
Abstract
The aim of this theoretical paper is to critically reflect on the ethical and methodological issues that arose during a study that observed nurses’ care-giving in an intensive care unit setting. The authors critically discuss the methodological and ethical issues as well as the practical realities that were encountered when evaluating a complex intervention using unstructured qualitative observations. We describe the process with negotiating access and entering into the clinical field. Moreover, we reflect on experiences related to methodological issues such as the observer role, how to construct field notes, and how to encounter ethical dilemmas and other problems when being an observer in a closed and protected setting like an intensive care unit. We argue that qualitative observations give an insider perspective when studying the conditions for health and well-being. Our experiences can be transferred to other contexts and guide researchers interested in doing qualitative observational studies.
• ○ Intensive care is a complex field in which to conduct research. ○ Caring is difficult to express verbally. ○ Observational research is not fully explored. • ○ The article identifies the methodological issues and ethical dilemmas researchers face when being an observer in a closed and protected setting like an ICU. ○ It reveals the practical realities that were encountered when evaluating a complex intervention. ○ It highlights how unstructured qualitative observations are useful in capturing phenomena that are difficult to express verbally • ○ Qualitative observation provides a valuable perspective when studying caring in different settings. However, careful planning is needed to navigate the ethical and methodological issues this presents.Highlights
Introduction
This paper discusses some of the methodological and ethical issues of conducting qualitative observational research, 1 as well as the practical realities that were encountered in evaluating a complex intervention. 2 The intervention aimed to change an intensive care unit (ICU) environment in a Swedish hospital according to evidence-based design principles; altering the environment in relation to sound, lightning, furniture, textiles, and nature. The study aimed to examine if and how such a refurbished ICU patient room influenced nursing care, that is, if the nurses’ caring actions became more sensitive and directed to patients’ well-being and recovery. 1 We concur with Mulhall 3 and Author 4 that unstructured non-participation observation from an interpretative approach is fruitful when examining the physical environment and interaction. To gain access to an ICU is complex per se, and today’s outbreak of the COVID-19 pandemic increases this complexity. The pandemic has led to suffering for patients and their families and caused tremendous demands on ICU staff and their work environment. This means that the problems and dilemmas connected to data collection through observations in ICU are particularly relevant to discuss and to further develop.
Background
The concept of environment has received limited attention in nursing research, often being taken for granted as a passive frame of reference within which professional caring occurs,5,6 although interest in the environmental impact of delivered care has had a revival lately.7–9 This neglect is especially the case in relation to the intensive care setting. This is a significant omission given the particular environment of the ICU with its domination by high tech equipment and round-the-clock medical regimens. The change to light sedation regimens have also made patients more aware of their environment,10,11 this coupled with disrupted circadian rhythms leads to up to 80% of patients experiencing delirium.12–15 These disturbances often remain after discharge. Concerns about the traditional ICU environment and its influence on patient well-being led to the development of an innovative program of research which aimed to assess the impact of an evidence-based design approach to the ICU environment on patient health and well-being.2,12,16,17
Refurbishing a Patient Room According to Evidence-Based Design
The concept of evidence-based design (EBD) means to base decision making about the environment on the best available research findings.18,19 One room in a Swedish hospital ICU was transformed using this approach combined with an additional design goal of sustainability and a desire to create a home-like milieu. 20 At the same time, it was important that the design did not compromise safety, function, and followed national guidelines for an ICU patient room. 21 Interior colorings, textiles, and furniture were chosen according to the “green list” and to be in soft pastel colors. Sound absorbent materials were used on the walls, ceiling, and floor. A cyclic light system was installed that was digitally altered to strengthen the usual 24 hours circadian rhythm. Outside a patio was decorated with small garden furniture and greenery. This green area formed part of the patients’ view through the window but could also be accessed by the patient’s visitors.2,18 The evaluation of the new ICU environment was informed by principles of complex intervention research and health geography22,23 and underpinned by a caring science perspective.24–26 This perspective is fundamental to nursing practice in Scandinavian countries and is characterized by a view of professional care as a commitment to prevent suffering and maintain the health, integrity, and life of others.27,28 The research program used both qualitative and quantitative approaches. This included the use of non-participant unstructured observation which is the focus of this paper.
