
Abstract
Children in food-insecure households have an increased risk of anemia. Participation in Supplemental Nutrition Assistance Programs (SNAP) has several benefits. However, it is unknown if it ameliorates anemia among school-aged children and adolescents living in food-insecure households. This study aims to assess the association of SNAP participation and anemia among children and adolescents living in households experiencing food insecurity. The sample population (n = 1635), aged 6 to 18 years, were pooled from the 2003–2014 National Health and Nutrition Examination Survey (NHANES). The exposure of interest was self-reported household SNAP participation. The outcome variable was the presence or absence of anemia, classified using the blood hematocrit concentration values. Survey weighted logistic regression was performed to calculate the odds ratio (OR) and 95% Confidence Interval (CI) of the association between participation in SNAP and anemia in food-insecure children. We found that over 80% of anemic children and adolescents, living in food-insecure households, participated in SNAP, while 63% of non-anemic children and adolescents, living in food-insecure households participated in SNAP (p = .007). Among children living in food-insecure households, SNAP participants had 3-fold increased odds of anemia compared to those who do not participate in SNAP, after adjusting for confounders (OR = 3.33, 95% CI: 1.25–8.88). In this study, SNAP participation was associated with increased odds of anemia in children and adolescents living in food-insecure households. Additional research is needed to assess if these unexpected findings are related to the adequacy of SNAP, affordability, and accessibility to healthy foods, or the household and individual food preferences in food-insecure households.
Keywords
Highlights
Supplemental Nutrition Assistance Program (SNAP) is associated with several health benefits; however, very little is known about the association between SNAP participation and anemia among children and adolescents living in food-insecure households.
Children and adolescents living in food-insecure, SNAP-participating households are more likely to have anemia, contrary to expectations.
More research is needed to explore the program structure, as well as the individual, household, and environmental factors associated with SNAP participation, to better understand the observed association between SNAP participation and anemia among children and adolescents living in food-insecure households.
Introduction
Food insecurity, defined as “inadequate access to enough food for all household members to live an active and healthy life” is a social determinant of health.1-3 In 2018, 13.9% of United States (US) households with children experienced food insecurity, with the proportion of Black and Hispanic households with food insecurity estimated to be 21.2% and 16.2%, respectively. 4
Food insecurity is a predictor of diseases in adults.5-7 Earlier studies, conducted among US adult populations, have reported associations between food insecurity and chronic diseases.7-9 Specifically, studies have demonstrated that food insecurity is associated with increased odds of diabetes,8-10 depression, and anxiety.11-14 In pregnant women, food insecurity has been associated with increased odds of anemia.15,16
Additionally, food insecurity is associated with negative health outcomes in children.7,17,18 Children living in households with food insecurity are three times more likely to report frequent headaches, 19 and 57% more likely to report upper respiratory tract infections. 20 Among infants and toddlers, food insecurity is associated with developmental delays,21,22 and among children ages 6–12 years, food insecurity is associated with psychosocial dysfunction including aggression and anger. 23 Additionally, food insecurity is associated with increased odds of fair and poor self-rated health among children three years or less, asthma among children 10–15 years, and anemia among children 12–15 years.7,24-26
The impact of food insecurity on children’s health may be further demonstrated by observing measurable laboratory values. For example, children and adolescents from food-insecure households have inadequate blood concentrations of serum proteins, vitamin D, folate, and iron, amongst other nutrients.27-29 Also, food insecurity is associated with elevated white blood cell count, reduced hematocrit volume, and iron deficiency anemia.30-33 Hemoglobin, found in hematocrit, is a protein responsible for shuttling oxygen in the blood. Low hemoglobin levels can be an indication of anemia, which has been associated with reduced cognitive function in children. 31
Nutrition assistance programs are safety net, federally funded interventions aimed at providing an adequate food supply to children, adolescents, and adults in qualifying households. 34 These nutrition assistance programs, such as the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and the Supplemental Nutrition Assistance Program (SNAP), provide nutritious foods that aid the physical, social, and cognitive growth of children and adolescents.35,36 These programs have been shown to increase nutrient intake in preschool-aged participants when compared to eligible non-participants. 36 Supplemental Nutrition Assistance Program (formerly referred to as food stamps) is the largest food nutrition program in the US. Although SNAP is administered in all states in the US, eligibility, and duration of access vary by state. 35 Households participating in SNAP have better self-reported health, fewer sick days, and fewer hospital visits.37-40 A longitudinal study that assessed health outcomes of children and households who had SNAP in early life demonstrated a reduced risk of metabolic diseases. 39 While studies have evaluated the health benefits of SNAP and the health challenges of food insecurity, there is very little research that evaluates the role of SNAP participation vs non-participation on anemia among school-aged children and adolescents living in families with food insecurity.
