
Abstract
SARS CoV2 is a virus of which we know little and every day we have more information that clarifies us about its prognosis, reinfection is a new subject of which little is known, and it is important to determine its incidence, associated conditions and prognosis
The research shows the incidence of SARS CoV2 infection in a large cohort of patients, the characteristics associated with it, including the incidence of hospitalization and death in the second episode so that we have more information about the evolution of this new virus.
The implications are in theory because we make known about the evolution of the virus but also about policies because it helps to make decisions about public policies in the management of SARS CoV2
Introduction
The initial belief was that the natural infection caused by SARS CoV2 could produce total immunity after its occurrence, but more and more reports have demonstrated the probability of reinfection, although they continue being few, compared with the large number of global cases.1-3
In coronavirus cases, reinfection has been associated with short-term immunity and genetic changes in viruses which allow them to escape from immune response 2 ; these reinfections mainly occur in persons with mild disease, or asymptomatic, in which a fast decrease of antibody titers is noticed.4-6
Worldwide studies, carried out in more than 22 countries, have observed that there are significant differences in reinfection cases with respect to the initial infection, finding that 75% had mild symptoms and showing an increase in asymptomatic cases for second episode when compared to the first (9.2% vs 31.9%). 7
A suspected case of reinfection is defined when, 90 days after an initial episode of SARS CoV-2 infection confirmed by reverse polymerase chain reaction (RT-PCR) or a positive antigen test for SARS CoV-2, and the person again presents clinical symptoms compatible with COVID-19 (other possible explanations having been ruled out). A genomic confirmation between the virus of the first episode and the second infection is made to confirm the reinfection, this will demonstrate there are differences between the sequenced viruses, 8 being a difficult confirmation to achieve in our location due to the scarce availability of viral sequencing tests to verify that the viruses belong to different strains.
Although it is true that diagnosing the reinfection requires a complex laboratory infrastructure, the detection of suspicious cases of virus reinfection simpler since it does not require viral genotyping. For that reason, it is a more useful definition for the management of patients and monitoring reinfection. According to this, we present the cases with suspicion of reinfection in the Department of Valle del Cauca.
Materials and Methods
A descriptive retrospective study of repeated measurements was made with the positive population of Valle del Cauca identified since the beginning of the pandemic March 92 020, until June 30, 2021.
The department of Valle del Cauca is in the southwest of Colombia, in the middle of the Pacific region, between the western flank of the central mountain range and the Pacific Ocean. In 2019, there were 4 758 950 inhabitants in Valle del Cauca, a department with a total area of 21 195 km2, which represents 1.9% of the national territory, and is divided into 2 districts (Santiago de Cali and Buenaventura) and 40 municipalities.
The study only included cases presenting 2 reports of SARS CoV2 infection confirmed by RT-PCR or antigen tests, with a minimum difference of 90 days between the 2 episodes.
The record of positive cases in Valle del Cauca was taken from the database of positive cases executed by the National Health Institute (INS for its acronym in Spanish), which is fed by all territorial entities of the country, with data coming from other 2 national databases SIVIGILA and SISMUESTRAS At Valle del Cauca, the reported positive cases are registered according to the place of residence.
Statistical Analyses
A descriptive analysis of socio-demographic and clinical variables was made. Likewise, a comparison of the clinical variables between the first and second infections was made, using differences in proportions and non-parametric test for McNemar samples, for dichotomous variables of symptoms, hospitalization, ICU, and mortality.
Results
From March 9, 2020, until June 30, 2021, a total of 327 886 positive cases were identified in Valle del Cauca, out of which 3249 were considered as suspicious of reinfection. This corresponds to 1.1% of the cases. The median of days between the first and second episode was 182 days (IC 95%: 90 - 154 days). When analyzing the behavior by municipalities, it was found that the district of Santiago de Cali represents the highest reinfection rate of the Department, with 1602 cases per 1 000 000 inhabitants. Five
5
municipalities of Northern Valle del Cauca did not have any reinfection cases by the end of the study (Figure 1). SARS CoV2 reinfection rate in the different municipalities of Valle del Cauca.
