
Abstract
Health insurance programs have the potential to shield individuals in low- and middle-income countries from catastrophic health expenses and reduce their vulnerability to poverty. However, the uptake of insurance programs remains low in these countries. We reviewed existing evidence from experimental studies on approaches that researchers have tested in order to raise the uptake. In the 12 studies we synthesized, educational programs and subsidies were the dominant interventions. Consistent with findings from previous studies on other health products, subsidies were effective in raising the uptake of insurance programs in many contexts. Conversely, education interventions—in their current forms—were largely ineffective, although they bolstered the effect of subsidies. Other strategies, such as the use of microfinance institutions and social networks for outreach and enrollment, showed mixed results. Additional research is needed on effective approaches to raise the uptake of insurance programs, including tools from behavioral economics that have shown promise in other areas of health behavior.
Keywords
Highlights
What do we already know about this topic?
Although health insurance has the potential to protect individuals from catastrophic health expenses and to reduce their vulnerability to poverty, participation in insurance programs remains low in low- and middle-income countries. There is limited evidence on effective approaches to increase participation.
How does your research contribute to the field?
We collated existing evidence on approaches that researchers have tested in order to raise the uptake of insurance programs. We focused on experimental and quasi-experimental studies, thus alleviating concerns about drawing evidence from studies with significant methodological limitations.
What are your research’s implications towards theory, practice, or policy?
The study provides insights into tools and strategies that can be leveraged to promote enrollment in health insurance programs in low- and middle-income countries. Thus, it is a useful reference for both development agencies and governments.
Introduction
Globally, approximately 150 million individuals experience catastrophic health expenditures each year and 100 million of them are pushed into poverty because of these expenses. 1 Over 90% of the individuals impoverished by healthcare expenses reside in low- and middle-income countries (LMICs).2,3 In response, governments in these countries have attempted to implement health insurance and social protection programs of varying scale and approach—all as a part of a broader effort toward universal health coverage and the attainment of the Sustainable Development Goals.
Notable forms of such programs include social health insurance (SHI), national healthcare insurance (NHI), and community-based health insurance (CBHI). The overarching objective of these programs is to protect the poor from the effects of unforeseen healthcare expenses by reducing out-of-pocket costs. A detailed description of these insurance models can be found elsewhere. 4 Briefly, SHI schemes involve contributions from the individuals, the employer, or the government, and are usually enacted through a statute of law. 5 In these schemes, the amount of contribution and the coverage do not depend on an individual’s health risk profile. NHI, sometimes called a single payer system, involves a single purchaser—usually the government—paying for a package of services on behalf of the population within a geographic area. 6 Finally, CBHI programs are local schemes with arrangements for pooling and mobilizing contributions from members. 7 Typically, CBHI programs are based on voluntary membership, are not-for-profit, and offer a predetermined package of benefits to the beneficiaries. 8
Despite the potential of these insurance programs to protect individuals from catastrophic healthcare expenses, their uptake is low across LMICs, and ranges between 5% and 25%.9,10 To date, we have a limited understanding of effective approaches to increasing the uptake. Two previous reviews have attempted to fill this gap.11,12 However, both reviews covered only CBHI programs and identified the broad determinants of the uptake of such schemes. In the current review, we built on that work and synthesized evidence from experimental and quasi-experimental studies on various approaches that researchers have tested in order to increase the uptake of health insurance programs and to promote retention. We did so for all types of health insurance programs in LMICs. Based on our synthesis, we identified several areas for further research that can help inform the design and implementation of future interventions.
Methods
We conducted a scoping review of experimental and quasi-experimental studies on health insurance interventions in LMICs following the framework of Arkey and O’Malley (2005). 13 In line with the framework, our steps included specifying the research question(s) for the review, identifying relevant studies, charting data from the selected studies, and synthesizing the findings.
