
Abstract
To examine whether rates of 30-day readmission after acute ischemic stroke changed differentially between Medicaid expansion and non-expansion states, and whether race/ethnicity moderated this change, we conducted a difference-in-differences analysis using 6 state inpatient databases (AR, FL, GA, MD, NM, and WA) from the Healthcare Cost and Utilization Project. Analysis included all patients aged 19-64 hospitalized in 2012–2015 with a principal diagnosis of ischemic stroke and a primary payer of Medicaid, self-pay, or no charge, who resided in the state where admitted and were discharged alive (N=28 330). No association was detected between Medicaid expansion and readmission overall, but there was evidence of moderation by race/ethnicity. The predicted probability of all-cause readmission among non-Hispanic White patients rose an estimated 2.6 percentage points (or 39%) in expansion states but not in non-expansion states, whereas it increased by 1.5 percentage points (or 23%) for non-White and Hispanic patients in non-expansion states. Therefore, Medicaid expansion was associated with a rise in readmission probability that was 4.0 percentage points higher for non-Hispanic Whites compared to other racial/ethnic groups, after adjustment for covariates. Similar trends were observed when unplanned and potentially preventable readmissions were isolated. Among low-income stroke survivors, we found evidence that 2 years of Medicaid expansion promoted rehospitalization, but only for White patients. Future studies should verify these findings over a longer follow-up period.
Medicaid expansion has well documented effects on health care utilization, and there is mixed evidence about its impact on racial health disparities in the United States, but no published studies have examined its association with post-stroke readmissions, and none has examined racial and ethnic differences in readmission trends related to Medicaid expansion.
Our research suggests that Medicaid expansion has no aggregate effect on 30-day readmission after ischemic stroke during the first 2 years of implementation, but it shows racial/ethnic differences in the response of readmission rates to the expansion of Medicaid: non-Hispanic White patients had increased utilization of inpatient care associated with Medicaid expansion relative to other groups.
Although confirmation in a sample with a longer follow-up period is needed, expectations about post-stroke readmissions should be managed in the 12 states that have not expanded Medicaid under the Affordable Care Act, and attention to racial/ethnic equity in readmission is warranted in the states that did expand Medicaid.What do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications Towards Theory, Practice, or Policy?
Introduction
Stroke persists as a leading cause of death and disability in the United States and places a substantial burden on the health system. 1 Moreover, 12% to 21% of stroke survivors will be re-hospitalized within 30 days.2,3 About one-fifth of readmissions after ischemic stroke are due to recurrent stroke, and many others are attributable to underlying comorbidities—for example, dysrhythmias, heart failure, and diabetes—or complications such as pneumonia, seizures, and falls.2,4 Comorbidities can be managed and complications prevented with high-quality post-stroke care, including office visits, outpatient medications, and rehabilitation. Health insurance enables access to stroke-related care: having insurance has been associated with improved access to preventive medications, emergency services, and inpatient rehabilitation for acute ischemic stroke, and with lower risk of stroke-related death. 5 However, the specific effect of insurance on readmission after stroke is undetermined.
The Patient Protection and Affordable Care Act (ACA) of 2010 expanded health coverage to millions of Americans through several mechanisms, including changes to Medicaid eligibility. 6 The ACA was meant to expand Medicaid eligibility—at an enhanced federal matching rate—to everyone with a household income below 138% of the federal poverty level (FPL). However, a Supreme Court ruling in 2012 allowed individual states to opt out of Medicaid expansion. 7 As a result, millions of adults remain uninsured in the 12 states where Medicaid has not been expanded under the ACA, because they are too low-income to qualify for Marketplace subsidies yet do not meet the limited criteria (e.g., pregnant, disabled, or elderly) for the original Medicaid programs in their states.