Characteristics of reinfection cases.
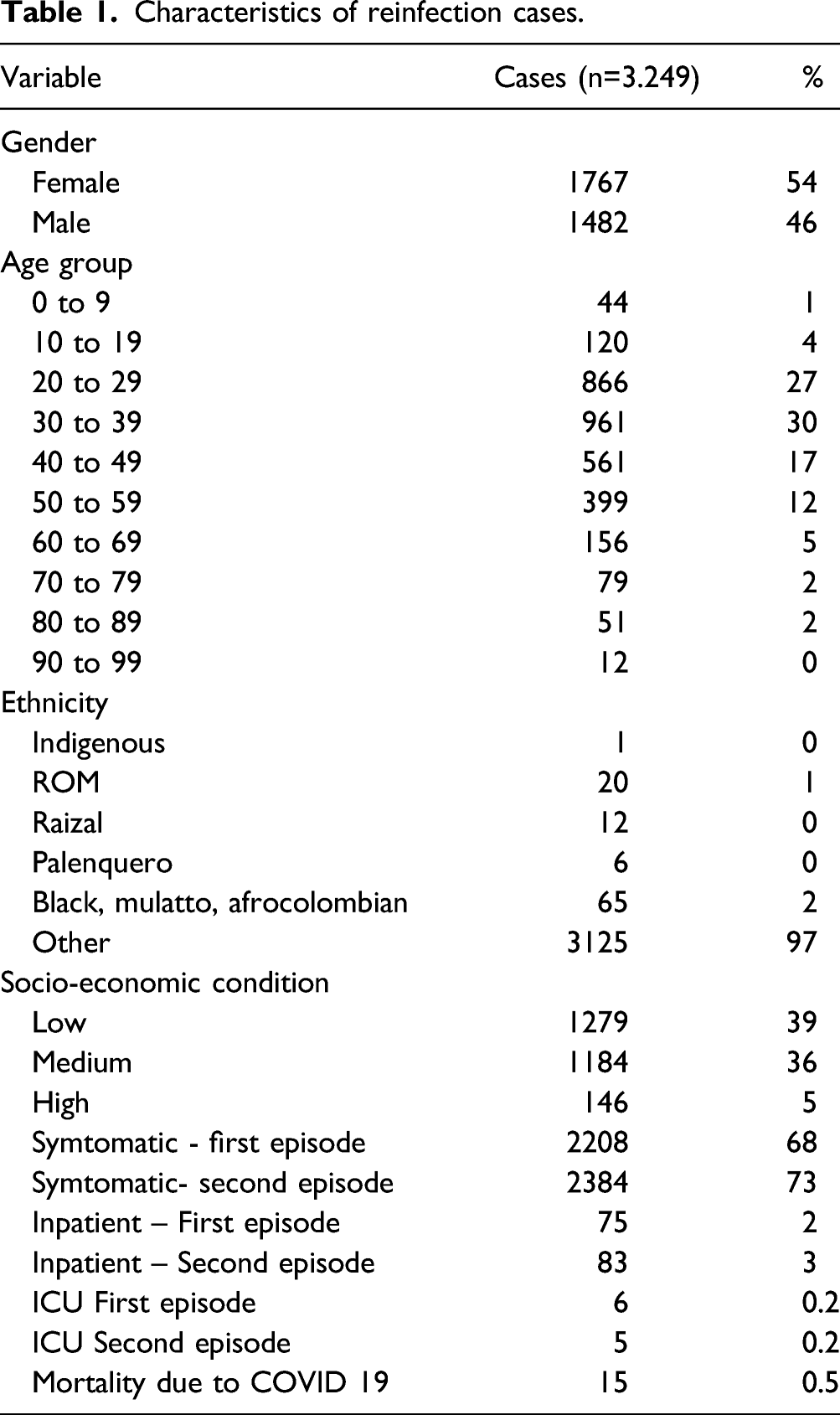
In terms of the occupation, 20.4% of the population had cleaning-related works, followed by 14.2% who worked as police authorities, with approximately 7% of workers in the healthcare sector, and a similar percentage of 7.3%, who were in the sales and trading sector.
