
Abstract
Background
The surgical environment has multiple factors that could affect nurses’ health. The aim was to determine the effects of the working environment of operating room nurses on their health compared to hospitalization nurses.
Methods
A sample of operating room nurses and hospitalization nurses were included in the study and participated by filling in a self-report survey containing sociodemographic data items, the validated Nordic and SF12 scales and a list of medical conditions.
Results
Three hundred and thirty-one nurses participated in the study. Statistically significant results had obtained for diagnoses of musculoskeletal disorders and contact dermatitis among the operating room nurses.
Conclusion/Application to Practice
Continuous training in ergonomics is essential. Moreover, surgical protocols for preventing infection should be revised, optimizing the chlorhexidine content of soaps to reduce the risk of lesions among the surgical staff.
Keywords
There is no previous research comparing the health of surgical nurses to inpatient nurses by assessing risks in the workplace.
Surgical nurses and hospital ward nurses face various health risks in their workplace due to exposure to biological agents, chemical agents (disinfectants and inhalation anaesthetic agents), radiation and physical burden due to patients or instruments’ handling surgical. In developed countries, there is specific legislation that regulates safety in the workplace. However, such legislation is not enough to prevent risks and secondary diseases suffered by professionals.
Knowledge about occupational risks and improvement actions allow minimizing the harm suffered by nurses.
Background
The work environment in which nurses carry out their daily work face situations and substances that can harm health. It is conditioned by the continuity of shifts for 24 hours, the occupational risks present in the different healthcare areas and the predominant female gender characteristic of this profession.
In working life, acute and chronic pathologies appear among the nursing community and are related to working conditions and their environment.
Many nurses wonder if working in this profession is harmful to their health.
The health and working conditions of the nursing staff (instability, job insecurity, excessive workload and reduced salaries) and the low participation in decision-making that affect workplaces constitute important psychosocial risk factors. This situation has been progressively deteriorating throughout the world. It has been reflected in the decrease in university demand and the desertion of the profession.
The Health and Safety Manual of the National Institute of Healthcare Management (Instituto Nacional de Gestión Sanitaria) classifies risks associated with the workplace as follows 1 : Exposure to biological agents: Pyrolysis of tissues produces ultrafine particles, volatile chemicals and biological compounds some of which are teratogenic or carcinogenic. Surgical plume irritates the respiratory tract and the eyes.2,3 Exposure to chemical pollutants: Disinfectants 4 and inhalational anaesthetic agents: Several studies have shown that chronic exposure to these substances can cause hepatic and kidney alterations in surgical staff. 5 Contact dermatitis and latex allergy: Surgery staff are healthcare workers with the highest prevalence of latex allergy.6,7 Women present more symptomatology than men, as with other atopic disorders.8-10 Repeated use of gloves to perform tasks together with frequent use of soaps and liquid disinfectants and insufficient drying of the hands favours the appearance of symptoms compatible with contact dermatitis. 11 Radiation exposure: Studies have shown increased papillary thyroid cancer incidence due to medical radiation. 12 Load bearing caused by handling objects/patients: Risk factors for suffering back problems include standing still for long periods, lifting heavy objects and patient mobilization.13,14 Work-related stress: Prolonged stress can harm health and can trigger diseases. 15 Studies warned that burnout could lead to serious health problems and reported increases among healthcare staff. 16 Some authors consider that around 25% of nurses suffer from burnout. 17 This syndrome can trigger the onset of severe depression, alcohol and abuse of mood-altering substances, hypertension and chronic disorders. 16
According to Peipins et al., 17 suicide was among the five most common causes of death among nurses, and that they also had higher rates of suicide than the general population.
Long rotating work shifts in addition to excess workloads cause stress and contribute to low job satisfaction and exhaustion, leading to other health problems such as obesity, cardiovascular diseases and type II diabetes. 18
The authors of this work intended to analyse different reasons for a high percentage of work absenteeism. The suspicion that these absences were related to the hostile environment nurses were subjected to would not be surprising.
Methods
Aims
The main objective of this study was to determine the effects of the working environment of operating room nurses on their health compared to hospitalization nurses. The secondary objectives were (1) to know the existing pathologies among nurses depending on their work area and seniority in the workplace; (2) to establish how nurses perceive musculoskeletal disorders and (3) to compare nurses’ perceived health with that of the general population.