In a systematic review of 62 observational studies, Medicaid expansion was associated with increased access to and quality of care. 8 For example, states that expanded Medicaid have seen increased reports of having a usual source of care or a personal physician,9–11 decreased non-emergent use of the emergency department, 12 and improved appointment availability.9,13 In addition, expansion states have seen increased primary care and preventive health visits,14,15 greater uptake of mental health services, 14 higher proportions of chronic disease patients receiving regular care,12,16 shorter hospital stays,17,18 and declines in reports of psychological distress and poor mental health.10,19 Finally, some health care quality indicators have improved more in expansion states, including glycemic monitoring for diabetes, 12 guidelines-based prescribing for asthma, 20 post-operative morbidity rates, 21 and blood pressure control. 20
However, the effect of Medicaid expansion on ischemic stroke outcomes remains largely unexamined. Prior research with Get With The Guidelines® (GWTG) registry data reported the effects of health insurance on in-hospital mortality and access to prehospital and rehabilitation services in ischemic stroke, but not the specific impact of Medicaid expansion on post-stroke readmissions. 5 A prior study with National Health Interview Survey data showed that self-reported inability to afford medications among stroke survivors aged 45-64 decreased after ACA implementation, 22 and another study of community health centers showed a positive association between Medicaid expansion and hypertension control. 20 One recent study, again using GWTG data, observed an association between Medicaid expansion and odds of discharge to a skilled nursing facility after acute ischemic stroke. 39 However, there is need to understand whether expanded Medicaid also affects readmissions after stroke, to the extent that better access to outpatient care has an impact on readmission rates.
Most of the states with an ongoing coverage gap related to non-expansion of Medicaid are located in the “Stroke Belt” (see Figure, Supplemental Digital Content 1, for side-by-side maps of stroke mortality and Medicaid expansion). Moreover, this coverage gap primarily affects adults under age 65, and stroke incidence has been shifting to non-elderly adults since the 1990s. 23 It is important, therefore, to understand the consequences of state Medicaid expansion decisions for stroke outcomes in this age group. The stroke burden on younger adults is especially pronounced for Black Americans, 23 and Medicaid expansion has been associated with improved racial equity in health insurance coverage and preventive care use. 24 Yet, research also suggests that non-financial, structural barriers to accessing care (e.g., mistrust, language barriers, discrimination, geography, availability of primary care providers, lack of minority workforce, and patient activation) may impede some of the benefits of Medicaid expansion for racial and ethnic minorities.25,26 Therefore, it is necessary to consider whether the impact of expansion on stroke outcomes differs by race and ethnicity. The objectives of this study, then, were (1) to determine the association between Medicaid expansion and the probability of 30-day hospital readmission following acute ischemic stroke, and (2) to evaluate whether race/ethnicity moderated the association between expansion and readmission.
Conceptual Framework
This study was motivated by an ambiguous relationship between health insurance coverage and hospital readmission in the context of ischemic stroke. In other health conditions with a chronic cardiovascular pathology, excess readmissions within 30 days of discharge are considered suboptimal, because they may reflect poor discharge planning or care coordination. 27 Financial incentives to reduce 30-day readmissions after hospitalization for myocardial infarction, chronic obstructive pulmonary disease, and heart failure were codified in the ACA’s Hospital Readmissions Reduction Program. 28 Readmissions can also be a product of poor access to follow-up outpatient care, such as prescription medications and appointments with specialists, regardless of care coordination efforts. Therefore, expanded health insurance may be expected to reduce readmissions for ischemic stroke survivors by promoting clinical disease management in outpatient settings.
Unlike other conditions, however, ischemic stroke frequently warrants return visits to the hospital for scheduled procedures to prevent stroke recurrence (i.e., secondary prevention). Stroke is also linked to multiple neurologic deficits that may lead to complications requiring inpatient care, such as aspiration pneumonia, seizures, and fall-related fractures. 4 In addition, the Oregon Health Insurance Experiment found that Medicaid expansion (through a lottery system) was associated with increases in both using outpatient care and being hospitalized. 29 To the extent that health insurance promotes timely inpatient care for complications or secondary prevention, Medicaid expansion may also work to raise the probability of readmission for low-income stroke survivors. Empirical research is needed to understand which direction dominates in the associations between Medicaid expansion and post-stroke readmission.
Our study examined the associations of Medicaid expansion with unplanned and potentially preventable readmissions in addition to all-cause readmission. “Unplanned readmission” after ischemic stroke excludes rehospitalization for procedures typically scheduled soon after discharge to prevent stroke recurrence (or as a follow-up to surgery that was performed emergently, such as cranioplasty after emergency craniectomy).2,4 Although health insurance likely increases demand for planned readmissions, the impact on unplanned readmissions after stroke is uncertain. “Potentially preventable readmission” is defined as hospitalization for a condition that is usually amenable to ambulatory care. 30 Health insurance may be expected to reduce such readmissions by facilitating access to ambulatory care, but only if timely outpatient appointments are available, which may not be the case when practices do not accept new Medicaid patients or lack appointment availability within 30 days.