Designing the Qualitative Observation Study
In an earlier study in the research program, nurses described how they felt that they provided nursing care with a more caring attitude in the refurbished ICU room. 16 Thus, a subsequent study was designed to examine this reported change in caring attitude in more depth including observation. 1 The focus for the observations was to capture the meanings of caring and nursing activities performed in the refurbished room and in a traditionally designed room situated next door. All the observations were conducted by one researcher, who was an experienced critical care nurse but who had not worked in the research setting. The research study involved conducting 4 observations in the intervention room and 6 in the control (non-refurbished) room. 1 Observations were completed in the control room before moving onto the intervention room to gain a sense of usual activities and interactions as a baseline. The data gained from the observations were discussed and analyzed by the research group and the results later published. 1
A working shift, usually consisting of a critical care nurse (CCN) and an assistant nurse (AN), was the focus of each observation. The participants consisted of 7 CCNs, 1 CCN-student, and 7 Ans (15 participants in total). The sample varied in terms of gender, age (22–55 years), and ICU work experience (3 weeks–12 years) Across both rooms a total 47.5 hours of observations were documented by careful field-notes (Box 1). The field-notes were written by hand during the observations and transcribed shortly after each observation. Both daytime and evening shifts were observed for between 4 and 6 hours a day. During the observations, the researcher sat quietly in a corner of the room that provided a full view of the actions of the nurses. However, there were times when she moved her position to obtain a better view of nursing activities or if additional space was needed by the staff. The field-notes recorded both descriptive and reflective notes 29 about the setting, the atmosphere in the room, the activities occurring, and the interactions among the various actors.
The non-participant, unstructured observations were carried out within a naturalistic and interpretive paradigm,3,30 meaning that data were gathered as a process where the everyday experience of people was captured in their natural settings. Following the completion of the observations, participants (nurses) were invited to take part in a qualitative research interview. 31 The observational and interview data were analyzed together using a hermeneutic-phenomenological method built on the writings of Paul Ricoeur and developed for nursing research.32,33
The aim of this actual paper is to highlight and critically reflect on the ethical and methodological issues that arose during a study that observed nurses’ care-giving in an ICU setting. Details on the research methods are provided in another publication.
Negotiating Access to the ICU
The refurbishment of the ICU room itself had involved gaining the approval of the hospital managers, chief physician, and head nurse. Subsequently, it had been important to engage the ICU staff in the planned transformation of the room and in the research program itself. Since the start of the research program, researchers and doctoral students had visited the setting, and data collection for several studies had taken place at the ICU. This collaboration between the researchers and the unit had laid the foundation for future alliances. This involved the research team giving seminars about the research (including the use of observational methods) and experts in environmental design (eg, architecture, textile design, Feng Shui) giving presentations about the planned redesign of the room. These seminars were well attended and proved to be important in ensuring that the ICU nurses fully understood the reason for the researcher’s presence, particularly given they were sharing the same space for lengthy periods of time. In addition, the researcher was dependent on their assistance with the study as well as their commitment to working within a transformed ICU environment.
Despite this previous collaboration, each study and period of data collection required access to be negotiated—to the unit, to the staff, and to the data of interest. Once approval from the hospital had been received, the researcher met with the ICU ward manager to negotiate how the observations would be carried out in practice in both the redesigned room and the control room. This involved obtaining information about staff shift patterns and daily routines. A decision was made by the Ward managers, for the researcher to wear the same “scrubs” that were worn by the staff. This was seen as both enabling the researcher to blend in with the environment and comply with the hygiene regulations of the unit. The observer also gained access to the break room for the staff which enabled social contact between the observations and interviews. However, to ensure that it was clear that the researcher was not a staff member, she wore a university name badge. The researcher was given access to the ICU in the form of an entrance card and codes to the staff’s changing room, so that she could come and go as the rest of the nursing staff.