We found a prevalence of 16.4% of pre-existing pathologies among reinfection cases. The preexisting pathologies investigated were arterial hypertension, diabetes, pathologies related to immunosuppression (primary or secondary immunodeficiencies or that require immunosuppressive drugs), chronic kidney disease, chronic lung disease including asthma. A relationship was found between the presence of reinfection and diseases related to immunosuppression (P < 0.05)
During the first infection episode, 68% of the patients had symptoms, while at the moment of reinfection, the percentage was 73.4%. 55% of the analyzed cases had symptoms in both infection episodes. It is important to mention that 81% of the cases with symptoms in the first episode, also had symptoms during the reinfection episode.
Non-parametric Mc Nemar test.

Likewise, the difference in measures between the categories of each of the socio-demographic variables and the presence of symptoms during both episodes was revised, finding a statistically significant difference between the different socio-economic strata and age groups with respect to the presence of symptoms, which was found in both episodes.
Differences between socio-economic variable categories.
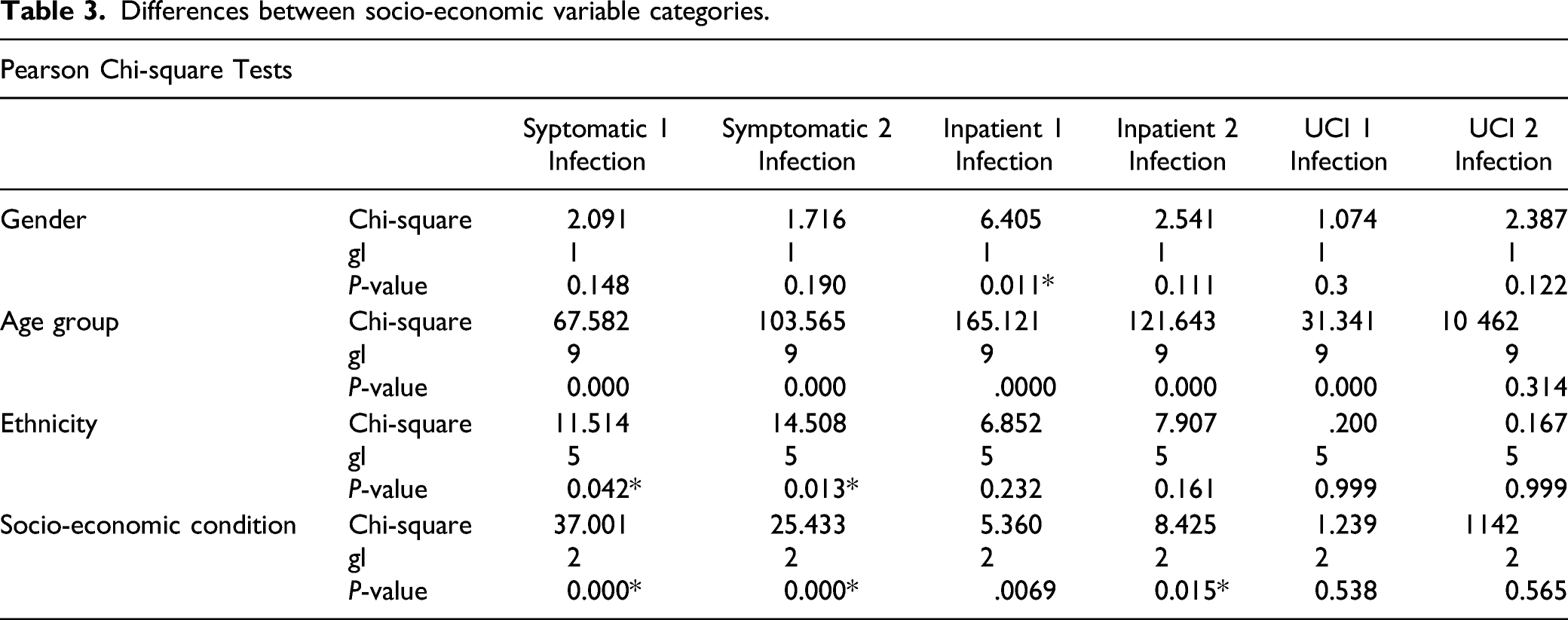
No significant differences were found between in-patients during the 2 infection episodes. However, a significant difference was found between the age groups and hospitalization, as well as between male and female during the first infection episode.