Additionally, hospitalization patterns in the U.S. vary by racial/ethnic identity. A review of over 60 studies covering the period 1998-2016 found evidence that racial and ethnic differences in hospitalization for chronic, ambulatory-care-sensitive conditions have increased, resulting in over 430 000 excess admissions among Black individuals compared to non-Hispanic Whites. 31 Multiple studies have shown that racial health disparities are not fully attributable to socioeconomic indicators.32–34 On the other hand, uninsured Blacks, Hispanics, and other patients of color had lower odds of all-cause readmission than uninsured White patients in inpatient data from five states, and readmission odds were comparable between Black and White Medicaid members. 27 Regardless of whether Medicaid expansion lowers or raises the chance of readmission after stroke, then, it is important to evaluate whether the effects of expansion on post-stroke readmission vary by race/ethnicity.
Methods
This study had a retrospective, quasi-experimental design using 6 State Inpatient Databases (SID) from the Healthcare Cost and Utilization Project (H-CUP) at the U.S. Agency for Healthcare Research and Quality (AHRQ). The SID are produced under data-sharing agreements with partners in 30 states, typically state health departments or hospital associations. 35 The databases contain deidentified discharge records from the vast majority (≥97% during the study period) of short-term, nonfederal, non-rehabilitation hospitals. 36 For this project, 4 years of data (2012-2015) were available.
Sample
The sample comprised all patients hospitalized in 2012-2015 with a principal diagnosis of ischemic stroke aged 19-64 at the time of the index hospitalization, who resided in the state where admitted; had an expected primary payer of Medicaid, self-pay, or no charge (mostly charity care); and were discharged alive. Ischemic stroke was identified with International Classification of Diseases-Ninth Revision-Clinical Modification (ICD-9-CM) codes 433.x1, 434.x1, and 436 or, in the fourth quarter of 2015, with ICD-10 codes I63.xx and I67.89. 2 Hospitalizations for hemorrhagic stroke or transient ischemic attack were disregarded due to important differences from ischemic stroke in prognosis. The restriction to ages 19-64 was necessary, because most U.S. residents outside this range have access to public health insurance programs in every state. In-state residence was required to ensure that patients had been exposed to that state’s Medicaid expansion policy prior to the index stroke.
The specification of primary payer as Medicaid, self-pay, or no charge was a proxy for low-income status, because there is no individual-level income variable in the SID. (Self-pay and charity care patients are typically uninsured.) This approach has been taken in other Medicaid expansion studies where income and poverty data were unavailable.37–39 The SID contain a variable for median household income quartile of the patient’s ZIP code, but this was not used due to lack of precision and the potential for ecological fallacy when ZIP codes are economically heterogenous. Nonetheless, we conducted a sensitivity analysis using the lowest quartile of median household income in the ZIP code to identify low-income patients instead of using primary payer. Finally, patients who died during their index hospitalization were excluded, because they had no probability of readmission.
Measures
States were divided into expansion (AR, MD, NM, and WA) and non-expansion (FL and GA) categories. 40 These 6 states were selected from the 12 SID that contain patient linkage variables to identify readmissions, because they had appreciable minority population sizes and no large-scale public health insurance expansions for low-income adults prior to the ACA. The pre-expansion period was 2012-2013; post-expansion was 2014-2015. Any in-state hospitalization within 30 days of discharge (except for rehabilitation, psychiatry, or cancer treatment) was considered a readmission, consistent with the Centers for Medicare and Medicaid Services specification of all-cause readmission. 41 For duplicate hospitalizations (mainly same-day admissions and transfers), the record with a transfer-out indicator or a length of stay of 0-1 days was discarded. Five additional duplicate pairs were adjudicated on a case-by-case basis.
A secondary analysis was conducted on just the unplanned and potentially preventable readmissions. Consistent with prior studies, a readmission was considered unplanned if it did not contain a principal procedure code for 1 of the following: carotid endarterectomy, percutaneous carotid or other precerebral artery stenting, patent foramen ovale closure, atrial fibrillation ablation, aortic or mitral valve replacement, or cranioplasty.2,4 Using the AHRQ Prevention Quality Indicators relevant to adults, a readmission was considered potentially preventable if the principal diagnosis code was one of the following: chronic obstructive pulmonary disease, asthma, diabetes (uncontrolled or with short- or long-term complications), hypertension, heart failure, bacterial pneumonia, or urinary tract infection. 30 Readmissions before and after Medicaid expansion were compared using z tests of the difference in proportions for expansion and non-expansion states.