Conceptually, among food-insecure households, children and adolescents receiving nutrition assistance would be expected to have reduced rates of anemia as compared to those without access to nutrition assistance. While food-insecure households may be more intentional in enrolling in SNAP, children and adolescents living in food-insecure households may have anemia prior to enrollment. Limiting the data to children and adolescents living in food-insecure households and measuring the association between SNAP and anemia after enrollment may give insights into the benefits of SNAP participation in this unique population. Also, measuring hemoglobin using quantifiable hematological parameters from the complete blood count (CBC) test will objectively evaluate the association of SNAP participation and anemia. There is no study, to our knowledge, that measures the association of SNAP on the health of school-aged children and adolescents living in food-insecure households using measurable hematological values. This study aims to assess the association of SNAP on the anemia status of children and adolescents living in food-insecure households using population-based data.
Methods
Study Population
This cross-sectional analysis uses 12-year pooled secondary data (2003 to 2014) from the National Health and Nutrition Examination Survey (NHANES). The NHANES is one of the oldest surveys in the US, which combines interviews, physical examination, and laboratory results to provide data on vital health statistics across the US. 41 Data are released every two years. Each two-year cycle, approximately 12 000 to 15 000 non-institutionalized US civilians are screened. Between 9500 and 10 200 of these individuals are subsequently interviewed, and between 9000 and 10 000 individuals are examined in each two-year cycle. 41 The interview and examination response rates ranged from 71 to 82% and 68 to 78%, respectively, across the years. 41 Interview questions directed at children and adolescents were either answered by the selected child or adolescent, or by a member of the household who was able to serve as a knowledgeable proxy. 42 The data obtained from the questionnaire, examination, and laboratory files across the six two-year cycles were merged using unique identifiers. The merged files for each two-year data were appended to produce a single dataset.
One inclusion criterion for our study was food security status. National Health and Nutrition Examination Survey classifies household food security status as full, marginal, low, and very low food security, coded from 1 to 4 respectively. Only respondents with low (coded 3) and very low (coded 4) food security were selected for this study. We limited study participants to those children and adolescents between the ages of 6 and 18 years (n = 3315). Furthermore, we excluded participants who were unsure whether they were SNAP participants (n = 1092) and those who did not have hematocrit values (n = 588). The final sample size (n = 1635) consisted of 996 children living in households participating in SNAP and 639 not participating in SNAP (Figure 1). Data selection steps using pooled data from the National Health and Nutrition Examination Survey (NHANES): 2003–2014.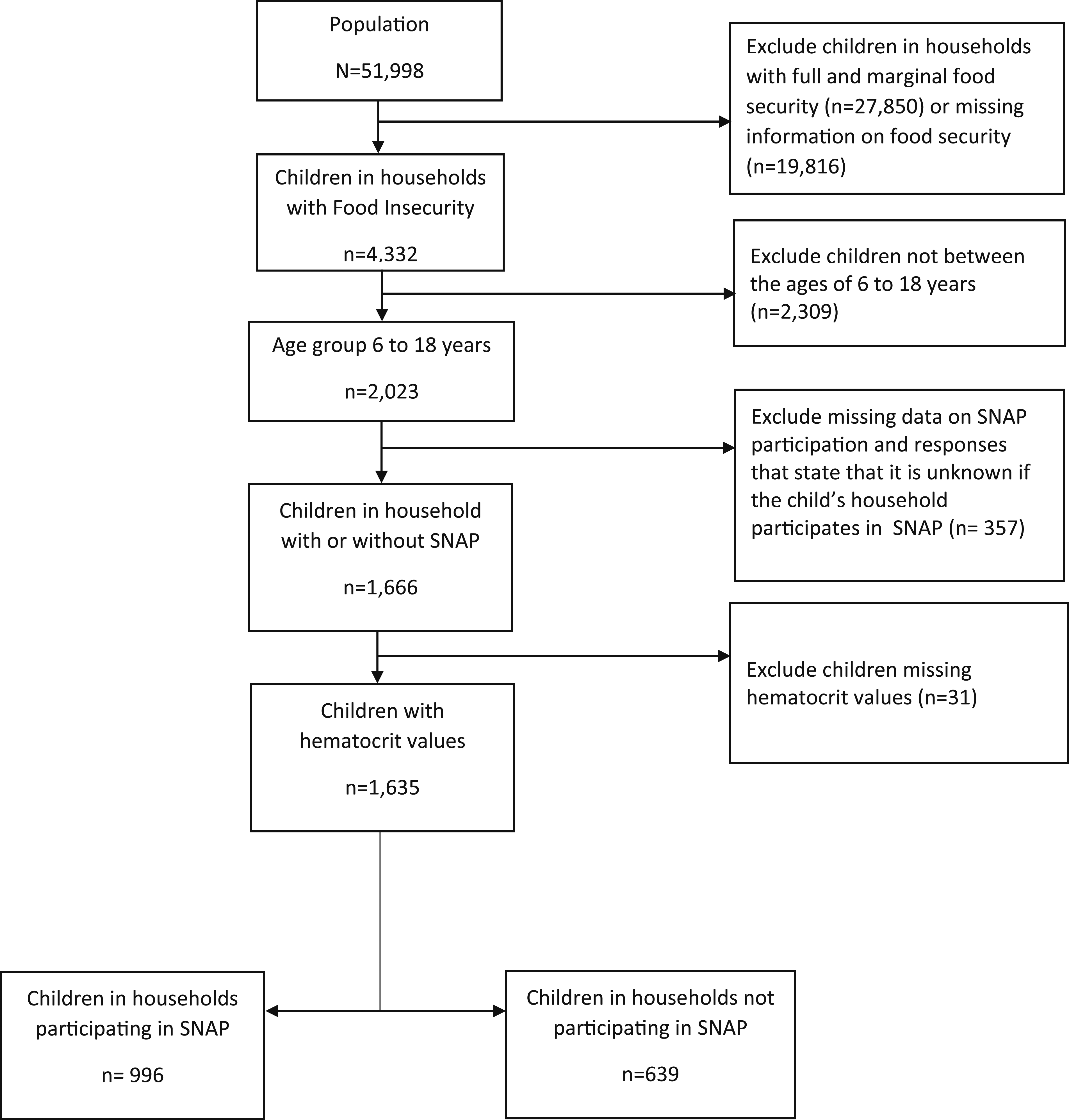
Exposure Variable
The exposure of interest in this study was household SNAP participation. This variable was self-reported, using the question: “In the last 12 months, did you or any member of your household receive SNAP benefits?” Individuals who indicated that they received these benefits were considered to be exposed.
Outcome Variable