Procedures and Considerations in Relation to Ethics
In addition to approval from the organization, research ethics committee approval was required before the observations could commence. In Sweden, research ethics approval is governed by the guidelines of the Swedish Research Society (The Swedish Codex), the Helsinki Declaration adopted by the World Medical Association (WMA) in 2013, 34 and the All European Academies (ALLEA), that is, the European code of conduct for research integrity. Written and oral information was provided to staff about the study at its outset and then repeated during the unit’s regular staff meetings. This included information about the voluntary nature of participation, confidentiality, and their right to decline participation. However, the very specific focus of observations was not disclosed to participants prior to the observations, to attempt to prevent this knowledge influencing their actions and interactions. The presence of the researcher was also highlighted by the senior nurse during staff changeovers, and any nurses who did not wish to participate in the study were not allocated to the rooms where observations were being carried out. The study followed what Polit and Beck 35 conceptualize as process consent, meaning that informed content from the participating nurses was viewed as a process that was subject to ongoing negotiation.
For example, if any nurses found the observation to be too intrusive, they would be able to choose to work in a patient room that was not allocated to the study. Informed consent from the research participants was collected before conducting the interviews. At that time, the staff received information about the aim of the observations and the study and had the chance once again to decline or give their consent of participation. Research ethics committee approval (Reg.XXX) was received without any requirements for amendments to be made to the research plan. Later in the paper we will discuss the real-life ethical dilemmas that had to be negotiated during the study itself. According to Swedish legislation, patients are autonomous and therefore capable to make their own decisions regards consenting to participate in research. Although critically ill patients are considered vulnerable research participants and therefore require thorough ethical consideration. 35 The researchers were conscious of the vulnerabilities of ICU patients and the need for their rights and dignity to be protected.36,37 Consequently, this fact was problematized in the ethical approval application form. A particular issue related to whether patients and their next of kin also should give informed consent, despite not being the research participants. Under Swedish research ethics regulations as the focus of the observations was on the ICU nurses’ activities, the consent of families or patients was not required. This interpretation may not be consistent with the research ethics regulations of other countries but complied with the regulation governing the study setting, in this case, Sweden. The Scandinavian countries have different ethical legislations and praxis compared to the US and UK concerning this. We strongly argue that it is crucial to be aware of and following the legislation in the country where observations are taking place. However, if observations were conducted when the patient was awake or if visitors were present, the researcher explained the reason for her presence to them and obtained consent. Furthermore, the researcher did not attend any handover reports where personal information about patients was shared. The research ethics application had highlighted that the observations would be carried out by a researcher who was an experienced ICU nurse who was sensitive both to patient vulnerability and family distress and thus aware of the need to withdraw from observation when appropriate. It was emphasized that the observations would not affect the care of patients or family members or the running of the ICU and that they would focus only on nursing activities. The staff had the mandate to stop the observer from entering the patient rooms if the situation was inappropriate for observation.
Navigating Methodological Issues
Do observations reveal a different perspective or “reality”?