Search Strategy
We retrieved records using PubMed (Medline), CINHAL, and PsychINFO electronic and Google Scholar databases. A number of search terms were combined using AND and OR Boolean operators with the help of a librarian to retrieve the studies (see Appendix 1), separately from each database. We imported and assessed the retrieved studies for eligibility following the guidelines in COVIDENCE, a web-based software for scoping and systematic reviews. 14 After removing duplicate studies, the first author screened abstracts and full-text documents using an agreed set of inclusion and exclusion criteria (see below).
Inclusion and Exclusion Criterion
We included primary research articles that met the following criteria: (1) the study design was either a randomized controlled trial (RCT) or a quasi-experiment, such as a difference-in-difference analysis; (2) the study examined health insurance uptake as one of the primary outcomes; (3) the study was based on SHI, CBHI, NHI, or a ‘mixed’ scheme—the common types of health insurance programs in LMICs; and (4) the country of study was classified as a LMIC by the World Bank. 15 We limited the sources to studies published in English between 2000 and 2022. A study was excluded if it met one of the following criteria: (1) only the abstract was available; (2) the study was based on forms of insurance other than health insurance (e.g., life insurance, livestock insurance); (3) the study used a case-control, cross-sectional, or qualitative design; and (4) the publication was an opinion piece, editorial, commentary, or a review.
Data Charting
We extracted data from the selected studies into a predesigned charting table. The data included country of the study, type of insurance program studied, and the study’s main objective(s), key intervention(s), and main findings. We pretested the chart on three of the included studies to ensure feasibility, completeness, and consistency of data extraction, and iteratively refined the chart as needed. We adapted the Cochrane Risk of Bias Assessment tool to formally assess the quality of the studies. 16 We evaluated six potential sources of bias: selection, performance, detection, attrition, reporting (see Appendix 2). The two authors independently reviewed the sources and assigned an overall score for quality (high, medium, low, or unclear). Score disagreements were resolved through discussion.
Results
Our initial search retrieved 1605 studies, of which 297 were duplicates (Figure 1). Of the remaining 1308 studies, 981 were excluded because they were not related to the study question and 315 were removed because they did not use an RCT or a quasi-experimental design or because they did not include enrollment as one of the outcomes. This resulted in 12 studies in the final review.

PRISMA flow diagram.
Overview of the Included Studies
The 12 studies covered 10 countries (Table 1). Three studies were conducted in Burkina Faso17-19 and one study was conducted in each of the following countries: Ghana, 20 India, 21 Indonesia, 22 Kenya, 23 Mexico, 24 Nicaragua, 25 the Philippines, 26 Senegal, 27 and Vietnam. 28 In terms of the type of insurance program, three of the studies examined the effect of their interventions on the uptake of CBHI programs,17,19,27 six on the uptake of SHI,18,20,21,24,26,28 and three on NHI.22,23,25 Method-wise, 10 of the studies were RCTs,17,20-28 while the remaining two were quasi experiments.18,19
Summary of the Studies Included in the Review.