The outcome of reinfection cases showed that 15 patients (.5%) died, and 13% went to the ICU during the 2 episodes. Of the deceased patients, 53% had symptoms during the first episode and 73.3% during the second.
Discussion
COVID-19, up-to-date, has infected 224 million people, and 4.6 million have died at global level, 9 thanks to the replication and mutation capacity of this RNA virus and its expansion potential. In the world, new strains have been found on a daily basis. 10 Based on this theory and the report of suspicious reinfection cases due to the recurrent presence of acute, highly compatible signs and symptoms, and a positive PCR test, 11 studies were initiated to describe the reinfection of patients.
In August, 2020, the first reinfection cases through experiments in Macacus Rhesus 12 were documented, followed by different reports of cases in humans, where incidences between 2.4% and 69.2% 13 were observed, describing SARS-CoV2 reactivation episodes, viral residues with genetic material in upper airway after the initial infection, and genomic differences between both simples. 10
In this study, the reinfection percentage was 1.1%, a lower percentage than those of other series, which range between 2 and 12%.14,15 The average reinfection time ranges between 90 and 172 days, 16 but in our study, reinfection cases were from 90 to 154 days, as maximum limit. It is possible that with longer time, and a larger number of mutated strains, the SARS CoV2 reinfection cases increase. Therefore, long-term studies which include genotyping are necessary to confirm this hypothesis. More research and recommendations associated to the timely identification and management of reinfection in the Americas, Europe and Asia 3 are made on a daily basis due to the potential great impact on the healthcare systems of many countries of the world.
A systematic revision of literature published in March, 2021, analyzed more than 50 articles related to reinfection research carried out in 18 countries, which showed an average age of 49, with 54.9% being male, and with at least 66.3% of them having a pre-existing pathology. 13 Our study showed more reinfection cases in female (54.3%), in ages between 30 and 39, followed by those between 20 and 29 years of age. With regards to pre-existing pathologies related to serious COVID-19 illness, we found a prevalence of 16.4% among reinfection cases. The relation with underlying diseases is not considered as a risk factor for reinfection, except for pathologies which compromise the immune system. In those cases, there was a higher reinfection rate in older adults, which was also associated with an increase in pulmonary complications and hospital stays.5-7
Age is a factor that is widely linked to the behavior of the virus and the secondary immune response to the physiological reserve, establishing conditions of prognosis and severity.13,17 Case reports published in 2020 and 2021, with study populations in Asia, Europe, North and South America, found that reinfection cases cover a varied age range, documenting patients from 4 years to over 100, with a higher frequencies between the third and fourth decades of life, but with a higher risk of complications associated with admission to the ICU or the need for mechanical ventilation after 65 years of age,16,18 further increasing this condition before the presence of comorbidities, also being the age group with the highest number of deaths, although lower than what was found in the first episodes and with lower prevalence’s in younger populations 2 ; keeping a relationship with what is presented in our study.