An earlier study in the research program revealed that nurses described how working in the redesigned room made them feel more alert and promoted the quality of their caring. 16 We were interested in exploring these findings further using a naturalistic and interpretive approach to understand how the environment influences caring. 30 Unstructured observations are rarely used in nursing research, yet they provide a valuable means of gaining a holistic insight into interactions and illuminating the contextual influence of the physical environment. 4 However, at the same time, it is important to recognize that the reality perceived by the observer is conditional; it is multi-voiced and open to manipulation (whether deliberate or not) by the observed. 38 The analysis of the observational data from our previous study suggested that the nurses’ caring attitudes, that is, sensitivity to individual patient needs were not influenced by the ICU room in which they were working but were connected to the individual nurse themselves, that is, some displayed a more caring approach than others. 1 This conflicted with the interview data from another study 16 in which nurses related their caring to the environment. Mulhall 3 states that a primary reason to use observations for data collection is to investigate if participants’ accounts are consistent with their actions. She argues that an interviewee has more possibilities to govern the content in the conversation, whereas in observation sessions, the researcher is freer to choose what to observe. Data are always open for interpretation, and a possible interpretation of our findings could be related to the role of the observer and the observer’s preunderstanding and theoretical knowledge in the literature concerning the concepts and application of caring science into clinical practice. It could be that the observer might not interpret an action as being caring, but on the other hand the nurses might see it as a caring act. However, if returning to the analyses of data that were worked through using phenomenological-hermeneutics,33,39 it can be argued that a text or scene is always open for several interpretations. The interpreter, however, must be able to move from a subjective to a distanced position and to present arguments for the most probable interpretation, that is, to consider if it is reasonable and likely. 4 To maintain rigor in unstructured non-participating observations, as in all qualitative analyses, means to comprise a careful collection and critical analysis of data and a transparent reporting of findings.
Being an Insider or an Outsider
In this study, the researcher observing the nursing activities was an insider, that is, someone who shared the characteristics and experiences of those being observed, 29 but had not worked in the actual unit. While there are disadvantages to this role in terms of overfamiliarity with the setting blinding a researcher to the actions and interactions occurring within it, in this study being an insider appeared to facilitate access to the ICU setting and provided a degree of theoretical sensitivity that was important during the observations and data analysis. 4 However, to guard against making assumptions or taking for granted what was being observed, the researcher made detailed descriptive field notes and kept a reflective diary (Box 1). In addition, prior experience as an ICU nurse provided the researcher with the knowledge and confidence to change her role from a non-participant to participant observer if the situation and the safety of the patient required her to act.
The ICU nurses observed were aware that the researcher shared their professional identity. Indeed to “fit-in” and reduce her intrusion in the setting, it was decided by the Ward managers, that the researcher would wear the same uniform as the staff. Nevertheless, there are risks to presenting the same outward appearance as the observed. Despite the different name badge, patients, visitors, and other staff members may have mistaken the researcher for an ICU nurse which highlighted the importance of the researcher introducing herself to people entering the ICU room. Since the staff was aware of the researcher’s professional identity, it is possible that it may have impacted on their professional behavior while the observer was present. While it is unknown if the staff changed their behavior due to the presence of the researcher and their knowledge about the study focus, the follow-up interviews with the participating nurses 1 examined their perceptions of her influence on their actions and interactions. These interviews revealed that they forgot about the presence of the observer after a few minutes.
Moving From a Non-participant to a Participant Role
The researcher adopted a non-participant observer role. However, as noted earlier due to her insider role, there were incidents that led her to moving to a participant observer role. Incidents observed were responded to differently depending on the researcher’s assessment of the level of risk to the patient. In one situation, a life-threatening incident was observed by the researcher but not by the ICU nurse, in which a patient attempted to extubate themselves. Here, the researcher stepped in immediately to prevent this action. In another situation, the researcher observed that the ICU nurses had missed taking a vital blood pressure measurement for a patient. After giving the nurses reasonable time to recognize their omission, she raised the error with them directly. Being an insider meant that the researcher had a professional and moral duty to intervene. Although Angrosino 30 notes that all qualitative researchers using observational methods have obligations to prevent harm to their research participants, but in an ICU environment it may require specialized prior knowledge to identify and appropriately manage observed patient safety incidents.
