360. 16 Low levels of psychological support, scarcity of first-hand medical information, shortage of personal protective equipment, and lack of training on infection control measures have severely affected the health and well-being of nurses. As a result, they have experienced high levels of stress and psychological distress. 17
This study has been selected to investigate the nursing staff of Pakistani hospitals for 2 reasons. Firstly, Pakistan’s geographic location is crucial. Pakistan shares borders with the 2 most critical countries, 18 China, where COVID-19 was first diagnosed, leading to a worldwide outbreak, and India, where the spread of the third wave of COVID-19 has overburdened the health system. Indian hospitals are overcrowded, the supply of oxygen is inadequate, and the ratio of positive cases has increased by more than three hundred thousand cases per day. Pakistan is addressing the issue by either regionally targeted or complete lockdown in the country. As a result, the shutting down of industry, strict isolation, job losses, and fear of COVID-19 has seriously affected the nursing sector in Pakistani.19,20
The second primary reason for this study is that the nursing sector in Pakistan suffers from the fear of COVID-19, limited healthcare facilities, and work-related stress. During the first wave, the fear of COVID-19 adversely affected the well-being of healthcare professionals, even leading to cases of suicide being reported. 17 The severity of the third wave, its fatal outcomes, a burden on the healthcare system, and the devastating situation in the neighboring country, India, are some reasons that are creating intense fear among the nurses of Pakistan. Nursing employees dealing with natural disasters, stress episodes, and operational risk events are more prone to stress that is detrimental to their well-being. 21 The prevailing economic crisis due to COVID-19, increase in medical expenditure, and fear of becoming infected with COVID-19 cause job insecurities for nurses.
This study contributes to the contemporary research on mental health and COVID-19 literature. This study also contributes to the well-being and COVID-19 pandemic literature within the area of healthcare literature. Finally, this study will also provide useful and practical implications for heads of nursing staff and healthcare policymakers to mitigate staff fear and boost their well-being.
The rest of the paper is distributed as follows: Literature Review and Hypothesis Development explains the research methodology, Materials and Methods presents the results and discussion, and Results and Discussion concludes the study with practical implications.
Literature Review and Hypothesis Development
Fear of COVID-19 among Nurses and its Effect on Their Subjective Well-Being
The pneumonia-like disease, COVID-19, appeared in Wuhan in November 2019. Within a few months, it had spread to more than 200 countries around the globe, causing significant damage to public health, huge economic losses, and affecting every aspect of life. 22 Being a life-threatening, contagious, infectious disease passed person-to-person, COVID-19 caused people to be afraid of it, and this perception of fear was increased by rumors, news, non-availability of prior information, and uncertainty about the future. 23
Beck and Emery (1979) 24 defined fear as “awareness and appraisal of danger, and anxiety as the unpleasant feeling state and physiological reaction that occurs when fear is provoked”. Thus, as a primary form of emotion, it is commonly found in men and women of all ages, cultures, and races. Thus, a fatal contagious epidemic such as COVID-19 can ignite the emotion of fear, anxiety, and panic among people around the world. Furthermore, a lack of prior knowledge, non-availability of real-time information, and dissemination of rumors on social media all easily added to the increasing fear of the COVID-19 pandemic situation. 24
Nurses, alongside doctors and other paramedic staff, played their role as frontline workers during this pandemic. 25 When every country’s healthcare system was overburdened and presented with several challenges, nurses were committed and performing their duties in acute fear of risking their lives, being infected, or infecting others. According to the International Council of Nursing (ICN), more than one hundred thousand confirmed COVID-19 cases worldwide were healthcare workers, including nurses. 22 Moreover, erratic and exhaustive work schedules, an intense work situation, non-availability of personal protective equipment (PPE), and working in unfamiliar stations affected the nursing staff. 26
Subjective well-being, the most studied phenomenon of positive psychology, is an effective factor of the human cognitive process, 27 which predicts a range of outcomes, including happiness, health, and other psychological functions.28,29 Ulloa, Møller, Sousa-Poza 30 called it the ultimate goal of an individual’s life for which 1 strives very hard. The happy people, whose subjective well-being is at a higher level, are more successful in social relationships, have good physical and mental health, and are more creative and proactive in social behaviors and problem-solving skills. 31 The subjective well-being of an individual is very much influenced by their surrounding environment and the situations the person is facing. This relationship is better examined by transactional stress theory which asserts that stress is merely an exchange between a person and their context. 32 It can cause damage to a person by threatening their well-being. The intensity of the factors, including past experiences, job demands, and current levels of job stress 33 may cause controllable and uncontrollable short or long-term stress. 34 Transactional stress theory is based upon cognitive and attitudinal appraisals, which state that stress is transmitted through an interactive process and ultimately affects the well-being of individuals. A hospitality industry study during the COVID-19 outbreak 35 found that workers' perception of this spread of COVID-19 was based upon their environment, which increased the likelihood of depressive symptoms, ultimately affecting their well-being. Bermes 36 also explored how the sharing of fake news pertaining to the spread, and adverse outcomes, of COVID-19 also caused transactional stress which can have a number of devastating consequences.
