
Abstract
Objective
To systematically evaluate the effects of Tai chi for improving elderly patients with type 2 diabetes.
Methods
According to PRISMA checklist, we conducted this standard meta-analysis. The multiple databases like Pubmed, Embase, and Cochrane databases were used to search for the relevant studies, and full-text articles involved in the evaluation of Tai chi in improving elderly patients with type 2 diabetes. Review manager 5.2 was adopted to estimate the effects of the results among selected articles. Forest plots, sensitivity analysis and funnel plot for the articles included were also conducted.
Results
Finally, 7 relevant studies were eventually satisfied the included criteria. We found that Tai chi group had lower glucose than control group (mean difference (MD)=-12.47, 95%CI [-21.20, −3.73], P=.005; I 2 = 32%), Tai chi group had higher activities-specific balance confidence (ABC) scale than control group (MD =9.26 with 95%CI [6.68, 11.83], P < .001) and Tai chi group had higher single limb standing test score than control group (MD = 8.38, 95%CI [4.02, 12.74], P = .001). The study was robust and limited publication bias was observed in this study.
Conclusion
Since we found Tai chi had better performance than usual care in improving old diabetes patients' glucose and life quality, the study supports that Tai chi can help old diabetes patients from several aspects including disease indicators, independence and life quality.
Introduction
Reducing the incidence rate and mortality rate of diabetic patients and improving their quality of life are important public health goals. Scientists studying the diabetes prevention program have found that people can reduce the incidence of diabetes and its complications by losing weight (5%–7% of body weight), eating a healthy diet (low fat, low calorie) and increasing physical activity1-3. Among the self-care behaviors that affect blood glucose control and diabetes complication prevention, regular exercise is one of the most problematic and underutilized therapies in diabetes management.4-6 Tai chi is a form of traditional Chinese martial arts, which is being practiced as a physical and mental health exercise. Research shows that Tai chi is related to good changes of blood lipid, lowering blood pressure, and improving aerobic endurance.7-9 Diabetes hurts nerve conduction in the central and peripheral nervous system, resulting in postural instability by altering peripheral nerve function. 10 Other consequences of diabetic peripheral neuropathy include reduced balance, strength, and gait parameters, which may be an intermediary factor leading to a high risk of falls in patients with diabetic peripheral neuropathy. 11 Due to the inability to produce appropriate neuromuscular responses, patients with diabetic peripheral neuropathy showed increased swinging amplitude and swing area. The reduction of balance may also lead to a decrease in physical, emotional, and social functions and ultimately harm the quality of life. 12
Tai chi uses slow movements, breathing exercises, and meditation. This kind of training is low impact. In this kind of training, diaphragmatic breathing is coordinated with graceful movements to achieve spiritual tranquility.13-17 Tai chi is practiced in a squatting position. Exercise intensity can be easily adjusted by controlling the angle of the knee joint (elderly subjects will use the high squat position, while healthy young subjects will use the low squat position). The classic Yang’s Tai chi has 108 postures and some repetitive sequences.18-20 Each training includes about 20 minutes of warm-up, 24 minutes of Tai chi and 10 minutes of calmness. The slow and gentle movements of Tai chi use all the main muscle groups and joints of the body, increase the strength of the muscles and joints, and improve balance, flexibility, endurance, range of motion, and coordination.21-23
In patients with diabetes, ankle varus and valgus, anteroposterior, and medial lateral plane of the body movement also decreased. All of these physical indicators not only proved the increased instability of this group, but also found that diabetic patients had lower safety when standing and walking compared with healthy people.24-26 Although a large number of studies have been done to determine how and when these complications manifest in patients, few interventions have been made to restore some or all of the functions that have been lost.27-29 One study looked at how fingertip touch improves postural instability in patients with diabetes and peripheral neuropathy, but this intervention does not improve sensation or function; it uses an alternative input (finger touch) to increase the information being processed to achieve balance.30-32 Therefore, it may be necessary to improve the posture stability and sensory ability of patients with diabetes. Tai Chi Program can enhance the physical strength of patients, increase the body resistance, relax the spirit of patients, and eliminate the tension of cerebral cortex.
In recent years, the effects of Tai chi have been noted, but the detailed role of Tai chi in improving elderly patients with type 2 diabetes has not been fully understood. Here, we conduct a meta-analysis to confirm the effects of Tai chi in old diabetes patients' glucose and life quality.
