
Abstract
Prostate cancer (PC) screening aims to detect PC in early stages, amenable to curative treatment and reduction in disease morbidity and mortality. However, PC screening may be associated with overdiagnosis and complications of unnecessary treatment for indolent disease. Therefore, careful patient selection for PC screening is critical to avoid overestimation and missed diagnosis. The aim of this study was to assess physicians’ knowledge and attitude towards early detection of PC in Jordan and whether their knowledge is an important predictor of their attitude. An electronic, self-reported questionnaire was used to collect data on demographics, knowledge, and attitude of physicians regarding early detection of PC. The participants’ responses were analyzed using descriptive statistics and multiple linear regression. Around 296 physicians agreed to participate in this study. Most respondents were males (75.7%), residents (34%), practiced medicine more than 15 years (29%) and graduated (81.4%) from local universities. Surprisingly, only 28.4% recognized PC as a non-self-detected disease and less than one-half (48.6%) were aware that PC screening tests are not enough to exclude a diagnosis of PC. The median knowledge Percent of Maximum Possible (POMP) score was 59%. Around two-thirds of participants showed a positive attitude towards early detection of PC (median attitude POMP score was 66%). Higher attitude scores were significantly associated with younger age, those working in private hospitals, and those having higher knowledge POMP score (P < .05). This study highlighted that most physicians demonstrated a positive attitude towards PC screening but with moderate level of knowledge that is considered an important predictor of their attitude towards PC early detection. Thus, improving knowledge and awareness of physicians should be considered as a strategy to improve their attitude towards prostate screening practices and informing men of the importance of regular screening.
Prostate cancer (PC) is one of the leading causes of death in Jordan and worldwide. Physicians’ knowledge and attitude towards early PC screening have not been evaluated before in Jordan Improving physicians’ knowledge could be considered as a strategy to improve their attitude towards prostate screening practices.What Do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications Towards Theory, Practice, or Policy?
Introduction
Worldwide, prostate cancer (PC) is the second most common leading cause of cancer in men and the fifth leading cause of death. 1 It is estimated that 248 530 new cases of PC will be diagnosed in the United States (US) in 2021 with 34 130 expected deaths. 2 PC incidence and mortality correlates with advanced age and 66 years as the average age at the time of diagnosis. 3 In Jordan, the incidence of PC represents 8.5% of all new cancer cases. Among the 5 165 979 males in Jordan, new PC cases in 2020 were 451 with 63 deaths. 4
Recent studies have shown that lower rates of PC incidence and mortality in several developed countries because of widespread use of Prostate Specific Antigen (PSA) testing to detect prostate cancer. 5 However, overdiagnosis and overtreatment remain a concern that needs to be addressed. A more cautious patient selection for PC screening is needed to improve the benefit to harm ratio.6,7 PSA testing is the most reliable biomarker for early detection, staging, and treatment monitoring of PC. 8 According to American Cancer Society (ACS), PSA testing is recommended to average risk men aged more than 50 years. For individuals at substantial risk of PC, screening starts at the age of 45. Candidate groups for early screening include African Americans and men with first-degree relatives diagnosed with PC at an early age (younger than 65). Further, those with more than one first-degree relative with PC at an early age, screening should take place at the age of 40. 9
Several studies have reported low rates of PC screening in Jordan10-13 due to a lack of knowledge about screening and early disease detection. 14 Although governmental support for implementing a national strategy of cancer control was one of the Ministry of Health strategic objectives for control of non-communicable diseases including cancer, Jordan does not have a national cancer control plan.15,16 Although all healthcare professionals could contribute to PC awareness, physicians have an essential role in improving PC knowledge and screening needs among their patients. Interestingly, in a recent meta-analysis by Peterson and colleagues, physicians’ attitude and recommendation have been shown to positively impact patient adherence to cancer screening. 17 Therefore, the aim of this study was to assess the knowledge and attitude of physicians towards PC early detection, and to assess the predictors of such knowledge and attitude.
Methods
Study Design, Setting, and Participants
A descriptive, cross-sectional survey was developed and used to assess knowledge and attitude of physicians toward early detection of PC in Jordan. The minimum sample size required for this study for multiple regression analysis was calculated using the formula proposed by Tabachnik and Fidell 18 :
N ≥ 50 + 8m. Where, m = Number of independent variables, since we have 9 independent variables, a minimum sample size of 114 was appropriately representative.
Many physicians were invited to participate in the study by posting the questionnaire link through social media websites. Several Facebook groups in Jordan including more than 20 000 physicians (Intern, general, resident, specialist, or consultant doctors) were used to distribute the survey. The largest Facebook group was “Hakeem” (https://www.facebook.com/Hakeem.joDrs/). The participants were informed about the purpose of the study prior to participation. Inclusion criteria include physicians who are currently in clinical practice. Exclusion criteria include medical students who did not obtain their MD degrees. The data were collected via self-reported questionnaire between November 2020 and September 2021.