The emergence of COVID-19 impacted the subjective well-being of frontline healthcare workers, particularly nurses. Recent research found several mental health issues, including depression, burnout, stress, and anxiety, in frontline workers, including nurses emerged due to COVID-19.37-39 Various recent studies found that post-traumatic stress and emotional fatigue among nurses directly dealing with COVID-19 patients.40,41 Early studies carried out by Huang, Lei, Xu, Liu, Yu
40
in the Chinese COVID-19 outbreak context found adverse emotions, anger, sadness, and fear of contagion in staff working in hospitals. The fear of COVID-19 has adverse social, mental, and health consequences significantly associated with mental health symptomatology and well-being.
41
Thus, nurses dealing with COVID-19 patients face the stress that affects their mental and psychological health and ultimately affects their subjective well-being. Therefore, we hypothesized that: HI: Fear of COVID-19 is significantly associated with the subjective well-being of nurses dealing with COVID-19 patients.
Perceived Job Insecurity and Subjective Well-Being
Perceived job insecurity can be defined as a threat to the maintenance of the current job’s continuity.
42
It can be divided into qualitative and quantitative aspects. These 2 facets deteriorate individuals' affective (subjective, physical, psychological well-being) and cognitive (undesirable reactions) abilities of individuals.
43
Due to working in a rapid-contact environment, frontline health workers are at a high risk of COVID-19 infection. Recent research indicated that high contact frontline workers were afraid of COVID-19. Those who suffered more did not report to work and were more exposed to financial vulnerability and job insecurity.44-47 From Pakistan’s perspective, nurses were unwilling to serve the COVID-19 patients without any extra incentive or family pressure. Thus, the administration forced them to treat COVID-19 patients, which caused job insecurity among them. Past researche indicated that uncertain contextual factors, i.e., health disasters, economic downturn, rapid technological changes, and political instability, can result in a high level of unemployment which can cause employees to a sense of perceived job insecurity.44,45,47 Thereby, fear of COVID-19 can result in frontline healthcare workers' perceived job insecurity. Indeed, due to COVID-19, diminishing labor costs (often by reducing wages and the number of employees) and restructuring operations might be undertaken by many organizations. Such organizational changes may induce a feeling of job insecurity in employees.
46
Additionally, during the pandemic, to prevent the transmission of COVID-19, many service organizations gradually adopt new technology (eg artificial intelligence) to replace human jobs,
48
making frontline healthcare workers' jobs insecure. Therefore, we hypothesized that: H2: Fear of COVID-19 is positively associated with perceived job insecurity.