Methods
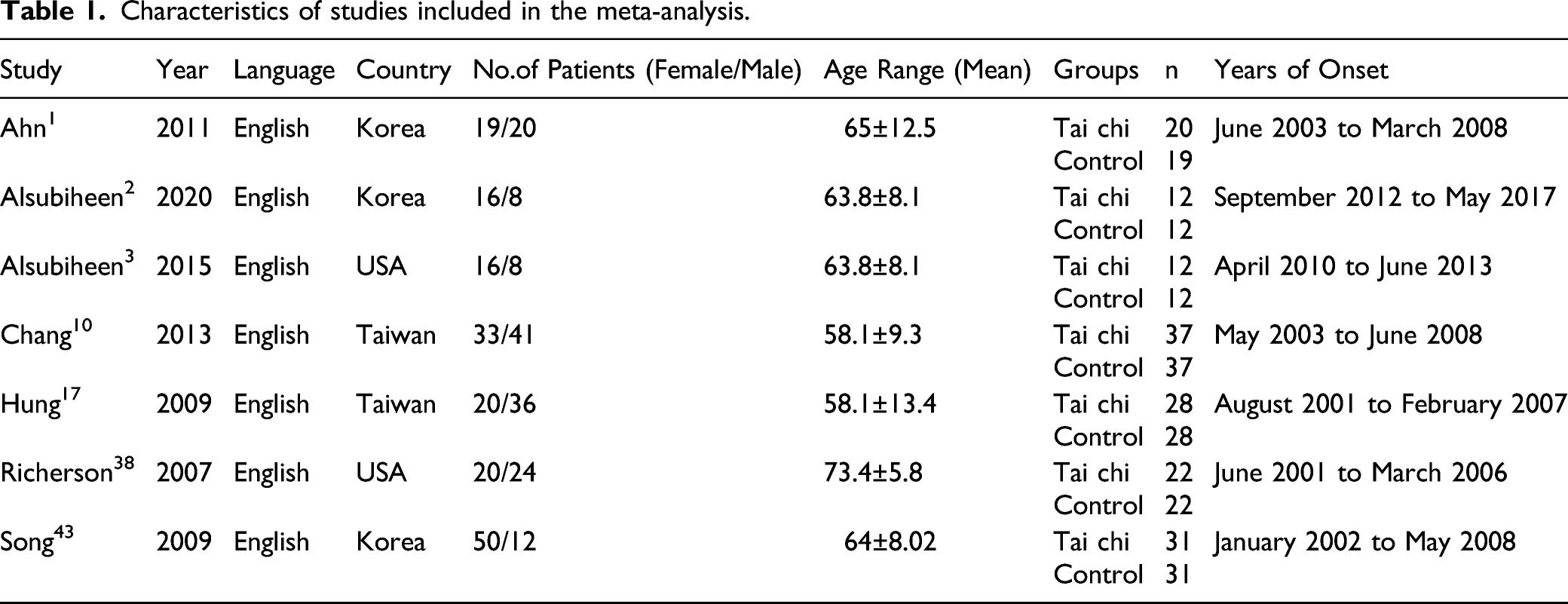
Characteristics of studies included in the meta-analysis.
Search Strategy
We started systematic search from databases: PubMed, Embase, Cochrane library, and China National Knowledge Infrastructure (CNKI) from available papers in literature up to Jan 2021 for potentially eligible studies. For the search, we used the Mesh term of “tai chi” and “diabetes mellitus” and their relevant key words. The reference lists from retrieved studies were reviewed to identify any new eligible study. The searching details was shown in Figure 1 following PRISMA checklist. Flow diagram of the study selection.
Study Selection
The inclusion criteria were as follows: (1) Population: elder patients (more than 55 years old) with diabetes mellitus type 2. (2) Intervention: Tai chi. (3) Control: Usual care. (4) Outcome: glucose (mg/dL), activities-specific balance confidence scale and Single limb standing test. (5) Study: RCTs (6) No language limitations.
The exclusion was as follows: (1) Patients without diabetes mellitus type 2 or not elderly patients. (2) Data in research is limited or insufficient. (3) They were duplicates.
Combining the keywords searching and inclusion/exclusion criteria, we conduct the literature searching in 4 main databases: PubMed, Embase, Cochrane library, and China National Knowledge Infrastructure. The details of searching would be shown in search process section.