With respect to the symptomatology, the studies describe most of the reinfected patients as asymptomatic, or with mild and moderate symptoms, predominantly respiratory or gastrointestinal. In our study, the presence of symptoms was of 17.7% in the second episode and 12.2% in the first infection. 55% of the patients included in the study had symptoms during both infections. Less than 15% of these patients required hospital management, and a low mortality. 13 In our research, the possibility of being hospitalized during the first episode was 1.2%, different from the second infection, with 1.4%, while the percentage for both infections was .8%. It is important to have in mind that these figures might represent an under-representation, since they are obtained from secondary sources and the hospitalization data may be slightly higher than the figures given here. The mortality rate was low, representing .8%. It calls our attention that out of the 15 patients who died, 13 went to the ICU during both episodes; these percentages are lower than those found in other studies where admission to the ICU was observed to be .5% for the first case and 1.7% for reinfection, and a mortality rate of 1.8% 7 ; therefore, this makes us think that such patients may have some type of individual susceptibility for a severe disease. It is important to make studies which may determine the individual mortality risk in patients with SARS CoV2 infection.
When we analyze the risk of reinfection based on occupations, we found that in addition to health workers, there are other high-risk professions such as cleaning-related works, police authorities and the sales and commerce sector. These professions have been related in the literature as professions of high/medium-high risk for COVID-19 related to the inability to perform remote work and ongoing exposure to the public, this kind of profession should be the key location for government actions to control COVID-19, and special consideration for vulnerable workers is warranted.19-21
In this study, the reinfection percentage was low, as well as the hospitalization and ICU cases. These results allow to define that in terms of the provision of healthcare services, reinfection defined in this study, does not generate any differences in care required vs the first episode. Therefore, measures taken to take care of these possible cases shall be the same as those established to take care of the pandemic, in accordance with the positive or negative new cases growth curve. In other words, it can be predicted that the reinfection cases will be 1.1% more than the projection of new cases, in a range from 3 to 6 months.
Given that the analysis was made overall positive cases of 1 of the most affected departments (states) since the beginning of the pandemic, and considering that the reinfection has a greater impact on the collective health, than the individual health, this study confirms the importance of maintaining epidemiological monitoring of the event, and continue with protocols to prevent large scale contagion, such as general vaccination, social distancing, and the use of masks under certain conditions, 22 but shall not change the public health and clinical management measures for primary infection cases, nor the management of later secondary infections due to SARS CoV2. 23
It is important to determine the relation between vaccination against SARS CoV2 and the appearance of post-infection episodes and the clinical presentation of the disease and verify the need to apply repeated dosages of vaccine to avoid later infections.
Within the limitations of this study is that data was obtained from the public health monitoring system (SIVIGILA) through routine notices. That means there can be under-registered figures in the information available for analysis. However, the territorial entity makes permanent efforts improving the coverage, quality, and timelines of the information. Another weakness of this study is the lack of molecular tests to determine the clonality between the first and second infection, which does not allow to confirm the above-mentioned cases as confirmed, maintaining them as suspicious.
Among the strengths of this study is the large size of the sample, being able to determine the affectation of the SGSSS with cases that had 2 infection episodes, within a period not less than 90 days. Despite being secondary data, in Colombia it is mandatory to report all suspicious and confirmed cases in the health surveillance system. Besides, there were 2 sources of data to avoid omissions, which makes improbable that a patient with a confirmed diagnose of COVID-19, skips this requirement. On the other hand, recognizing the reinfection level helps us guide the public health actions for the population and determine the need to continue with the general protection measures established in the department of Valle del Cauca.
Conclusions
Reinfection in SARS coV2 is a proven and possible phenomenon, in our study we found that the possibility of reinfection is greater in people between 20-39 years old, possibly related to being an economically active population. The probability of moderate and severe infection is similar to that of primary infection, reaching up to 15%, and the probability of death is 1.2%, similar to that of primary episodes of infection. It is important to consider the SARS CoV2 virus as the causal agent of respiratory pathology in all symptomatic people regardless of their previous infection status.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and Consent Statements
Our study did not require an ethical board approval because the data was taken of databases of public health surveillance. Among the ethical obligations of surveillance is to communicate the data to the community in general