Discussion
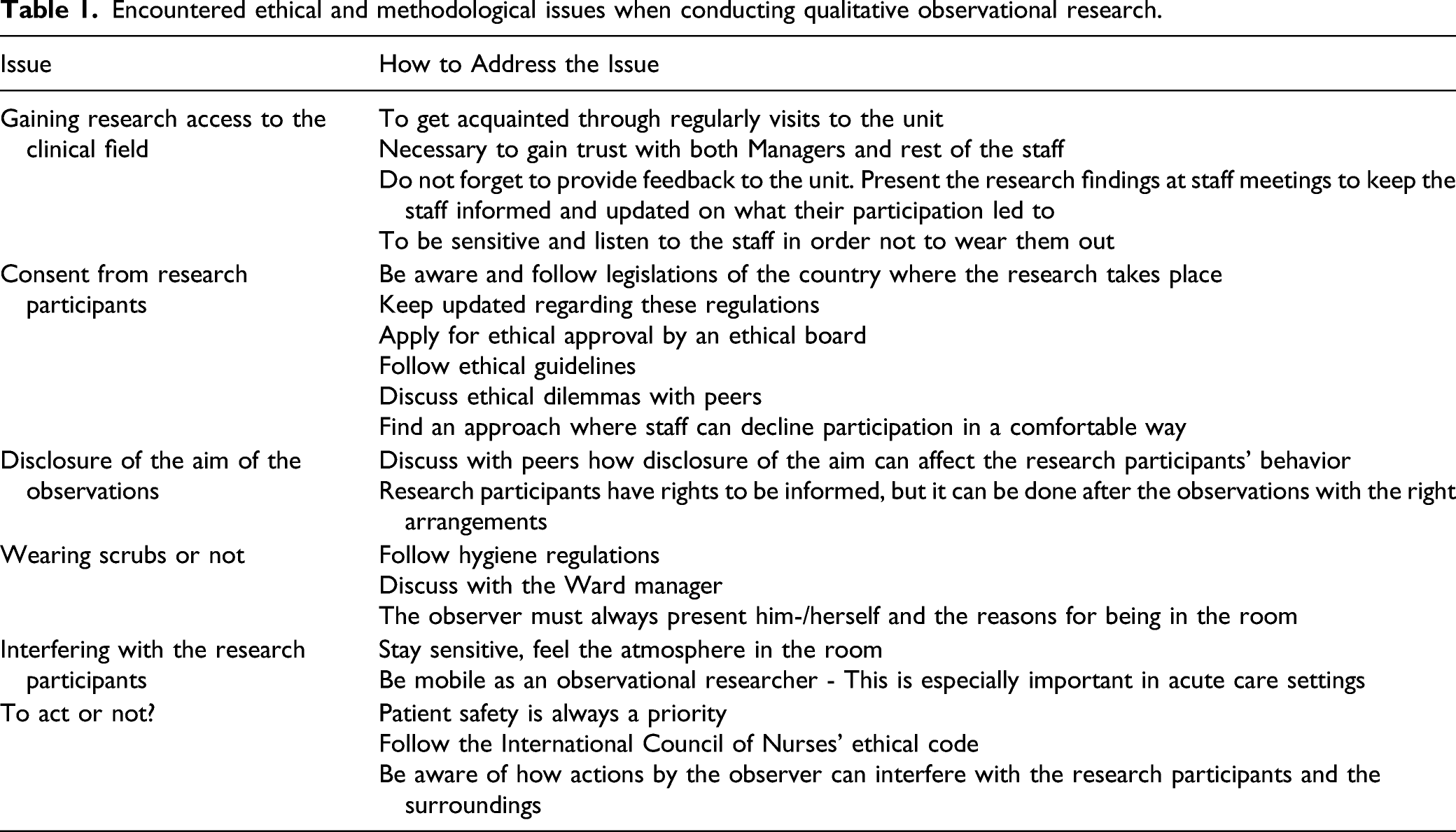
Encountered ethical and methodological issues when conducting qualitative observational research.