The racial group and Hispanic ethnicity variables were combined and dichotomized into non-Hispanic White vs all other groups (see detailed explanation under Analysis Plan below). Age was measured in years and treated as a continuous variable, sex was treated as binary, and urban influence codes were dichotomized into living in a metropolitan area or not.
Analysis Plan
The analytic approach was a difference-in-differences (DD) framework, a robust method for causal inference in policy evaluations. 42 Logistic regression with random effects for clustering by hospital and an interaction of “treatment” (state expansion decision) and time (pre or post expansion) was performed to estimate the effect of Medicaid expansion on readmission, adjusted for age, sex, number of diagnoses, and metropolitan residence. 43 Predicted probabilities of readmission were computed from the estimated regression parameters (holding covariates at their mean values), the change in readmission probability was estimated for expansion and non-expansion states using average marginal effects, and the difference in the change in probability between the 2 groups—the net effect of Medicaid expansion—was estimated with a planned contrast of marginal effects.
Next, a three-way interaction of time-by-treatment-by-race (i.e., a difference-in-differences-in-differences, or DDD, estimator) was added to the models to test whether race/ethnicity moderated any association between expansion and readmission, because testing for a subgroup-treatment interaction is a more appropriate statistical approach to subgroup analysis than stratifying the sample. 44 To maximize the interpretability of the three-way interaction models, we limited the number of subgroups to 2, which required dichotomizing race/ethnicity. We categorized race/ethnicity into non-Hispanic White vs all other groups (referred to as “White” and “non-White” in the results for short), because of evidence in our DD analysis that readmission was strongly associated with classification as White, and because prior studies of Medicaid expansion and of readmission reported differences in outcomes between White patients and other groups.27,45 Furthermore, among ischemic stroke patients, Whites have a higher prevalence of carotid artery stenosis compared to other groups and therefore may be expected to have higher incidence of planned endarterectomy. 46 Excluding endarterectomies from our secondary analysis of unplanned readmissions allowed us to evaluate any residual difference in readmissions between White patients and patients of color.
To estimate the differential effect of Medicaid expansion by race/ethnicity, predicted probabilities were again computed from the estimated model, holding covariates at their means. The predicted change in readmission probability was estimated with average marginal effects for each subgroup: Whites and non-Whites in expansion states, and Whites and non-Whites in non-expansion states. Finally, a planned contrast of marginal effects was run to estimate the net effect of expansion and race/ethnicity on readmission probability. To test the identifying assumption of the DD framework, we compared pre-expansion trends between expansion and non-expansion states. Specifically, we plotted the 3 readmission outcomes by discharge quarter to inspect for parallel trends, and we carried out an event study that interacted a 2012 indicator with expansion decision (using 2013 as the reference value) to check for evidence of Medicaid expansion effects before expansion happened.
Three additional types of robustness checks were conducted to assess whether results were sensitive to model specifications. First, readmissions to hospitals flagged as long-term acute care (LTAC) or rehabilitation facilities were excluded. (This identifier was available only for AR, FL, MD, and WA and comprised just .37% of readmissions in those states.) Then, readmissions for acute cerebrovascular disease—AHRQ Clinical Classification Software code 109—were added to the analysis of unplanned readmissions, regardless of procedure code, in case some of these procedures were for recurrent stroke instead of secondary prevention. 4 (This increased unplanned readmissions by 1.2%.) Finally, fixed-effects terms for state and year of observation were added to the regression models. This research was considered exempt by the first author’s institutional review board and complied with a data use agreement with AHRQ. All analyses were conducted in Stata version 16 (StataCorp LLC, College Station, TX). The data sets and related software tools may be acquired from H-CUP at https://www.hcup-us.ahrq.gov/.
Results
Sample Characteristics
Sample characteristics.

*Mostly charity care.
SD, standard deviation.