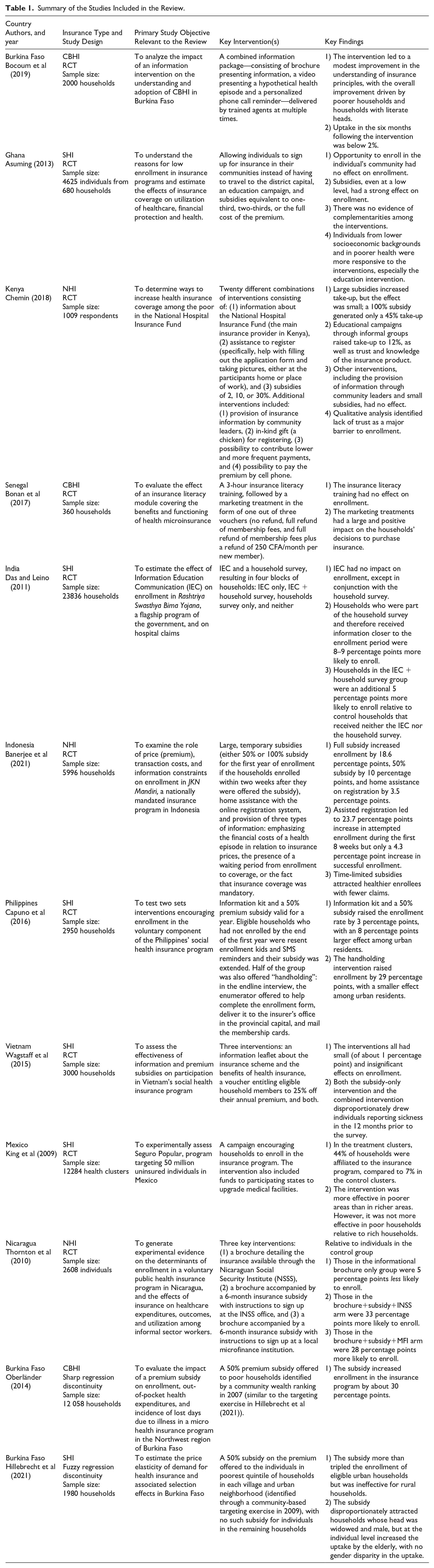
Before synthesizing the studies’ findings, a brief summary of each study is in order. In Africa, Bocoum et al (2019) analyzed the effect of providing information through multiple avenues (specifically, a brochure presenting factual information, a video presenting a hypothetical health episode and a personalized phone call reminder) by trained agents on the adoption of CBHI in rural Burkina Faso. 17 Asuming (2013) examined the effect of three interventions in northern Ghana: allowing individuals to sign up for insurance in their communities instead of having to travel to the district capital, an education campaign, and subsidies equivalent to one-third, two-thirds, or the full cost of the premium. 20 The author then used the resulting variation in insurance coverage to estimate the effect of enrollment on utilization, out-of-pocket expenses and health outcomes. In this review, we focused on the first of part of their study. Chemin (2018) investigated the effect of three key interventions—information about health insurance, assistance to enroll, and small subsides of 2, 10 or 30% of the membership fee—on uptake of in-patient health insurance in Kenya. 23 Finally, Bonan et al (2017) tested the effect of an insurance literacy module covering the benefits of health microinsurance and the functioning of local CBHI schemes, and that of three marketing treatments—specifically, varying levels of subsidies on membership fees—in Senegal. 27
In Asia, Das and Leino (2011) conducted an information and education campaign in the context of India’s flagship program, Rashtriya Swasthya Bima Yojana. They used a household survey as an intervention to gauge the extent to which surveys alone can alter the likelihood of enrollment. 21 Banerjee et al 22 (2021) investigated the effect of large, temporary subsidies, at-home registration assistance, and the provision of three types of information—emphasizing the financial costs of a health episode in relation to insurance prices, the presence of a waiting period from enrollment to coverage, or the fact that insurance coverage was mandatory—on enrollment in Indonesia’s JKN Mandiri program. 22 Capuno et al (2016) tested two sets of interventions—information and a 50% premium subsidy—encouraging enrollment in the voluntary component of the Philippines’ social health insurance program. A year after the initial intervention, the researchers re-sent the enrollment kits and SMS reminders and extended the subsidy to those who had not enrolled. Half of the group was also offered “handholding”: in the endline interview, the enumerator offered to help complete the enrollment form, deliver it to the insurer’s office in the provincial capital, and mail the membership cards. 26 Wagstaff et al 28 (2016) conducted a similar experiment in Vietnam, where they offered households one of three interventions: an information leaflet about Vietnam’s government-run scheme and the benefits of health insurance, a voucher entitling eligible household members to 25% off their annual premium, or both. 28
In Latin America, King et al 24 (2009) assessed the effect of a campaign encouraging households to enroll in Seguro Popular, Mexico’s insurance program, on catastrophic expenditures, medication spending, and health outcomes and utilization. 24 The intervention also included funds to participating states to upgrade medical facilities. Finally, Thornton et al (2010) offered different combinations of information, subsidy and enrollment location to informal workers in Nicaragua, and examined effects on out-of-pocket expenditure and healthcare utilization, among others. 25 Specifically, they randomized participants into one of three offers: a brochure detailing the insurance available through the Nicaraguan Social Security Institute (NSSS), a brochure accompanied by a 6-month insurance subsidy with instructions to sign up at the INSS office, or a brochure accompanied by a 6-month insurance subsidy with instructions to sign up at a local microfinance institution.