Study Design
It was a multicenter cross-sectional observational study carried out in four Spanish hospitals (one hospital with more than 500 beds, one hospital with between 200 and 500 beds, one hospital with less than 200 beds and one hospital with less than 100 beds).
Study Population
The study population were composed of 331 operating room nurses and ward nurses working from four Spanish hospitals between December 2018 and February 2019. All participants were volunteers. They had recruited in the initial introductory study meeting between January 2019 and September 2020.
The inclusion criteria were (1) operating room nurses who worked as scrub nurses, circulating nurses or anaesthesia nurses and (2) hospitalization nurses.
The exclusion criteria were (1) careers without the professional status of nursing staff; (2) working for less than one year and (3) scrub nurses working sporadically in the centre.
Data Collection
All nurses who met the inclusion criteria were consecutively in the study as they answered the questionnaire between December 2018 and February 2019. Nurses were grouped into two groups according to the professional group who worked their role: Surgical nurses or hospitalization nurses.
The number of cases included in the present study was 314, distributed evenly between the two participating groups (157 in each group).To justify this number, we started from variability of 30% (CV) from the publication of Vilagut et al. (2008). The difference to be detected between both groups was set at 5 points, which would be an approximate effect of 10%; losses were not more significant than 10%. Finally, we estimated the 5% for the alpha error probability and a beta error of 20% (minimum power of 80).
Study Variables
The research team members delivered the surveys by hand after presenting the study to the participants and collecting the informed consent document in their respective hospitals. Those who agreed to participate signed a consent document, and once the questionnaires had been answered, they were returned to the researchers by hand. In the four hospitals, the entire staff of permanent surgical nurses participated in the study voluntarily. However, the group of hospitalization nurses was assumed consecutively until the calculated n was achieved. The survey consisted of questions with multiple-choice answers to determine the perceived health and know the nurses’ pathologies.
The primary outcome variables of the study determined the effects of the working environment of operating room nurses on their health compared to ward nurses, which was determined with the health perception of each of them.
The research team provided all nurses with an anonymous questionnaire to be completed in writing. It consisted of 28 closed questions with multiple-choice answers to assess perceived health and musculoskeletal symptoms and describe their diagnosed pathologies.
The questionnaire’s questions on perceived health were constructed from the Modified Scale SF12.20 This Scale is a reduced version of the SF36 Scale, used throughout the world since the 1990s to measure the health status, which in the present study was called perceived health, of the general population. 21 Question 2 of the SF36 was added to the Scale of this study due to the interest it represented. One point was awarded for an affirmative answer in dichotomous answers and 0 points for a negative answer. In multiple-choice questions, the score was awarded from 0–very bad to 4–very good or from 0–not pain to 5–much pain or 0–always to 5–never.
In the questionnaire, questions on musculoskeletal symptoms presented with the Nordic Scale 22 are widely used in occupational health to detect musculoskeletal symptoms easily. It is a standardized questionnaire for the detection and analysis of musculoskeletal symptoms, applicable in the context of ergonomic or occupational health studies to detect the existence of initial symptoms, which have not yet constituted disease or have not yet led to consulting the doctor. One point was awarded for an affirmative answer in questions with dichotomous answers and 2 points for a negative answer. The rest of the questions quantified the time of the duration of the episode.
Data Analysis
After assessing normality, normally distributed data were described as mean and standard deviation (SD), nonnormally distributed data were described as the median and interquartile range (IQR) and frequency data were reported as absolute frequency and percentage. For the study of the relationship between variables, statistical tests were used according to the nature of the variables: Chi-square or Fisher’s exact test for categorical variables, Mann–Whitney U test or Student’s t-test for nonnormally distributed and independent data t-test for normally distributed quantitative variables. In all cases, the significance level was 5% (α = .05). Data analysis was performed using IBM SPSS (version 24).
Ethical Considerations
The research project had the approval of the clinical research ethics committees of the different hospitals.
The study variables were registered in the Zenedo.org available from https://zenodo.org/record/4501280in February 2021.