Readmission Before and After Expansion
Figure 1 displays the readmission rates in the pre-expansion and post-expansion periods. In expansion states, the percent of patients readmitted within 30 days for all causes increased by 1.16 percentage points (z = 2.02, P = .04) from 6.99% to 8.15%, whereas in non-expansion states, all-cause readmission increased by .72 points (z = 2.02, P = .04) from 7.16% to 7.88%. A similar pattern was observed for unplanned readmissions, which increased by .91 percentage points in expansion states (z = 1.63, P = .10), compared to .74 points in non-expansion states (z = 2.14, P = .03). Potentially preventable readmissions remained essentially flat during the study period, increasing by .02 percentage points in expansion states (z = .14, P = .89), and by .01 percentage points in non-expansion states (z = .09, P = .92). (See Table, Supplemental Digital Content 2, for all readmission rates.) A All-cause readmissions over time by state Medicaid expansion status. Note: Excludes rehabilitation, psychiatric, and cancer treatment. B Unplanned readmissions over time by state Medicaid expansion status. Note: Excludes readmissions for procedures commonly used for secondary stroke prevention (e.g., endarterectomy). C Potentially preventable readmissions over time by state Medicaid expansion status. Note: A readmission is considered potentially preventable if the principal diagnosis code is an ambulatory-care-sensitive condition.
Difference-In-Differences Analysis
Logistic regression results (difference-in-differences analysis).

**P <.05.
Note: Standard errors in parentheses. Control variables included dummies for White race, female sex, and metropolitan area residence; number of diagnoses; and age in years.
Marginal predicted means (difference-in-differences analysis).

**P <.05.
Note: Standard errors in parentheses. Adjusted for White race, female sex, metropolitan area residence, number of diagnoses, and age in years.
Moderation by Race/Ethnicity
Logistic regression results with moderation by race/ethnicity (difference-in-differences-in-differences analysis).
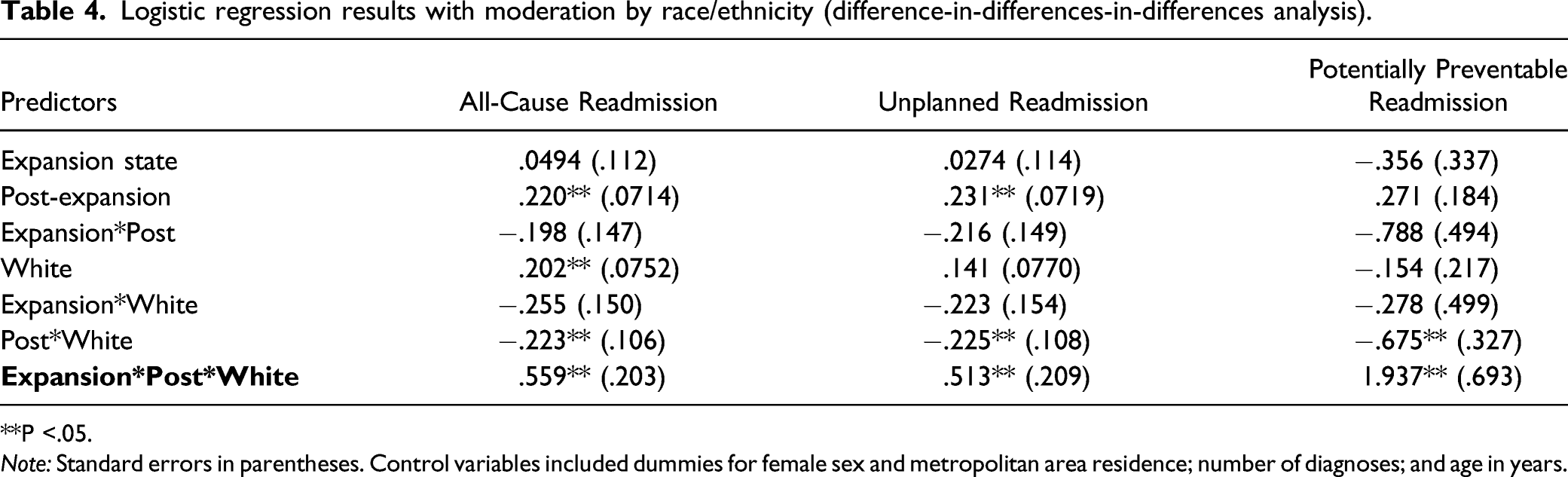
**P <.05.
Note: Standard errors in parentheses. Control variables included dummies for female sex and metropolitan area residence; number of diagnoses; and age in years.
Marginal predicted means by race/ethnicity (difference-in-differences-in-differences analysis).

**P <.05.
Note: Standard errors in parentheses. Adjusted for female sex, metropolitan area residence, number of diagnoses, and age in years.