Study Tool
The study questionnaire was adapted from Odedina et al and Alqudah et al questionnaires.19,20 The face and content validity of the questionnaire were tested by several experts in clinical practice and oncology research. Then, the questionnaire was piloted and distributed to a sufficient sample size (n=30). Adjustments were made (where necessary) based on the experts’ or/and pilot study participants’ comments. The following questions have been added before final validation of the questionnaire: Regular performance of DRE, percentage of patients who pay for their own health care in the health center and history of medical care to PC patients. Data collected during pilot testing were not included finally.
The questionnaire consisted of four sections with close end, multiple choices, and 5-points Likert scale questions (Appendix A). The first section consisted of 10 questions that collect participants’ demographics eg, age, gender, practice settings, years of experience, etc. The second section contained 3 questions asking participants about experience in dealing with PC patients.
The third section was designed for assessing participants’ knowledge about PC through 15 questions. The 1st question asked how confident the participants were in providing information about PC screening. The 2nd question assessed the knowledge about the most prevalent cancers in Jordan. The 3rd, 4th and 8th questions assessed the participants’ ability to identify PC risk factors while questions 7 and 13 assessed knowledge about PC prognosis. Questions 5 and 15 assessed the ability to identify eligible individuals to PC screening, while questions 10, 11 and 12 assessed the knowledge and practice related to PC screening tests. Questions 6, 9 and 14 assessed participants’ ability to detect suspected signs of PC. The answer to these questions were either “True,” “False” or “Not sure.”
The fourth section aimed to evaluate participant’s attitude towards early detection of PC with eight questions that assessed how the participants perceived: the benefit of raising patients’ awareness of PC (question 4) and PC screening (question 3), their responsibility of identifying individuals eligible for PC screening and possible PC signs and symptoms (question 5), their interest in providing PC education to the patients (question 6), the barriers of providing PC education such as: Time (question 2) and patient refusal (question 7), and their interest of having additional information about PC (question 1) and about early PC detection specifically (question 8). The answers to these questions were on 5-point Likert scale ranged from strongly agree to strongly disagree.
Measured Outcomes
A total knowledge and attitude scores were assigned to each completed questionnaire. Knowledge scores were assigned as the following: each correct answer (or correctly checked or correctly non-checked risk factor) received a score of 1, while incorrect or “Not sure” responses received a score of 0. The highest possible knowledge score is 22. Attitude scores were assigned as the following: for each statement reflecting a positive attitude, the participant scored 5 points for each “Strongly agree”, 4 points for each “Agree”, 3 points for each “Neutral”, 2 points for each “Disagree” and 1 point for each “Strongly disagree”. Whereas the statement reflecting a negative attitude, the participant scored 1 point for each “Strongly agree”, 2 points for each “Agree”, 3 points for each “Neutral”, 4 points for each “Disagree” and 5 points for each “Strongly disagree”. The possible attitude score range was from 8 to 40. The total knowledge and attitude scores were summed and standardized into Percent of Maximum Possible (POMP) using the following Equation:

Statistical Analysis
Following data collection, the survey responses were coded and entered a customized database using the Statistical Package for the Social Sciences (SPSS), Version 25.0 (IBM Corp., Armonk, New York, USA). Continuous variables were presented as means and standard deviations or medians and interquartile ranges depending on the normality of variables. Screening of potential predictors for participants’ attitude of the early detection of PC was carried out using simple regression analysis because the fewer variables included, the more accurate multiple regression model. 21 Potential predictors with P-value < .25 in the simple linear regression analysis were included in the multiple linear regression analysis. Multiple linear regression provides knowledge of the association of each predictor variable with the outcome after the effect of other predictors have been removed.22,23 A P-value of <.05 was considered statistically significant.
Results
Demographics and Clinical Practice Characteristics of the Study Participants
Socio-Demographic Characteristics of the Study Sample (n = 296).

Physicians’ Experience in Dealing With Prostate Cancer Patients (n = 296).

Participants’ Knowledge and Attitude Towards Early Detection of PC
Participants’ Knowledge About Prostate Cancer (n = 296).