Data Extraction and Quality Assessment
Two of the authors independently reviewed the formal published versions of all eligible studies for content and screened them according to the specified inclusion criteria using a data extraction form based on the Cochrane Consumers and Communication Review Group’s data extraction template. Disagreements were resolved by discussion between the 2 review authors; if no agreement could be reached, it was planned a third author which would decide. The following data were extracted: (1) Study characteristics: first author’s name, country, sampling size, age and gender of the patients, intervention arms, and follow-up. (2) Outcomes: if the study reported mean value, we will extract mean value and standard deviation, if not, we will collect events and total in 2 arms. (3) Studies on same sample from different articles, the interested outcomes, longest follow-up and interested population was chosen.
The validity of eligible RCTs was assessed using the Cochrane risk of bias tool in Review Manager 5.2. Funnel plots were planned to evaluate the risk of bias across studies (Liu et al, 2013).
Statistical Analysis
A χ2-based test of homogeneity was performed, and the inconsistency index (I 2 ) statistic was determined. Mean difference and corresponding 95% confidence interval (CI) were used to summarize the results. The statistical heterogeneity of these studies was calculated by Cochran’s Q test and I 2 index (more than 50%, P < .1, high heterogeneity). Considering that a large number of people from different regions in each study are different, and different variables are adjusted in different studies, a random effect model is adopted to avoid possible heterogeneity. Meanwhile, if I 2 index was less than 50%, a fixed effect model was adopted. We assess possible publication bias by funnel plot. All analyses were performed using review manager (version 5.2, Cochrane Collaboration, 2011). We also tried to conduct a sensitivity analysis based on the quality and weight of the test, and exclude each individual test in turn.
Search Process
A preliminary search found 905 related publications, of which 63 were excluded from duplicate publications. After filtering by title and abstract, 49 articles remain. Forty two studies were excluded due to unsatisfactory article types and insufficient data. Finally, select 7 articles for meta-analysis. The research selection process is shown in Figure 1.
Results
Characteristics of Included Studies
The detailed characteristics of the included studies are shown in Table 1. All these studies were published from 2000 to 2021. The sample size is between 24 and 74. There were 162 cases in the Tai chi group and 161 cases in the control group.
Quality Assessment
The methodological quality of the studies was evaluated by the quality assessment tool in Cochrane manual. Figures 2 and 3 show the quality assessment in this study. As we have seen, there is limited bias in the included articles. Only one study showed the problem of attrition bias (Richerson and Rosendale, 2007). From the perspective of deviation summary, there is no problem with selection deviation, performance deviation, detection deviation, and reporting deviation. Generally speaking, only 1 trial has a risk of bias and 6 trials have no risk. Assessment of the quality of the included studies: low risk of bias (green hexagons), unclear risk of bias (yellow hexagons), and high risk of bias (red hexagons). Risk of bias was assessed with use of the Cochrane risk-of-bias too.

Outcomes of Meta-analysis
Forest plot about glucose
Five studies involve in glucose between Tai chi and control groups using fixed effect model and it was shown in Figure 4. The result suggested that there was significant difference in glucose (MD=−12.47, 95%CI [-21.20, −3.73], P = .005; I
2
= 32%). We could find that Tai chi group had lower glucose than control group and the mean difference is −12.47 which mean that the difference was small (about 10% of raw data). Meta-analysis about ABC scale Forest plots of glucose between Tai chi and control groups.

In the analysis, 3 articles were included. The results of heterogeneity test showed that random effect model wad was needed to analyze the data (I
2
= 91%). The overall effect of ABC(activities-specific balance confidence) scale was significant and mean difference was 9.26 with 95%CI [6.68 and 11.83] and overall P value was < .001 (Figure 5). The result showed that Tai chi group had higher ABC scale than control group. Since the MD was 9.26 which is also about 10% of raw data in both groups, the difference between 2 groups is small. Meta-analysis about single limb standing test Forest plots of ABC scale between Tai chi and control groups.

In the analysis, 4 articles were included. The results of heterogeneity test showed that fixed effect model wad was needed to analyze the data (I
2
= 45%). The overall effect of single limb standing test was also significant and the mean difference was 8.38 with 95%CI [4.02, 12.74] and overall P value was .001 (Figure 6). Tai chi group had higher single limb standing test score than control group. In this part, the MD was 8.38 and it was more than 50% of raw data in both groups, which indicated that the difference in single limb standing test was big. Forest plots of single limb standing test between Tai chi and control groups.