Similar patterns were observed for unplanned and potentially preventable readmissions. The predicted probability of unplanned readmission rose by 2.06 percentage points, 95% CI [.44, 3.67], for Whites in expansion states and by 1.59 points [.61, 2.57] for non-Whites in non-expansion states. The estimated increases in unplanned readmission were statistically non-significant for non-Whites in expansion states, .09 [–1.55, 1.74], and for Whites in non-expansion states, .04 points [–1.08, 1.17]. The net difference between Whites and non-Whites was 3.51 percentage points [.77, 6.26]. For potentially preventable readmissions, predicted probability increased an estimated .49 percentage points [–.02, .99] for Whites and decreased .27 [–.76, .21] for non-Whites in expansion states. In non-expansion states, predicted probability decreased .27 points [–.63, .08] for Whites and increased .30 [–.10, .70] for non-Whites. Although these estimates were not statistically significant, the net difference between Whites and non-Whites was significant at 1.33 percentage points [.45, 2.22].
Robustness Checks
Trend lines before and after expansion for all outcome variables are displayed in Figures 1 and 2. (Data from the fourth quarter of each year were omitted when fitting the trend lines because of the decreased chance of observing a 30-day readmission for discharges in December.) On inspection, the baseline trends for unplanned readmission appeared non-parallel between expansion and non-expansion states; however, they were notably more parallel when disaggregated by race/ethnicity. The event studies showed no evidence of a statistically significant interaction between 2012 (vs. 2013) and expansion status in 5 of the 6 models. The event study for the sixth model (of potentially preventable readmission and moderation by race/ethnicity) was not estimable due to sparseness of data in 1 of the cells. A All-cause readmissions over time by state Medicaid expansion status and patient race/ethnicity. Note: Excludes rehabilitation, psychiatric, and cancer treatment. B Unplanned readmissions over time by state Medicaid expansion status and patient race/ethnicity. Note: Excludes readmissions for procedures commonly used for secondary stroke prevention (e.g., endarterectomy). C Potentially preventable readmissions over time by state Medicaid expansion status and patient race/ethnicity. Note: A readmission is considered potentially preventable if the principal diagnosis code is an ambulatory-care-sensitive condition.
The results of the analyses were stable after adding state and year fixed effects to the models, and after excluding readmissions to rehabilitation and LTAC hospitals in the 4 states where possible (data not shown). The models of unplanned readmission were robust to the reclassification of all readmissions for acute cerebrovascular disease as unplanned. Finally, the sensitivity analysis using the lowest median household income quartile (instead of primary payer of Medicaid, self-pay, or no charge) showed the same pattern of non-significant results for the DD estimates. For moderation by race/ethnicity, none of the DDD estimates were statistically significant in the sensitivity analysis, though the effect estimates were similar in magnitude and direction for all-cause readmission, at 2.33 percentage points [–.76, 5.42], and unplanned readmission, at 1.98 percentage points [–1.03, 4.99].
Discussion
Overall, this study observed no statistically significant association between Medicaid expansion and 30-day readmission post ischemic stroke after 2 years of implementation. However, this study did observe a significant difference in the association between Medicaid expansion and readmission by race/ethnicity. Specifically, the predicted probability of all-cause readmission among non-Hispanic White patients rose an estimated 2.63 percentage points (or 39%) in expansion states but not at all in non-expansion states. This finding was reversed for non-White and Hispanic patients, whose readmission probability increased in non-expansion states (by 1.53 percentage points, or 23%), but not in expansion states. Medicaid expansion, therefore, was associated with a 4.04 percentage point rise in readmission likelihood for Whites relative to non-Whites, after adjustment for covariates. This pattern of results held when only unplanned and potentially preventable readmissions were examined.
In other words, the difference in readmission probability widened between non-Hispanic White patients and all others after expansion in expansion states, whereas it narrowed in non-expansion states (Figure 3). One driver of the rise in readmissions in expansion states among White patients could be an uptick in planned readmissions: hospital visits for procedures such as endarterectomy that are typically performed for secondary stroke prevention. It is possible that Medicaid expansion facilitated access to timely procedures for secondary prevention more for White patients than for patients of color. This finding is consistent with a study of Behavioral Risk Factor Surveillance System data from 2011-2016, which found that Medicaid expansion had favorable impacts on access to care and health outcomes among Whites, but relatively few such impacts among Blacks and Hispanics.
45
In addition, carotid artery stenosis is more prevalent among Whites.