The outcome variable was the presence or absence of anemia, classified using the blood hematocrit concentration values. Hematocrit concentration, recorded as a continuous variable, was recoded as a binary variable, using the reference ranges published in the NHANES laboratory manual, accounting for changes across gender and different reference ranges across the years. 43 Anemia was defined as hematocrit values lower than the reference range of hematocrit concentration. 44 Hematocrit values within and above the reference ranges were classified as not anemic.
Confounders
Confounders were selected a priori from published studies related to SNAP and food security.30,40,45-47 We selected demographic characteristics such as age, gender, race/ethnicity, children’s and caregiver’s educational attainment, household poverty-income ratio, as well as the household size, child/adolescent hospitalization within the past year, household WIC participation, and child/adolescent’s self-rated health as potential confounding variables. Child hospitalization and self-rated health assessed the child’s health at the time of survey. 48 Women, Infants, and Children participation served as an indicator of concurrent participation in other food assistance programs while household size served as an indicator of household structure. These potential confounders may be associated with SNAP and anemia, without being in the causal pathway.
Statistical Analysis
All statistical analyses were performed using SAS Software version 9.4. 49 Descriptive statistics were generated for exposure, outcome, and sociodemographic variables. Measures of association among categorized variables were assessed using chi-square analysis, with significance set at a P-value less than .05. Since the data were drawn from a population survey and pooled across 12 years, the final weighted variable was calculated by dividing the sample weight variable by 6, representing the number of data cycles in the pooled sample (two years of data represents one data cycle). 50 Logistic regression analysis using survey commands was used to calculate the odds ratio (ORs) and 95% confidence intervals (CIs).
Results
Frequency distribution of the sociodemographic, food security, and hematologic variables from the National Health and Nutrition Examination Survey (NHANES): 2003–2014.

SNAP: Supplemental Nutrition Assistance Program; WIC: Special Supplemental Nutrition Program for Women, Infants, and Children; χ2 test comparing proportion of anemia. Statistically significant associations (P < .05) are indicated in bold.
Odds ratios and 95% confidence intervals of the associations between select variables and anemia among children residing in food-insecure households; 2003-2014 National Health and Nutrition Examination Survey (NHANES).

CI: Confidence Interval; Ref: Reference Category; SNAP: Supplemental Nutrition Assistance Program; WIC: Special Supplemental Nutrition Program for Women, Infants, and Children.
Statistically significant associations (P < .05) are indicated in bold.
Adjusted odds ratio and 95% confidence interval of the association between SNAP participation and anemia in children and adolescents residing in food-insecure households; 2003–2014 National Health and Nutrition Examination Survey (NHANES).

CI, Confidence Interval; Ref, Reference Category; SNAP, Supplemental Nutrition Assistance Program.
Statistically significant associations (P < .05) are indicated in bold.
a Model adjusted for age, gender, race/ethnicity, children and caregiver’s educational level, poverty-income ratio, household size, self-rated health, history of hospitalization, and household receipt of WIC.