The two quasi-experimental studies, both from Burkina Faso, estimated the effect of a premium subsidy on insurance enrollment using a regression discontinuity (RD) design.18,19 In early 2000s, the government of Burkina Faso provided a 50-percent subsidy on the insurance premium to poor households. The eligibility for the subsidy was determined by a community-based wealth ranking. The two studies compared insurance uptake among individuals on the two opposite sides of the eligibility cutoff in an RD framework. 29
Commonly Tested Strategies and Their Effectiveness
Educational Campaigns
One of the two previous reviews identified the lack of understanding of how insurance works as one of the major barriers to enrollment in insurance programs. 12 Not surprisingly, 10 out of the 12 studies in our review tested some form of an educational intervention. In Table 2, we provide details of each educational intervention, covering the key approaches used, the content of the educational material, the medium of dissemination, the timing of the educational campaign in relation to when the insurance was offered, and whether the study assessed the effect of the educational campaign on participants’ knowledge directly.
Description of Studies that Used an Education Intervention.

The most common education approaches were door-to-door campaigns and workshop-based group education. In both approaches, the participants were provided with information kits—primarily brochures and booklets—containing information about the insurance program, its premium and, the benefit package, the registration procedure, and any applicable subsidies.20,23,25 In most cases, the education materials were distributed by trained insurance agents who also answered questions from the potential enrollees. The information kits aimed to ensure that potential enrollees, including those with limited education, understood the principles of insurance. These kits utilized “easy to read text,” pictorial cues, and cartoons.21,23 One study provided an extended training covering topics such as personal financial management, savings, risk management, and insurance. 27
The timing and intensity of the educational campaigns differed across studies. In several studies, the offer to sign up for insurance was made concurrently with the provision of education, while in others education preceded the offer of enrollment—by a few weeks to a few months.21,22 The most intensive education intervention was conducted in Burkina Faso, where researchers combined an informational brochure with a video tutorial and phone call reminders. 17 Other approaches to reinforcing education included follow-up visits by trained agents,20,21 phone text reminders, 26 and the use of community leaders for enrolling individuals into insurance programs. 23
Although an improved understanding of an insurance program is often required for individuals to enroll in the program, only two studies assessed whether the knowledge provided by the researchers increased recipients’ understanding of insurance principles and the health insurance product offered.17,20 The remaining studies did not directly assess the effect of their education interventions on knowledge.
In terms of the effects on uptake, the majority of the studies found that education did not increase enrollment in insurance programs. Even in Burkina Faso, where a modest improvement in understanding of insurance principles was found among the participants, enrollment after 6 months was below 2%. 17 Based on this finding, Bocoum et al (2019) concluded that the demand for insurance enrollment was inelastic to information and that the lack of information was not a major barrier to the uptake of insurance in that context. In Nicaragua, those who received the information brochure were approximately five percentage points less likely to enroll in the insurance program than those in the control group who received nothing; 25 the information intervention worked in the opposite direction of what was expected.
The strongest effects of education were observed in Kenya, where information kits were disseminated via existing informal community groups such as cooperatives, clubs, and churches. This intervention capitalized on existing trust among individuals in informal social networks, reporting a 12% increase in insurance uptake as a result of the intervention. The uptake sustained for a year.
Based on their study in Senegal, Bonan et al (2017) argued that the observed lack of the effect of education on insurance uptake may be explained by a number of factors, including the quality of the education module or the participants’ prior expectations about the insurance product. They argued that overly optimistic prior expectations may make insurance products less appealing once the details are known. This could also help explain the counterintuitive results reported in Thornton et al (2010).