Investigators complied with fair clinical practice laws and the ethical principles for research in human beings described in the Helsinki Declaration version updated in the 64th General Assembly, Fortaleza, Brazil, October 2013. Confidentiality and privacy of personal data had been guaranteed by ensuring compliance with European data protection laws, namely, with Regulation (EU) 216/679 of the European Parliament and Committee of 27/04/2016 (RGPD-Spanish Agency for Data Protection).
Each study participant was handed an informative sheet about the study and had asked to sign the informed consent. Participation was voluntary and anonymous, and the participant could withdraw from the study at any time.
All questionnaires and informed consent documents had stored in the archives of one of the hospitals, where they will remain for 25 years after the publication of this article, after which they will destroy.
Results
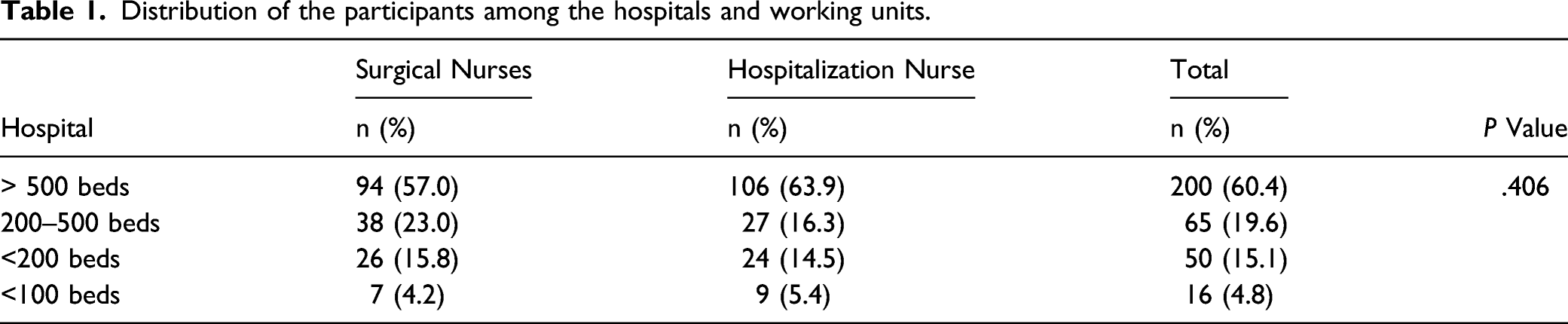
A total of 331 nurses participated in the study, 165 were operating room nurses and 166 worked on a hospitalization unit. Most of the participants were women (87.9%) aged between 22 and 63 years (mean = 42, SE ± 11.59) with around 17.81 years of work experience (SE ± 11.58).
Distribution of the participants among the hospitals and working units.
Characteristics of the participants recruited into the study, by the group.

Perceived health by the study group.

Figures 1 and 2 show differences between nurses and the general population concerning perceived health. Perceived physical health by nurses compared to general population. Perceived mental health by nurses compared to general population.

Nordic questionnaire by group the study.

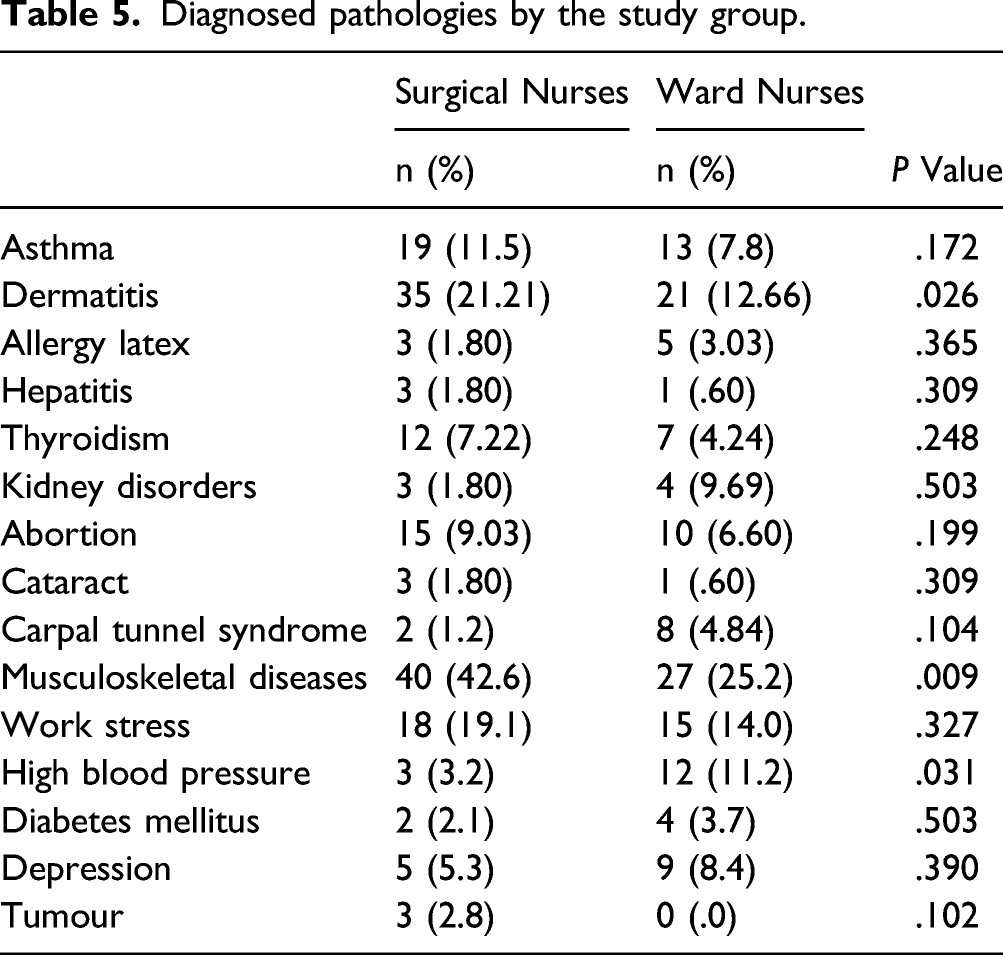
Diagnosed pathologies by the study group.
Discussion
This study looks at the possible presence of the pathologies described in the literature and the participants’ perceived health. Also, it investigated a possible link between any of these medical conditions and the different surgical areas.
In the introductory meeting of the study, it became evident that the list of these pathologies is pervasive, and we decided to focus on the most important ones or those for which the conditions of the operating room nurse presented the most predisposing factors.