Discussion
In this population-based study, approximately 2% of children and adolescents living in food-insecure households had anemia. Furthermore, children and adolescents who were participants in SNAP had nearly three times the odds of anemia as compared to children and adolescents living in households that were not SNAP participants, and this finding was statistically significant.
The small prevalence of anemia in our study is similar to findings of other studies using a nationally representative sample.51,52 A World Health Organization report estimated that 3.1% of preschool-age children in the United States have anemia. 51 Similarly, a study using 2007–2010 NHANES data found the prevalence of iron deficiency anemia to be 3.9% in preschool-age children across all households, not just those with food insecurity. 52
Very few studies have evaluated the relationship between SNAP and anemia.33,36 A study done in 1998 comparing nutritional intake among preschoolers living in households participating in both SNAP and WIC as compared to non-participant preschoolers, showed that the combined effect of SNAP and WIC was associated with a higher blood volume of iron, which clinically can be conceptualized as reduced anemia. 36 Similarly, Leung and Blumenthal, 53 using pooled data from the 1999–2008 NHANES and a population of children living at or below the poverty line, reported that SNAP was associated with significantly increased serum iron after controlling for sociodemographic factors, participation in other food assistance program and household food security status. Leung and Blumenthal, 53 however, did not report the changes in serum iron by household food security status. While these prior studies acknowledge the benefits of SNAP among all beneficiaries, findings from our study suggest that SNAP benefits may not be sufficient in addressing the health needs of children and adolescents living in food-insecure households.
For this study, our hypothesis was that SNAP participation would be associated with reduced odds of anemia, as SNAP is intended to provide nutritious foods for households with food insecurity. 4 However, our findings showed the opposite—that SNAP participation was associated with increased odds of anemia. Indeed, the far-reaching benefits of SNAP on reduced food insecurity, 45 reduced chronic illness, 47 and increased cognitive function 39 demonstrate its immense positive impact on children’s health indices. However, this study highlights that the benefits of SNAP may be inadequate among the population that needs it the most—food-insecure children and their households.54,55 Earlier studies have reported some of the factors associated with the benefit inadequacies of SNAP such as the geographical variation in food prices,54,56-58 and disparity in food outlets,54,59 and food access.54,60-62
The observed relationship between SNAP and anemia among children and adolescents living in food-insecure households emphasizes the need to assess SNAP’s program structure as well as the individual, household, and environmental factors associated with anemia in food-insecure households. These factors may include, but are not limited to, the measurement of SNAP adequacy,56,63 an assessment of healthy food knowledge, attitudes, and preferences especially in food-insecure households,64,65 an evaluation of effective measures that mitigate food deserts and food swamps (measures of distance to healthy food and availability of unhealthy food choices, respectively).60,61,66,67 Also, there is a need to assess the spatial distribution of anemia among children and adolescents living in food-insecure households as well as evaluate effective measures that may attenuate the rural-urban disparity in food access. 68
This study should be considered in light of its limitations and strengths. First, it is impossible to establish causality from a cross-sectional study. Also, the temporal sequence from SNAP participation to anemia assessment could not be assessed from the NHANES. While SNAP participation preceded anemia assessment, the exact duration varied among participants, and this information was not reported in the NHANES. There is also a possibility of coverage error in sampling individuals with low and very low food insecurity. Individuals with food insecurity are more likely to have associated housing instability, 69 making them less likely to be identified by the NHANES survey design. 70 In addition, there is a potential for selection bias since between 15 and 25% of the children and adolescents who were screened opted not to have laboratory examinations and blood drawn. 50 Nondifferential misclassification of the exposure due to self-report of SNAP participation is possible as individuals may have felt there was a stigma associated with responding affirmatively to this question. Nondifferential misclassification of the outcome, however, is unlikely as anemia was measured by hematological profile according to the participant’s gender. This study is further strengthened by its nationally representative population. The results of this study can likely be generalized to US children aged 6–18 years old who live in households with food insecurity.
With a paucity of data on quantitative health indices of children and adolescents aged 6 to 18 years living in households with low and very low food insecurity, this study represents one of the few studies that elaborate on the burden of anemia among children and adolescents in food-insecure households participating in SNAP in the US.
Conclusions
Among households with low and very low food insecurity, participation in SNAP benefits is associated with childhood and adolescent anemia. This unexpected relationship presents areas for future research. Additional research is needed to assess if these unexpected findings are related to the adequacy of SNAP, affordability, and accessibility to healthy foods, or the household and individual food preferences in food-insecure households.
Footnotes
Authors’ Contributions
The authors’ responsibilities were as follows: OJA, JDS, EGB, NO, and LRH: designed the research plan; OJA, EGB: analyzed the data; OJA, JDS, EGB, NO: wrote the paper; OJA, JDS, and LRH had primary responsibility for the final content; and all authors: read and approved the final article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article