The effect of education on enrollment may also depend on the timing of education, as Das and Leino (2011) showed in India. In their experiment, the education campaign, which was launched two months before the insurance policy was offered, had no effect on enrollment. However, households that were surveyed and therefore received information through the interviewers closer to the enrollment period were significantly more likely to enroll. Based on this finding, the authors suggest increasing information “dosage” (i.e., reinforcing earlier educational messages during subsequent visits for a survey) as a way to increase enrollment. 21 However, this finding on “dose–response” contradicts the finding by Bocoum et al (2019) in Burkina Faso, where a “repeated” engagement yielded only modest gains in knowledge about insurance and no improvement in uptake. 17
Subsidies
The provision of subsidies was the second most common intervention used to raise the uptake of insurance programs. Six out of the 10 RCTs and the two quasi-experimental studies tested the impact of subsidies on enrollment. The subsidies were provided to the potential enrollees predominantly in the form of a premium subsidy.
The amount of subsidy, frequency, and timing varied across studies. The amounts ranged from no subsidy to a 100-percent subsidy, with a 50-percent subsidy on the premium the most common. The intervention households in the Philippines study received a 50% premium subsidy in the first year of enrollment. 26 Those in the Kenya study received varying levels of subsidy (2%, 10%, and 30%), in addition to informational package and registration assistance. 23 The intervention households in Ghana received a full subsidy totaling GHC 12.20 ($8.13), while those in Nicaragua received six-month insurance premium subsidy worth approximately US$96.20,25 As mentioned earlier, the two quasi-experiments from Burkina Faso were based on a 50-percent subsidy provided to poor households.18,19
Generally, the studies reported a positive effect of subsidies on enrollment. For example, in rural Burkina Faso, the 50-percent subsidies increased insurance uptake by approximately 30 percentage points. 19 The program in Indonesia offered time-limited subsidies—only available for two weeks after the offer was made. This unique feature was meant to resemble an insurance market where limited time period for enrollment is intended to safeguard against moral hazard. 22 In the study, a full subsidy increased enrollment by 18.6 percentage points, while a 50% subsidy increased enrollment by 10 percentage points. 22 These subsidies also attracted lower-cost individuals, thus reducing adverse selection—a common problem in health insurance markets. 22
Previous studies focusing on other preventive health products such as deworming pills, use of insecticidal treated bed nets, vitamin supplements, water chlorine, and handwashing soap have concluded that demand for these products are highly price sensitive.30,31 Dupas and Miguel (2017) have summarized the findings of these studies and provided a demand curve for these products (see Figure 2, page 46). 32 For comparability, in Figure 2, we show the demand curve for insurance programs based on information extracted from the studies in this review. The figure shows the relationship between insurance uptake expressed as a percentage (x-axis) and the effective price individuals face, also expressed as a percentage (x-axis). Consistent with the demand curves for other health products, the demand for insurance is sensitive to prices. Unfortunately, raw data on baseline premiums rates in these studies were not available for us to calculate the elasticities and compare them with those reported for other health products. It was also not possible to assess if there was a sharp dampening of demand when a positive price was charged (that is, going from a small subsidy to no subsidy), as small subsidies were uncommon in the included studies.

Insurance uptakes rates by the level of subsidy.