The main objective of the present study was to determine the effects of the working environment of operating room nurses on their health compared to hospitalization nurses. According to our results, we can only affirm that the operating room work environment has adverse effects on the health of surgical nurses compared to hospitalization nurses when we refer to musculoskeletal diseases and dermatitis. Compared to the rest of the pathologies studied, no statistically significant differences were observed between both populations. It is appreciated without sufficient statistically significant evidence that there are more cases of the population with thyroid problems in the surgical nurses, with 7.22% (n = 12) of cases, slightly higher than the cases reported by hospitalization nurses that it represents 4.24% (n = 7) of the total (P = .248). In the same way, we observed a slight increase in fertility problems in the surgical population, from the surgical nurses reported infertility in 9.03% (n = 15) compared to 6.60% (n = 10) of affected people in the hospitalization area (P = .199).
Musculoskeletal Disorders
It is highly prevalent internationally among perioperative nurses and is the leading cause of absenteeism and requests to change work posts. 13 Although a part of the sample from surgical nurses referred some pathology, only 10.9% of them requested a change of surgical specialty. Approximately one in three cases of absence among operating room nurses are linked to musculoskeletal disease. 14
Several studies on MSD among perioperative nurses show similar results to this study, regardless of their location worldwide. 23 They reported results similar to our study that 58% of operating room nurses suffered from back pain in the previous 12 months and 85–90% of these continued working results. 11.2% only requested to transfer nurses, who had consequently transferred to another healthcare unit or service, similar to our results, 10.9% of the surgical nurses.
Stress
Individual working conditions make operating room nurses vulnerable to permanent work-related stress. 16 Work overload, a lack of staff or resources, the constant need to learn how to use the latest technology and the urgency of the situations, which require staff to act urgently and responsibly, can trigger burnout syndrome. In our study, 19.1% of the operating room nurses and 14.0 ward nurses suffered from stress. The overall results reflect the situation that the profession is facing currently. All hospital departments are experiencing a significant generational change, making it impossible to replace all the nursing staff. The nursing staff are aggravated by a lack of stability and security, leading to excessive workloads and few incentives to seek professional promotion. It decreases in salaries causing feelings of frustration, ill-feeling and demotivation among the nursing staff.