46
Therefore, Black, Hispanic, and Asian/Pacific Islander patients may have experienced more intracranial strokes, which are less amenable to follow-up surgical procedures. Adjusted predictions from moderation analysis. Note: Predictions are from a logistic regression model of readmission within 30 days for any cause (except rehabilitation, psychiatric, or cancer treatment) with a random effect for hospital intercepts. All covariates (sex, age, urbanicity, and number of diagnoses) are held at their mean values.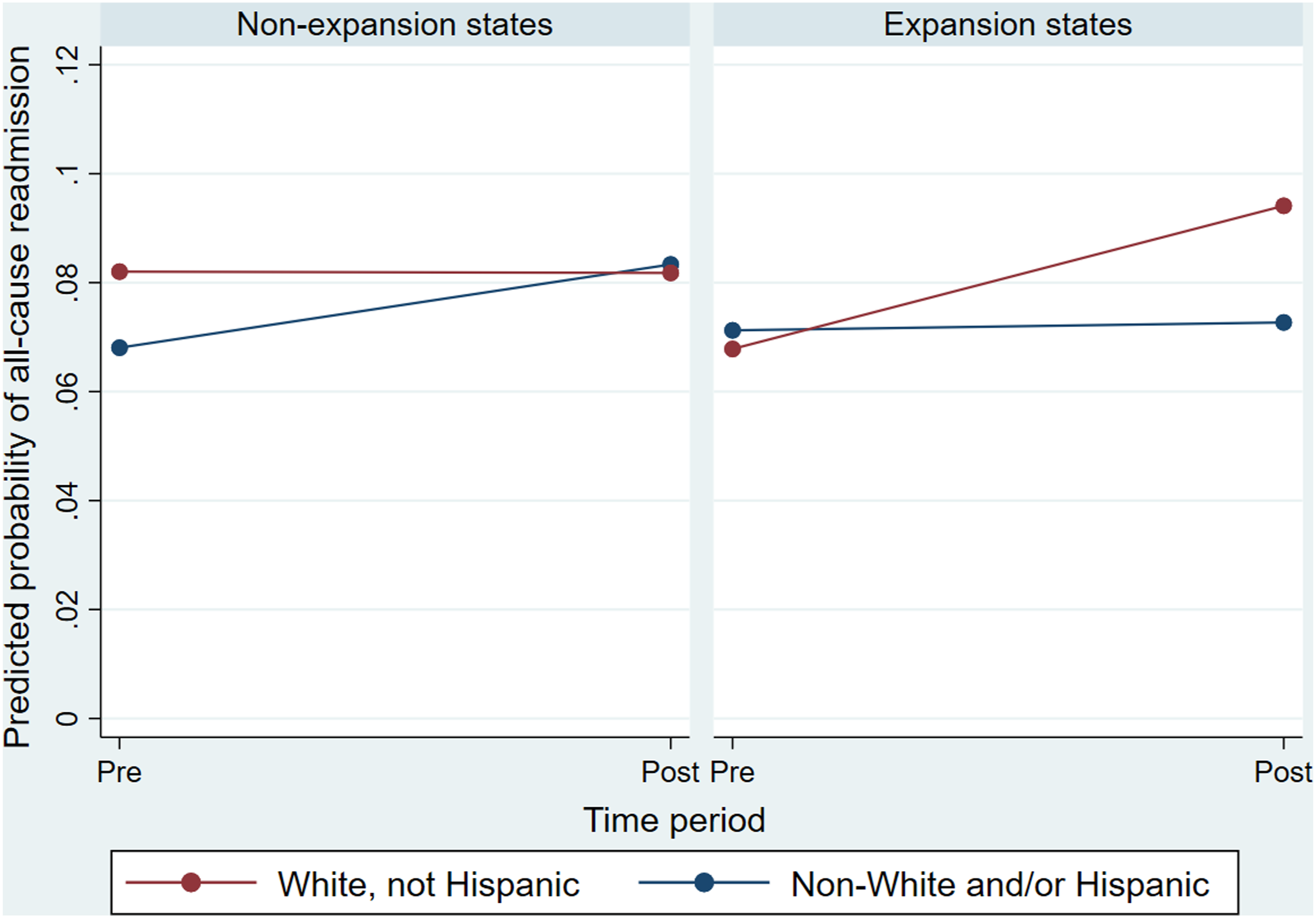
However, the discrepancy in planned procedures does not account for the entire interaction between Medicaid expansion and race/ethnicity, because the three-way interaction was also significant in the model of unplanned readmissions. This could be due to misclassification: planned readmissions were defined by a single procedure code in the discharge record—based on prior literature2,4 and expert consultation—irrespective of other clinical data. At least some readmissions for these procedures may be due to recurrent stroke, though retaining these procedures as unplanned if the readmission diagnosis was acute cerebrovascular disease did not alter the results. Alternatively, the rise in readmissions in expansion states may reflect better access to medically necessary acute care, at least for White patients. In the year prior to the start of public reporting on hospital readmissions, a study of discharge data from five US states found that having no insurance was associated with lower odds of 30-day readmission across three minority groups (Black, Hispanic, and other), but not among Whites. 27 The authors concluded that readmission rates may reflect needed care, not just suboptimal outcomes. 27
There is evidence that White patients have more trust in the health care system and their physicians due to the absence of perceived prior discrimination.47,48 If so, then non-White and Hispanic patients in this study may have delayed or deferred hospital care that Medicaid expansion otherwise would have enabled. In addition, these findings raise the possibility that providers recommend hospitalization more often when the patient is White and non-Hispanic, which could reflect a more aggressive approach to managing White stroke survivors. It is also possible that White patients experienced more complications and required more acute care—the smaller but still significant effect of Medicaid expansion on potentially preventable readmissions among Whites corroborates this interpretation. However, more frequent readmission for ambulatory-care-sensitive conditions could still reflect higher levels of trust in the system or more aggressive management by providers.
This study has several limitations. First, the data set contained only 2 years of follow-up data after implementation of Medicaid expansion. It could take more time for the full effects of this policy change to become apparent. Second, the low-income cohort for this analysis was specified using primary payer, because income data were unavailable. It is likely that the sample did not include all stroke survivors who earned below the income threshold to qualify for expanded Medicaid—and it may