Other Strategies
Apart from education and subsidies, several other strategies were used to improve enrollment in insurance programs, often in combination with education and subsidies. They included: (1) offering registration in the communities, thus making it more convenient to enroll;20,25 (2) “handholding”—insurance agents helping enrollees to fill out and submit forms to central registration offices;22,23,26 (3) using social networks for education and enrollment; 23 and (4) offering enrollment through local institutions such as microfinance institutions. 25
Evidence on the effectiveness of these approaches was mixed. For example, the decentralization strategy in which enrollment facilities were brought closer to the customers was effective in raising enrollment in Nicaragua and Indonesia, but had no effect in Ghana.20,22,25 Relatedly, “handholding” raised enrollment by 29 percentage points in the Philippines, with a smaller effect among urban residents than among rural residents. 26 However, using community leaders to disseminate information, providing in-kind incentives (chickens) upon registration, or allowing payments from mobile platforms did not increase enrollment in Kenya. 23
Complementarity vs Substitutability Between Information and Subsidies
The question of whether subsidies and educational campaigns are complements or substitutes is of interest to policymakers.33,34 If the two are complements, one bolsters the effect of the other, thus making the combined effect greater than the sum of individual interventions. Conversely, if they are substitutes, their effects may offset each other, thus reducing the benefits of implementing them together.
The studies that tested information and subsides together suggested a strong complementarity between the two in some contexts but not in others. In the Philippines, the combination of information and a 50% subsidy increased enrollment by five percentage points. 26 In contrast, the combined information-subsidy intervention had no effect in enrollment in Vietnam. 28
The combination of education campaigns or subsidies with other “conveniency tools” yielded mixed results. For example, combining a premium subsidy and personal phone reminders increased enrollment by 36 percentage points in the Philippines, but adding a conveniency component (decentralization of registration offices) in Ghana had little to no additional effect on enrollment.20,26
Heterogeneous Effects Across Dimensions of Socio-Economic Status
It is possible for the interventions described above to have different effects on different socio-economic groups, even within the same country. An understanding of these differential effects is important for effective targeting of future interventions. Five out of the 12 studies in this review examined heterogeneous effects of their interventions on enrollment.17,18,20,26,27 The common dimensions across which heterogeneous effects were assessed include income, education, and rural vs urban.
The Burkina Faso and Ghana studies examined heterogeneous effects across income. In both studies, the effect of subsidies was stronger among poor households compared to their rich counterparts.17,20 The differential effect was more pronounced when subsidies were combined with education. 17
The Ghana and Senegal studies reported heterogeneity in effects across the education gradient. In Ghana, households with an educated head were more responsive to the interventions, particularly the one that combined information and subsidies. 20 However, there was no differential impact of education on insurance uptake in Senegal. 27
The Philippines study examined heterogeneity by urban versus rural residency. The effect of the main intervention (informational kit plus 50% premium subsidy) was 8 percentage points higher among the urban residents than among the rural residents. 26
Hillebrecht et al (2021) showed that, in Burkina Faso, halving the insurance premium increased enrollment among poor urban residents by more than three times but was largely ineffective for rural residents.
Discussion and Conclusion
Our scoping review included 10 RCTs and two quasi experimental studies from LMICs. We found that educational campaigns and subsidies were the two most common interventions that have been tested to increase enrollment in insurance programs in these countries, and that subsidies were generally effective in raising enrollment. This finding is consistent with evidence on other health products, where reducing subsidies—effectively raising the price—has been shown to dampen demand.35,36
Country-specific findings reported above should be understood in the context of that country’s economic status, the healthcare system, and existing health insurance programs and policies. These contexts have been discussed in detail elsewhere.37-47 However, these countries have a number of common features. First, only a small percentage of the population in these countries is covered by insurance programs. Second, these countries are experiencing a rapid surge in non-communicable diseases, which impose substantial financial burden to households in absence of health insurance. 48 A third common feature is the presence of a larger informal sector, which limits the share of the population that can be covered through employer-based insurance programs. The large informal sector also poses logistical challenges for collecting taxes and insurance premiums, as would be needed to fund the insurance programs.
While educational campaigns may be necessary in many LMICs given poor understanding of insurance principles in these settings, 8 the existing literature suggests that education alone is not sufficient to increase enrollment in insurance programs. Depending on the setting, this may be due to a range of factors, including limited decision-making power of those selected to receive the educational intervention (e.g., women) or simply the poor quality of the education provided.17,27 Indeed, a prior review has shown that there are many determinants of enrollment in insurance programs in LMICs, including age, gender, educational attainment, location, household size, socio-economic status, and marital status. 12 Put differently, there may be several intertwined barriers—beyond the lack of education—to which the education programs may not have catered.