People’s lives and jobs are in jeopardy as a result of the COVID-19 outbreak. The threat of losing a job might make it challenging to stay engaged at work, increasing the temptation to leave early 49 and decreasing subjective well-being. 50 The conservation of resource (COR) and job demand resource model (JD-R) are excellent theoretical perspectives by which subjective well-being (SWB) can be understood. 51 During COVID-19, employees' perceived job insecurity (PJI) can be seen as potentially losing their resources, thus reducing SWB. Previous studies evidenced that job insecurity could cause resource loss and negative psychological concerns such as SWB, depression, and anxiety.52,53
The JD-R model also proposes that cognitive and emotional job demands drain individuals' physical and mental resources and reduce SWB.54,55 The changes related to the work conditions of frontline healthcare workers due to COVID-19 – increased job demand – may generate additional stressors, thereby decreasing their physical and mental resources and possibly raising SWB.
56
Moreover, to complete tasks in a high-risk environment, frontline healthcare workers must mobilize more effort to control their emotions; this can deplete their resources and cause psychological imbalances that, if unmanaged, can reduce SWB. Thus: H3: PJI is positively associated with SWB. H4: PJI mediates the relationship between fear of COVID-19 and SWB.
Materials and Methods
This study recruited nurses who were directly engaged in treating patients with COVID-19 in different hospitals in Lahore, Pakistan. Due to the pandemic and lockdown, an academic survey was conducted with a limit to a single input. Before data collection, we had obtained the ethical approval to conduct this study from the institutional review board of Hailey College of Commerce, University of the Punjab, Lahore, Pakistan, with reference number D/79/HCC, Feburary9th 2021. Every public hospital in Lahore has established COVID-19 wards with dedicated staff. The researchers collected data from Lahore General Hospital (LGH), Services Hospital (SH), Jinnah Hospital (JH), and Mayo Hospital (MH). The sample of the study consisted of 600 nurses working in COVID-19 wards of different hospitals in Lahore. As the study population was not known, Thus, 600 nurses were selected as a target sample size. According to Cochran, 57 320 is the minimum required sample size for an unknown population, with a confidence interval of 95%. The researchers enhanced the sample size, keeping in view the limited response rate and incomplete questionnaires, to get better and more accurate results. Informed written consent was obtained from the participants for voluntary participation in the study through answering a “Yes or No” question, and privacy of the contents was also ensured.
The survey consists of 2 sections: 1) Demographics, 2) Fear of COVID-19, subjective well-being, and job insecurity items. All the responses were obtained on 5 points Likert scale with values ranging from 1 for Strongly Disagree to 5 for Strongly Agree. The demographic information of the respondents, consists of their age, material status, and work experience, were obtained.
The fear of COVID-19 scale, developed by Ahorsu, Lin, Imani, Saffari, Griffiths, Pakpour, 58 was used to assess fear of COVID-19 as perceived by participants. This scale consists of 7 items, and an example of 1 of the items is “I am most afraid of coronavirus-19". This scale’s composite higher internal consistency, reliability (Cronbach alpha) is .81, which is greater than the acceptable level. 59 The second variable, the perceived subjective well-being of participants, was measured using the satisfaction with life scale of García, Barraza-Peña, Wlodarczyk, Alvear-Carrasco, Reyes-Reyes, 60 which consists of 3 items related to satisfaction with life, financial satisfaction, and overall happiness. This scale accounted for high internal consistency with a Cronbach alpha value of .74. Finally, the perceived job insecurity variable was measured using the scale developed by De Witte, De Cuyper, Handaja, Sverke, Näswall, Hellgren, 61 consisting of 4 items wherein the reliability (Cronbach alpha) of this scale is .84.
Data analysis of this study was carried out in 2 stages. Firstly, preliminary analysis techniques were used to check whether the data fit for further analysis. Secondly, the Structural Equation modelling technique and factor analysis were carried out for hypotheses testing. Moreover, descriptive statistics were conducted via frequency distribution and a clustered bar chart. Furthermore, in inferential statistics, this study uses Spearman’s correlation analysis as we have ordinal data. Data analysis was carried out using the Statistical Package for Social Sciences 23.0 and associated AMOS Graphics.