have included some patients who earned more. Likewise, some uninsured patients at baseline likely gained access to subsidized private coverage through the ACA exchanges, not through Medicaid expansion, but the eligibility threshold for subsidies (100% FPL) was uniform across states, so the difference in differences in readmissions between expansion and non-expansion states is not likely attributable to other elements of the ACA. Third, the data set did not include specific dates of service, so it was impossible to exclude index discharges in December or to perform a time series analysis. Finally, although DD analysis is a robust approach to causal inference in policy evaluations, this study was still observational; unmeasured confounding variables could have influenced the results.
Conclusions
This study found no overall association between Medicaid expansion and the probability of 30-day readmission after ischemic stroke in four diverse states after two years. However, expansion was associated with racial/ethnic differences in readmission changes: non-Hispanic White patients experienced a notable rise in the likelihood of readmission in states where Medicaid expanded relative to non-White and Hispanic patients. These findings were robust to variations in model specifications, and the same pattern was observed when unplanned and potentially preventable readmissions were isolated. In the 12 states that still have not expanded Medicaid under the ACA, expectations about the impact of expansion on post-stroke readmissions should be managed, and attention to racial/ethnic equity in readmission is warranted. Future studies should verify these findings using a longer follow-up period.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580211062438 – Supplemental Material for Medicaid Expansion and Racial/Ethnic Differences in Readmission After Acute Ischemic Stroke
Supplemental Material, sj-pdf-1-inq-10.1177_00469580211062438 for Medicaid Expansion and Racial/Ethnic Differences in Readmission After Acute Ischemic Stroke by Blake McGee, Seiyoun Kim, Dawn Aycock, Matthew Hayat, Karen Seagraves and William Custer in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580211062438 – Supplemental Material for Medicaid Expansion and Racial/Ethnic Differences in Readmission After Acute Ischemic Stroke
Supplemental Material, sj-pdf-2-inq-10.1177_00469580211062438 for Medicaid Expansion and Racial/Ethnic Differences in Readmission After Acute Ischemic Stroke by Blake McGee, Seiyoun Kim, Dawn Aycock, Matthew Hayat, Karen Seagraves and William Custer in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
Nilay Shah, MD, of Northwestern University, and Jim Marton, PhD, Melissa Osborne, PhD, and Jessica Smith, PhD, of Georgia State University provided valuable consultation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by a grant from the American Nurses Foundation through the Anne Zimmerman Research Endowment Fund. Additional funds were provided by the Byrdine F. Lewis College of Nursing and Health Professions Foundation and the Institute of Health Administration at the J. Mack Robinson College of Business at Georgia State University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.