This review was restricted to experimental studies, which provided casual estimates of the effect of the intervention on insurance uptake and are less prone to methodological limitations than cross-sectional studies. Nonetheless, our study had a number of limitations. While we did a comprehensive database search for references, some studies may have been missed. Furthermore, we only included peer-reviewed publications in English; non-English sources and experiments that may have been reported in evaluation and technical reports of NGOs and development agencies have not been captured.
Despite these limitations, this review provides useful information for governments and development practitioners. The review suggests that governments aiming to raise enrollment in insurance programs should primarily consider ways to address financial barriers that individuals face. Policymakers need to strike a balance between maximizing access to services for the needy population and minimizing benefitting those who can afford insurance without any subsidy, 32 as large-scale subsidies are not feasible and sustainable in many LMICs.
Given the limited breakthrough with using conventional education campaigns and limited feasibility of subsidies, there is a critical need to test additional interventions. Of note, except for a few exceptions (e.g., Bonan et al, 2017; Thornton et al, 2010) studies have yet to capitalize on social institutions, such as trust within a network, to encourage the uptake of insurance. Socially organized informal groups such as churches, cooperatives, burial societies, and community clubs are ubiquitous in many LMICs, but their potential for changing health behavior—in this case, encouraging enrollment in insurance programs—has been tested explicitly only in a few contexts.
Future experiments should examine whether the use of health information technology as used in high income countries can be adapted to LMICs. 49 While current efforts in high income countries—such as the possibility of enrolling for insurance online in the US—may appear ambitious in LMICs, mobile phones are now widely used in LMICs and have shown promise in a range of areas from raising adherence to antiretroviral therapy for HIV to promoting immunization. Such technologies can help tackle multiple barriers to the uptake of health insurance, ranging from inconvenience and transport costs to the lack of information.
Future studies can also explicitly test techniques from behavioral economics that have been utilized in other areas of health to alter behavior. Decisions about whether to enroll in an insurance program can be affected by a range of behavioral factors—including default and present biases. Relatedly, literature in public administration in high-income countries suggests that learning, psychological and compliance costs associated with interacting with the government can also deter individuals from utilizing government services. 50 The extent to which the education intervention in the studies included in this review catered to these factors is not clear.
Finally, in several LMICs, only expenses incurred at designated health facilities are covered by insurance programs. 51 In those cases, the uptake of insurance may depend on the quality of the services in participating health facilities. A few studies included in this review had interventions targeted to health facilities. However, to our knowledge, no study has examined the effect of the quality of care on the uptake of insurance.
Footnotes
Appendix 1. Search Strategy
Appendix 2. Quality Assessment of the Studies Included in the Review

| Study | Risk Assessment Parameter | Risk Level | Basis of Judgment | Overall Quality |
|---|---|---|---|---|
| Bocoum et al (2019) | Random sequence generation | Medium | Not specified | High |
| Allocation concealment | Low | Treatment households randomly selected | ||
| Blinding of participants and personnel | Low | Treatment assigned at village level, except in one set of villages | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the experiment | ||
| Incomplete outcome data | Low | Attrition of 4.5%, but no evidence of differential attrition | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Hillebrecht et al (2021) | Random sequence generation | N.A. | Quasi-experimental study design | High |
| Allocation concealment | Medium | Eligibility for subsidy determined in the village | ||
| Blinding of participants and personnel | Medium | Eligibility for treatment determined in the village | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the study | ||
| Incomplete outcome data | Low | Not reported | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Oberländer (2014) | Random sequence generation | N.A. | Quasi-experimental study design | High |
| Allocation concealment | Low | Eligibility for subsidy determined in the village | ||
| Blinding of participants and personnel | Medium | Not feasible due to nature of intervention | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the experiment | ||
| Incomplete outcome data | Low | Not clear | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Bonan et al (2017) | Random sequence generation | Low | Random number generator used | High |