These well-known aspects directly or indirectly affect nurses’ perceived mental health and negatively affect their lifestyle.
In 2012, Schmidt et al. studied the perceived health of a general population sample using the same SF12 Scale. 24 Therefore, with the results of both studies, it has been possible to compare nurses’ perceived health as a professional group with that of the general population. The scores obtained show that nurses presented slightly lower scores for perceived mental health than the general population. When observing the results about groups of the different age ranges, physical health perception can be lower or higher depending on the participants’ age but not statistically significant. Only the groups under 25 years old and nurses over 55 had a worse perceived physical health than the general population. Mental health is scored with the worst values for nurses when we compare it with the general population.
Contact Dermatitis
Interestingly, in our study, contact dermatitis was significantly more prevalent in one of the hospitals, detected in 20.9% of the nurse participants. The reason for this is known as the concentration of chlorhexidine antiseptic solution in this hospital was increased from .4 to .8% to prevent postoperative infection. Moreover, a higher prevalence of skin conditions in healthcare professionals has linked to higher concentrations of this product. We notified our results to the hospital’s Health and Safety Department to highlight its importance for staff health and safety.
The nurse/patient ratio in Spain is far below the European average. Only five nurses are employed to care for 1000 patients, while the European average is almost nine. This situation directly affects the nursing staff’s work and health, who experience excess workloads in the hospitalization and operating rooms.
Current legislation should incorporate measures to improve the nurse/patient ratio. Many healthcare professionals do not take enough care of their health and do not even follow the advice they give to their patients. Healthcare professions, especially nursing, require a strong social commitment and work under tremendous pressure. This situation can negatively affect the workers’ mood and emotional balance, essential to working healthily and providing patients with adequate care.
The nursing profession’s physical and emotional efforts are very similar in all healthcare departments of the hospital, which is reflected by our results.
Occupational risks are limited as they are carefully controlled by the Health and Safety Departments of the hospitals studied.
Training is one of the most critical areas to prevent occupational hazards and professional diseases. Rather than targeting a specific goal, this should regard to explore and understand in greater depth the situations that arise in this setting, particularly the work environment, the working conditions and the resources available. It is essential to provide continuous training in ergonomics and special apparatus to prevent lumbar and dorsal injuries in all hospital departments. Moreover, prevention protocols of surgical infection should be revised to optimize the proportions of chlorhexidine in soaps to help prevent skin lesions among operating room staff.
In-depth knowledge of the occupational hazards and the actions required to address them will minimize the harm suffered by operating room nurses and ward nurses alike.
The results obtained with a sample of this size help establish initial associations, which must explore in greater depth in further studies.
Limitations of the Study
The sample of operating room nurses was approximately 99% of the permanent staff in the hospitals studied. By contrast, the group of ward nurses used for purposes of comparison was more variable. We excluded intensive care units from the study because of their similarity in many aspects with operating rooms (restricted access to the areas, very specialized nursing care).
The causality of the different medical conditions is varied and can be affected by numerous factors and surgical settings.
Although the reasons why surgical nurses suffer a pathology to a greater or lesser extent in comparison to nurses from another area cannot be determined, a situational mapping was carried out. Such mapping allowed a better understanding of surgical nurses’ health reality than nurses from outside the surgical area.
Conclusions
The nursing profession carries occupational risks regardless of where the activity takes place. The operating room work environment has adverse effects on the health of surgical nurses but without significant differences from hospitalization nurses.
Footnotes
Acknowledgements
We want to thank all the nurses who have collaborated altruistically in our study. We would also like to thank Dr Ignasi Gich and Dr Margarita Aguas for collaborating in the initial statistical analysis of the results and their support. We are grateful to the student Mireia Estrada Ros, who participated in the data collection in one of the study hospitals.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Code Ethics Committee
On the 7/11/2018 with 2018/54-INF-HUSC code ethics committee, the study was approved with idcsalud at Catalunya.