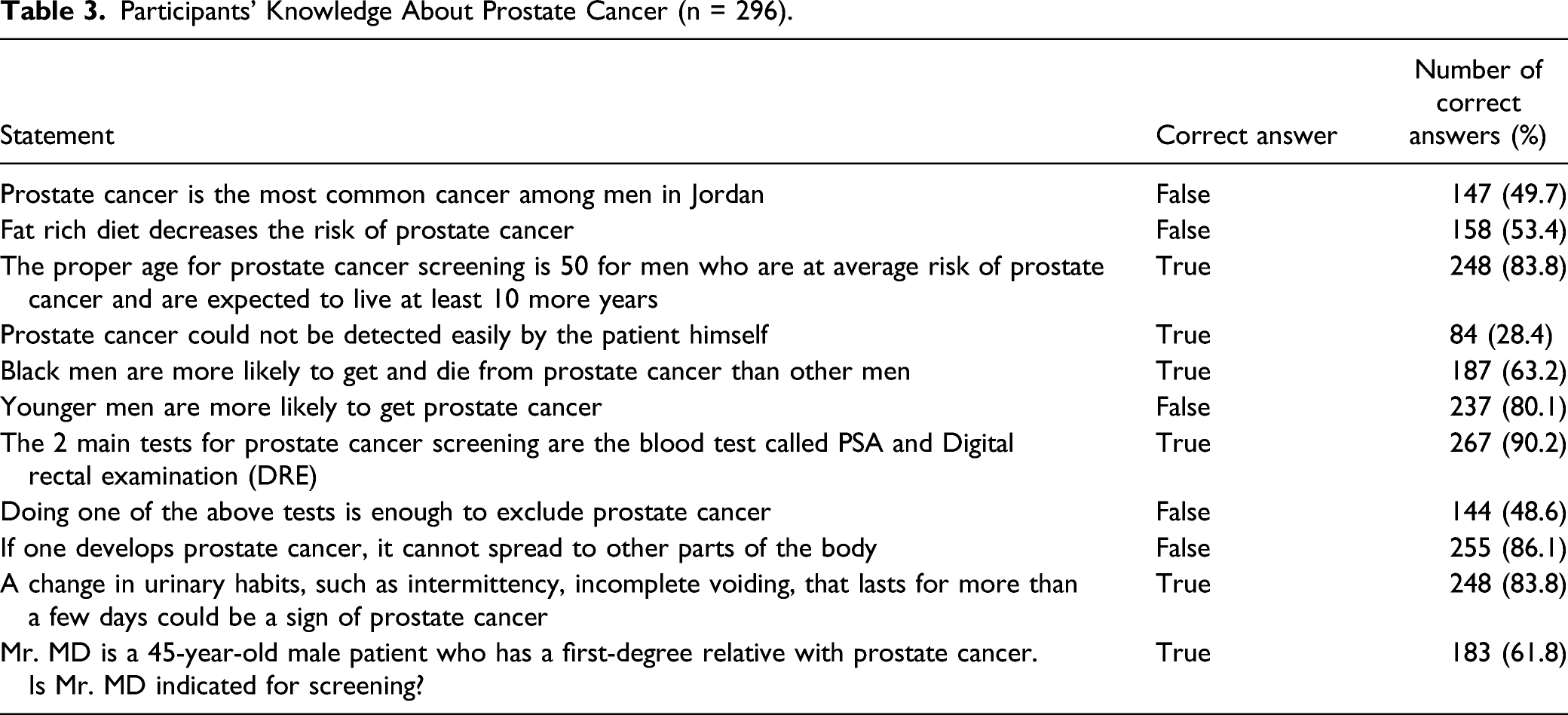
Figure 1 shows respondents’ performance on the drop-down questions asking about possible PC risk factors. Correct risk factors for PC were identified by 31-76% of respondents. The POMP knowledge score varied in a range of 23 to 91% with median score of 59% (IQR 13.6). PC risk factors identified by participants (n = 296); green color represents correct PC risk factors while red color represents incorrect PC risk factors.
Participants’ Attitude Towards Prostate Cancer Early Detection (n = 296).

aRepresent a negative attitude.
Simple Liner Regression to Assess Predictors of Participants’ Attitude Score (n = 296).

*Eligible for entry to multiple linear regression (P-value < .25).
Multiple Liner Regression to Assess Predictors Affecting Participants’ Attitude Scores (n = 296).

*Less than .05 was considered statistically significant.
Discussion
According to the World Health Organization (WHO), early cancer diagnosis has a significant impact on treatment success and achievable when disease education (knowledge) and encouraging subject involvement are combined in early detection practices. 24 In a previous study conducted in 2018 on Jordanian men awareness of PC, there was a remarkable lack of knowledge about PC screening among men aged 40 years or more. 25 However, according to the most recent reports, Jordanian men have the potential to gain knowledge and adherence to a healthy lifestyle for PC prevention through the implementation of a structured teaching program. Improved knowledge about illness and treatments has been shown to enhance adherence to healthy lifestyles. 26 The population’s attitude toward PC screening is primarily determined by the level of knowledge and quantity of provided information.10,27,28 Proper information and recommendations from physicians are the most important factors in enhancing the screening practices. It has been found that physicians’ recommendation is the most important factor affecting PC screening practices.10,27 Although this study was conducted to assess the knowledge and attitude of physicians, it is also important to inform the healthy male population about the incidence of PC and how to screen for it. In a recent study conducted in Italy, Morlando et al have shown that around 50% of men’s knowledge about PSA testing was provided by their physicians. 29 This underscores the importance of the need for increasing physicians’ knowledge and awareness which in turn will to increase the target population knowledge of PC screening.