| Allocation concealment | Low | Treatments randomly assigned at the household level | ||
| Blinding of participants and personnel | Low | Small number of households selected from a large area | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the experiment | ||
| Incomplete outcome data | Medium | Compliance rate was 58% | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Capuno et al (2016) | Random sequence generation | Low | Computer generated random numbers used | High |
| Allocation concealment | Low | Randomization at the municipality level | ||
| Blinding of participants and personnel | Low | Randomization at the municipality level | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the experiment | ||
| Incomplete outcome data | Medium | Attrition rate not clear | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Chemin (2018) | Random sequence generation | Medium | Not specified | High |
| Allocation concealment | Low | Households assigned to arms randomly | ||
| Blinding of participants and personnel | Medium | In some groups, staff provided info. and helped with registration | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the experiment | ||
| Incomplete outcome data | Low | No evidence of incomplete outcome data | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Asuming (2013) | Random sequence generation | Medium | Not specified | High |
| Allocation concealment | Low | Randomization at community level | ||
| Blinding of participants and personnel | Low | Randomization at community level | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the experiment | ||
| Incomplete outcome data | Low | No evidence of incomplete outcome data | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Das and Leino (2011) | Random sequence generation | Medium | Not specified | High |
| Allocation concealment | Low | Households randomized into interventions | ||
| Blinding of participants and personnel | Low | Only 3000 households received the intervention | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the experiment | ||
| Incomplete outcome data | Medium | 27% of households could not be reached for household visits | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Thornton et al (2010) | Random sequence generation | Low | Randomization was conducted using a lottery system | High |
| Allocation concealment | Low | Individuals randomized into intervention arms | ||
| Blinding of participants and personnel | Medium | Not specified | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the experiment | ||
| Incomplete outcome data | Low | Follow-up rates were above 90% across all groups | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Wagstaff et al (2015) | Random sequence generation | Low | An online randomization tool was used | High |
| Allocation concealment | Low | Households were randomized into arms | ||
| Blinding of participants and personnel | Medium | Not specified | ||
| Blinding of outcome assessment | Low | Outcome measures preidentified before the experiment | ||
| Incomplete outcome data | Low | Attrition rate between baseline and end surveys is just over 1% | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| King et al (2009) | Random sequence generation | Medium | Not specified | High |
| Allocation concealment | Low | Matched pair cluster randomized experiment | ||
| Blinding of participants and personnel | Low | Randomization was at the health cluster level | ||
| Blinding of outcome assessment | Low | Expected results published before data analysis | ||
| Incomplete outcome data | Medium | Not clear if loss-to-follow-up was differential across arms | ||
| Selective reporting | Low | No evidence of selective outcome reporting | ||
| Banerjee et al (2021) | Random sequence generation | Low | Randomization conducted using CSPro (see trial registry) | High |
| Allocation concealment | Low | Randomization at household level | ||
| Blinding of participants and personnel | Low | Not specified | ||
| Blinding of outcome assessment | Low | Outcomes preidentified, and measured using administrative data | ||
| Incomplete outcome data | Low | Some individuals could not be matched with govt. data, but the missingness was not differential across arms (footnote 14) | ||
| Selective reporting | Low | Trial was pre-registered |
Notes. The framework above is taken from Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ WV. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2. 2021. The five risk assessment parameters are intended to capture the following types of bias: selection bias (in absence of random sequence generation and allocation concealment), performance bias (in absence of blinding of participants and research personnel, detection bias (in absence of pre-determined outcome), attrition bias, and reporting bias.
Acknowledgements
We would like to thank Katherine Phillips at the Pennsylvania State University for providing guidance on the search strategy. We would like to acknowledge support from Penn State’s Population Research Institute, which is supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The open-access publication of this article was made possible through financial support from the Department of Health Policy & Administration at the Pennsylvania State University.