Examples of Field Notes From the Observations

The fact that the study had received approval from the ethics committee also facilitated access to the setting. However, of most importance was that the managers and staff were motivated to facilitate data collection as there was a strong desire to improve their work environment. Our experiences suggest that it is a prerequisite for observers to have insight and knowledge both about the type of care and the environment being studied when it comes to entering a clinical field like an ICU. Research has described this area as frightening and shocking for a person who is not familiar with intensive care.1,40 We therefore consider that it was important that the observer was an experienced ICU nurse who could build positive relationships with staff and gain their trust, but with an outsider perspective. Since the aim of the study was to illuminate the meanings of caring and nursing activities performed in different designed ICU patient rooms, 1 it was crucial that the researcher had experience of intensive care and caring practices. We argue that researchers should study phenomenon within their own field of expertise. Moreover, it is the aim of the study that determines whether an insider or outsider perspective is suitable for an observational study. Although there is value in having neutral observers who see the “taken for granted”.
The fact that the observer was an experienced ICU nurse meant that she had a preunderstanding of the routines, traditions but not personal relationships of staff which helped them in seeing with an attentive and receptive gaze.4,41 In addition, this meant that actions and interactions were observed and interpreted through a caring science lens which underpinned the study. This approach is founded on the writings made by Katie Eriksson 42 as well as theory of professional growth as a nurse described by Patricia Benner.43,44 The study had a phenomenological-hermeneutical approach, where lived experiences were in focus. 32 This was used as a framework to assess the performed and given care. The insider–outsider perspective in observations and ethnographical studies has been debated. 45 We and other researchers argue that it is not a dichotomous approach 46 rather a movement between these approaches.
When a researcher, in this case, a trained ICU nurse, takes on a non-participant observer role in an ICU setting s/he may witness situations that risk patient safety. This becomes particularly salient in an ICU setting where patients are critically ill, and treatment is connected to fast decisions and technological equipment. This means that the researcher may need to be able to rapidly assess what is witnessed and know when to act. In an editorial, 47 the researchers discuss the phenomenon of “guilty knowledge” which means witnessing situations that might be reported to an authority. Here we argue that although it could be misinterpreted that the observer was a member of the staff, it was also a patient safety issue that the observer could and did interact when needed. Thus, observation is connected not only to seeing but also to having the knowledge and courage to decide when to act. Consequently, it is important for there to be ongoing discussions within research groups about ethical dilemmas that might arise during observation sessions and how to manage these. 4
We found conflicting results between a previous interview study 16 and the observations 1 in relation to the influence of the ICU environment on the caring actions of nurses which confirms the usefulness of unstructured non-participation observation. There is no standardized way to record field notes. 48 The observations in this study were guided by the themes; Time, People, and Context, as described in methodological texts concerning observations and ethnography.49,50 It is important that the researcher takes a rigorous approach in making field notes that involves careful contemporaneous description of what is observed before moving to an interpretation process using both subjective and objective approaches.4,32,44 Our field notes focused on the atmosphere and people present in the room, their actions, and interactions. Moreover, notes were made about the technical equipment, sounds, and lighting as these factors influenced the environment as well as the view from the windows into the outside green area. In the study, 1 the observation sessions were followed by an interview with the staff who had been observed. Here, the field notes were used as a tool to enable the sharing of the events in the observation session as well as deepening the conversation between the interviewees and researcher.
Conclusions
In this paper, we have presented our personal reflections about our experiences of conducting unstructured non-participation observations in an area that is often considered as closed to such research due to the vulnerability of critically ill patients. Our recommendations for conducting observation work are grounded in our experiences in hospital high-tech environments, but we also consider them transferable to other contexts.
Footnotes
Acknowledgements
We are grateful to the participants for their willingness to share their everyday caring practice.
Author Contribution
The authors made a substantial contribution to the design of the paper, and we have all taken part in drafting and reflecting on the content and consequently take public responsibility for the content.
Declaration of Conflicting Interests
There is no conflict of interest or funding in relation to the work with this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.