Results and Discussion
Using simple random sampling, we have distributed the questionnaires to 600 nursing staff of COVID-19 wards of public hospitals, including Lahore General Hospital (LGH), Services Hospital (SH), Jinnah Hospital (JH), and Mayo Hospital (MH). After many follow-ups and reminders, we received only 340 useable responses, a response rate of 56.67%. The demographic details of the respondents are as follows: 122/340 (36%) nurses belong to the 20-30 years group, 187/340 (55%) nurses are from 31-40 years old, and only 31/340 (9%) nurses are above 40 years; majority 262/340 (77%) nurses are married while only 78/340 (23%) are unmarried; and197/340 (58%) nurses have 1-5 years work experience, while 143/340 (42%) have above 5 years work experience.
Figure 2 shows the nursing staff’s responses on the fear of COVID-19, subjective well-being, and job insecurity variables. The first 7 statements represent the fear of the COVID-19 scale; the findings show that most of the nursing staff perceive that listening to news and cases of COVID-19 on social media creates anxiety, as out of 113 nursing staff, 45 replied ‘stronger agree’ for statement number 5. When watching news and stories about COVID-19 on social media, I become nervous or anxious.’ 3 statements, SWB1, SWB2, and SWB3, represent the subjective well-being scale. The findings indicate that nursing staff suffers from fear of COVID-19, reducing subjective well-being and financial constraints. Most of them, as out of 107 nursing staff 45 replied ‘strongly disagree’ for the second statement, ‘SWB2. I am satisfied with the financial situation of my household’ on this scale. Finally, the last 4 statements of Figure 2 illustrate the job insecurity scale, as out of 105 nursing staff, 45 replied ‘stronger agree’ with the last statement, ‘JI4. I might lose my job in the near future.’ This finding indicates that nurses are feeling insecure about their jobs in the near future. Response on fear COVID-19, subjective well-being. and job insecurity.
The normality of the data was checked through skewness and kurtosis, and results indicated that all the values fell between the ranges from −1 to +2. Content validity was ensured through Cronbach’s alpha. The convergent and discriminant validity were established through factor analysis. Confirmatory factor analysis (CFA) was conducted to check the robustness of the dataset. The study used the scales already well-established and tested. However, still, there is a need to validate these scales in the context of Pakistan’s service sector. Variance analysis showed that R-Square values for all the constructs are significant, as all the items returned a high proportion of variance in the outcome variable. The minimum R2 is .28 for J4. However, the maximum value is 1.00 of J1, .99 for F4, .81 for F3, .76 for S2, and .73 for F1 etc.
Factors loadings for fear of COVID-19, subjective well-being, and job insecurity met above the minimum accepted trash hold. The values of weights of standardized regression of all items are greater than .5 except for 1 item, ie, Job insecurity JI4. Results also indicate that all independent items' variance in the dependent variable is significantly explained (See Figure 3). Model consistency and goodness of fit.
Goodness of Fit.

The validity analysis results indicate that all the items distinctly loaded on all constructs of fear of COVID-19, job insecurity, and subjective well-being of nurses have average loading of all items found >.7 on each construct. The average variance extracted (AVE) of the constructs ranged from .54 to .61, which exceeds the cut-off point of .50. The composite reliability (CR) and Cronbach’s alpha (α) values are also greater than .70 cut-off points. Furthermore, common method bias (CMB)-Harman’s single factor test was conducted to determine the systematic variance among the variables. A systematic variance may inflate the variance among relationships. Results indicated that 23% variance was explained by 1 factor, which is less than 50%; thus, it is acceptable.
Correlation Analysis.

Note: *** and ** indicates 1% and 5% level of significance.
Figure 4 depicts the significant and direct relationship between the fear of COVID-19 and the subjective well-being of nursing sector employees. Table 3 presents the moderating results; an interaction term was generated through SPSS AMOS to test the moderation effect of job insecurity on the relationship between fear of COVID-19 and subjective well-being. Firstly, fear of COVID-19 and subjective well-being were standardized in SPSS. Direct effect of the independent variable on the dependent variable. Moderating Effects of Perceived Job Insecurity in the Association Between Fear of COVID and Subjective Well-Being.