In the present study, we assessed physicians’ knowledge and attitude towards early PC detection for the first time in Jordan. The level of knowledge was moderate; the median knowledge score was 59%. This is comparable with what was reported by Afra et al 30 where the mean knowledge score was 54.3% in Saudi Arabia. More concerning was the finding that most of our study participants were unaware that PC is asymptomatic in its curable stages (72%) and that PSA testing or DRE are insufficient to exclude PC (51%). In fact, a recent systematic review and meta-analysis showed that DRE has a sensitivity of 51% and a specificity of 59%. 31 Although 71% of participants indicated that they could provide PC early detection counseling, only 28% routinely screen patients older than 50 or in their 40s with risk factors. Nonetheless, these findings were higher than international reports where only 1% of responding physicians routinely screen more than 80% of male patients over 50. 32
Most participants had a positive attitude; the median attitude score is 66%. The majority of participants accepted their responsibility of prostate early detection and screening. In addition, most participants recognized their role in providing information and recommendation on PC screening. Finally, most participants are interested in learning more about PC.
The results of multiple linear regression demonstrated that knowledge, age and practice setting are the major predictors of physicians’ attitude. Our findings revealed that higher knowledge scores were associated with a better attitude towards providing PC early detection education and screening. These findings were consistent with Arafa et al findings that PC knowledge level was a major determinant of physicians’ attitudes. In addition, this study indicated that the major barriers of providing PC counseling and screening perceived by physicians were lack of knowledge and skills. 30 Together, these findings emphasize that raising the awareness of physicians about PC early detection will improve their attitude toward their responsibility in providing information and education on early PC screening. In this study, younger physicians showed a better attitude toward early PC detection. These findings were consistent with previous studies in which age and knowledge were the main determinants of physicians’ attitude towards PC screening. 30 In contrast, Hicks et al indicated that younger physicians had lower attitude level towards PC screening. 33
Recent European studies have established a robust European screening model to avoid unnecessary biopsy procedures, underdetection, overdiagnosis and overtreatment via introducing modern technologies such as risk calculators (RCs) and magnetic resonance imaging (MRI).7,34,35 The algorithm starts with risk-based PSA testing, followed by multivariable risk stratification with RCs that incorporate several variables including PSA, DRE, age, %free PSA, transrectal ultrasound (TRUS), previous biopsy status, and MRI results.7,34,35 However, MRI availability might be an issue in countries such as Jordan. Therefore, the use of PSA in healthy males, aged between 50 (45 in risk-groups) and 70 years followed by a risk stratification and using PSA density (PSA related to the prostate volume) could be the modality of choice in PC screening to significantly reduce overdiagnosis and overtreatment.7,34,35
Limitations
Since physicians’ responses were self-reported and not guided by experts, they might not accurately represent actual practice.
Conclusion
To date, this is the first study in Jordan that has assessed physicians’ knowledge and attitudes toward early detection of PC. Although most physicians have a positive attitude towards PC early detection, their knowledge level was inadequate. Our findings indicate that physicians’ knowledge is an important predictor of their attitude towards PC early detection. Thus, raising physicians’ awareness of early PC detection must be considered as a strategy to improve physicians’ attitude and practices of PC screening tests. Future research should be focused on identification of proper education means to improve the physicians’ knowledge about early PC detection. Applying novel algorithms utilizing PSA and RCs as in the European model could be the modality of choice in PC screening to significantly reduce overdiagnosis and overtreatment.
Supplemental Material
Supplemental Material - Early Detection of Prostate Cancer: Self-Reported Knowledge and Attitude of Physicians in Jordan
Supplemental Material for Early Detection of Prostate Cancer: Self-Reported Knowledge and Attitude of Physicians in Jordan by Mohammad A. Y. Alqudah, Raneem Al-Samman, Obada Matalgah, and Rana Abu Farhah in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
We are grateful to Jordan University of Science and Technology (JUST) for support and obtaining ethical approval
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Consideration
This study was conducted after obtaining the Institutional Review Board (IRB) approval from Ethics Committee at Jordan University of Science and Technology (JUST) (Approval # 42/137/2021).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.