Sensitivity Analysis and Publication Bias
To examine the stability of the outcome, a sensitivity analysis was needed. When Ahn’s article in 2011
1
removed, the result demonstrated that in heterogeneity part, I
2
of sensitivity changed from 32% to 47%. It indicates that the heterogeneity is steady (Figure 7). Sensitivity analysis forest plots of glucose between Tai chi and control groups.
To assess publication bias in this study, a funnel plot was conducted. The result of funnel plot suggested that no significant evidence of potential publication bias existed (Figure 8). Funnel plot of publication bias.
Discussion
From our results, we can find that glucose in Tai chi group was lower than control group. In analysis of ABC scale, Tai chi group was higher than control group. About single limb standing test, Tai chi was also higher than control group. Therefore, from these 3 different aspects, we can find Tai chi can help old diabetes patients in disease control, life independence and balance ability.
According to the U.S. Centers for disease control, 8.6 million or 18.3% of adults 65 and older have diabetes. Due to many physiological systems affected by the disease, diabetes research has been focused on identifying possible complications and their causes, and intervention measures to improve the quality-of-life of patients with diabetes are limited.33-35 Fear of falling and loss of balance are 2 major complications of diabetes and aging. The elderly and diabetics are usually slow to respond. Over the years, the loss of balance of payments has been very serious. Falls increase medical costs for the elderly.36-39 Yue and Xue reported that Taijiquan can effectively reduce blood glucose and HbA1c and improve most psychological aspects of quality of life during regular practice for more than 6 months. Tai Chi combines physical exercise and meditation based on balancing airflow. The influence of shadowboxing on diabetes control may be related to the aerobic exercise components of Taijiquan, but Qigong relaxation exercise may also affect blood glucose control. 40 This is consistent with our study.
Tai chi, as a traditional exercise method, has been used to improve balance and posture control in China. It is called a physical and mental skill, because people use their brains when they do exercises.41-44 Tai chi is a kind of comprehensive movement, including the slow coordination of gravity shift, posture adjustment and synchronous deep breathing. This combination involves many different psychological and physiological factors, such as calmness and concentration in exercise, following the example of the coach, reaching the appropriate form to improve muscle elasticity, and combining exercise with deep breathing to improve cardiac output and provide sufficient blood flow for muscles.45-48 Xiao and Zhuang show that Taijiquan is a potential method to promote and accelerate the “relearning” process. It can improve balance and gait, and more importantly, prevent falls 49 and this is also consistent with our results.
In a cross-sectional study of the elderly, Tai chi practitioners reported significantly higher quality of life in most subscales of SF-36. 50 Even after controlling for demographic variables, the improvement in quality of life was significantly related to the number of years and frequency of practicing Tai chi.51-53
In previous studies, diabetic patients who exercised Tai chi for more than 12 weeks reported higher cutaneous vascular conductivity and better peripheral nerve conduction velocity of bilateral median and tibial nerves.54-56 These findings suggest that Tai chi exercise can improve sensory function and neuropathy related symptoms. Previous studies57,58 have also shown that elderly people with peripheral neuropathy have improved plantar sensation after 24 weeks of Tai chi exercise. With the improvement of plantar sensation, Tai chi training can help the subjects to control their posture better and get better balance. The effect of Tai chi exercise on the balance of the elderly or diabetic patients has also been fully supported by the literature.59-64
Above all, the results showed that Tai chi had better performance than control group in evaluation of glucose and life quality including balance and independence. This is consistent with several reported articles. However, some limitations existed in this article. First, more indicators evaluating other aspects should be included, and this could be conducted in the future. Second, more researches from various countries and subgroup by different race couldbe analyzed in the next research. Third, we included only a small number of studies, and the small patient population may increase bias in the analysis.
Footnotes
Acknowledgments
We would like to acknowledge the nursing and medical staff that generously took the time to participate in this study.
Author Contributions
[(This will be published with your article. Please provide authors’ initials as appropriate)]
Criteria
Author Initials
Made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data.
Yanmei Wang, Pei Yang, Wenhui Zhang
Involved in drafting the manuscript or revising it critically for important intellectual content.
Yanmei Wang, Jianjun Yan, Peng Zhang, Min Lu
Given final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Yanmei Wang, Jianjun Yan, Peng Zhang, Pei Yang, Wenhui Zhang, and Min Lu
Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Yanmei Wang.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by the Key Disciplines of Pudong New Area Health System(Grant No. PWZxk2017-10) and Funded by Talent Project of Shanghai Pudong New Area Gongli Hospital(Grant No. GLRI2018-01).