Furthermore, the interaction term was introduced, and lastly, the model was analyzed in AMOS after inserting the standardized values. Results again confirm the hypotheses of our study and indicate a significant direct relationship between fear of COVID-19 and the subjective well-being of nursing staff in hospitals. This association is significantly moderated by perceived job insecurity as an interaction of job insecurity is significant; the P-value is .000. The findings are also presented in Figure 5. Moderating effect of perceived job insecurity.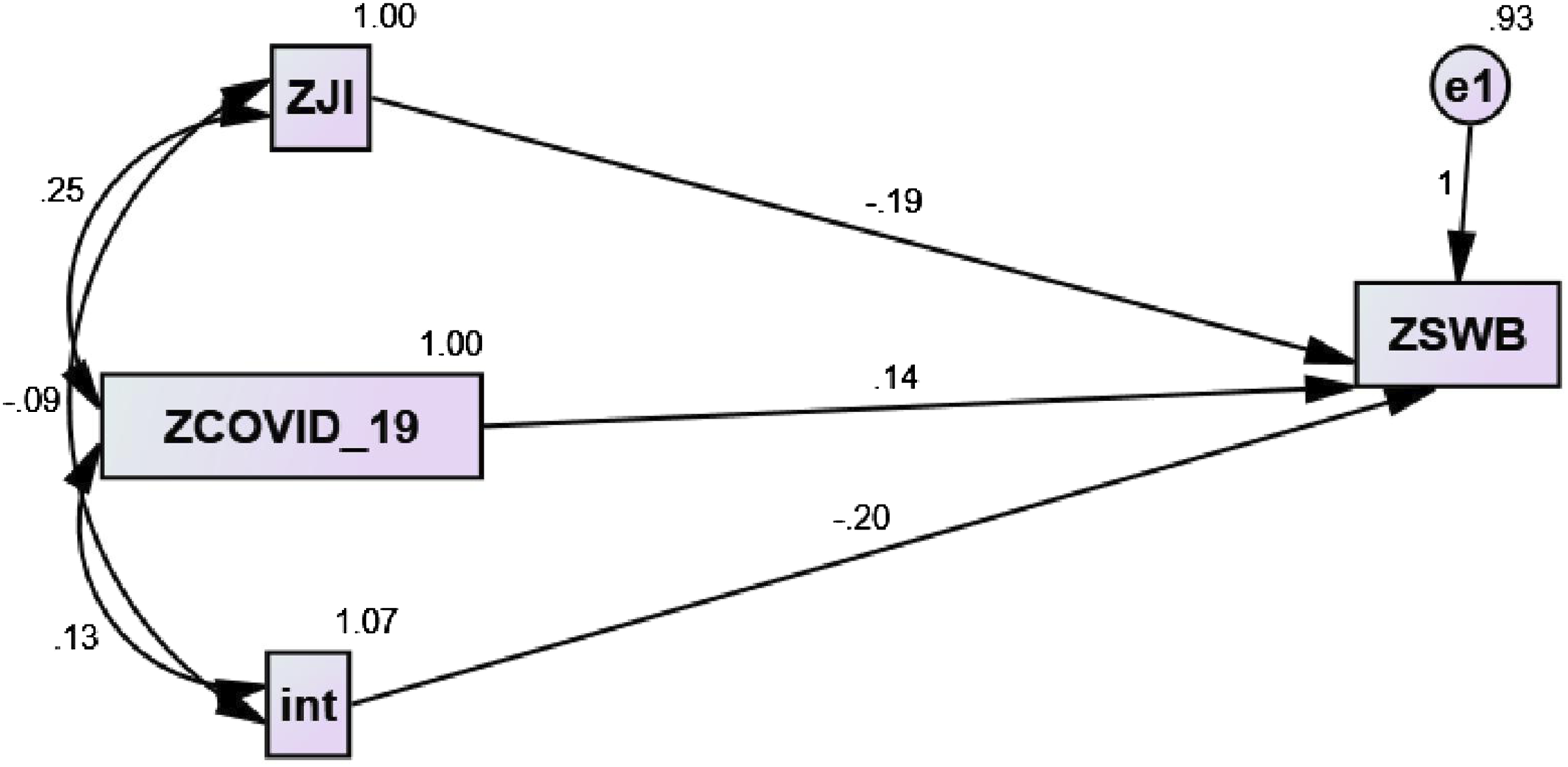
Our study’s findings show that the fear of the psychological fear of COVID-19 significantly undermines the well-being of the nursing staff of Pakistan. Our results are in line with the prior work that finds that the life satisfaction of the workers substantially undermines the mental stress caused by COVID-19 in different regions of China.62,63 Our study finds that fear of COVID-19 is creating a sense of job insecurity among employees. This finding is similar to research on the mental well-being of the public and health workers during the COVID-19 pandemic, which suggests that COVID-19 has a psychological impact on people’s lives.64-68 Both the fear of COVID-19 and job insecurity further trigger a negative influence on the workers' well-being. These findings are linked with the prior work undertaken on how job insecurity and stress of work have a significant impact on employees' well-being.69-71 Although our findings are intriguing, these findings are limited to Pakistan’s nursing sector only and might suffer self-selection bias. Thus, we urge the upcoming studies to contribute to different contexts and address self-selection bias.
Conclusions
Our findings have implications for Primary and Secondary Healthcare, the Punjab Health Care Commission (PHC), and for ways in which the management of public hospitals and regulators can deal with the fear of COVID-19, thus helping to ensure the mental well-being of their nursing staff. Our study highlights different factors, such as fear of COVID-19 and job insecurities among nursing staff, which undermine their well-being. Several researchers discussed plenty of strategies both for the nursing staff and for the management to overcome the fear of COVID-19 and mental stress within the public hospitals' nursing staff.17,37,69,70 These strategies are discussed below:
Staff, Colleagues, and Teams
1. Take opportunities to step away for short but unscheduled breaks, particularly when feeling under stress or strain. 2. Employ meditation and mindfulness techniques inside and outside of breaks. 3. Work for shorter shifts, and take enough time for recovery between working shifts. 4. Take proper care of oneself and colleagues, checking whether they have taken food and drinks and had proper rest. 5. Talk, assist and help your new colleagues who need support. Shared breaks, staff huddles and handovers, and team off-load sessions can be very useful.
Management and Policy Makers
7. Management should be visible and approachable to the nursing staff. From time to time, asking how staff are feeling may help and boost their morale. 8. Communication has very useful results. Regularly communicate with staff. When face-to-face contact is not possible, a concise and clear email may serve the purpose. Acknowledge the nursing staff’s needs, boost their confidence, show empathy, and value their contribution to helping COVID-19 patients. 9. Indicate to staff that their well-being is the priority of management. Implement mandatory work breaks and effective monitoring, and ensure there is individual and team support for each staff member. 10. Plan for shifts of nursing staff. Rotate their duties from high stress to low stress. Partner experienced and inexperienced nursing colleagues, and make sure there is a supportive culture. 11. Remove non-urgent and unnecessary business to reduce the workload and alleviate the staff burden. 12. Provide training for traumatic situations; convey the factual and coping skills necessary for potential mental health issues.
These strategies need to be implemented for nursing staff and other healthcare workers in hospitals in developing countries such as Pakistan. Although our study has interesting findings, it is limited to the nursing staff of public hospitals in Pakistan and does not generalize to the other sectors. Thus, we encourage more research regarding other non-health frontline sectors for future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the financial support of Hubei University of Economics to support the open-access of this article through its excellent Ph.D. program-wide grant number (XJ18BS06).