
Abstract
The critical role of the health workforce in the function of the health care system is undeniable. In times of disaster and public health emergency, the importance of this valuable resource for the organization multiplies. This scoping review was conducted to identify, analyze, and categorize interventions to improve willingness to work in times of disaster as well as the existing knowledge gaps in the topic. For this purpose, four databases were searched. These included Scopus, PubMed, WOS, and World Health Organization observatory, and they were searched for papers published from July 2000 to September 2020. Studies of the English language that described strategies to improve human resources for health willingness to work during times of disaster/public health emergency were included. Full-text papers were screened by authors and data extraction was done according to self-designed form. Framework analysis identified key interventions based on human resources for health action framework. From 6246 search results, 52 articles were included, a great portion of which was published in 2020 probably due to the COVID-19 pandemic. Northern America was the region with most studies. From 52 included studies, 21 papers have reported the interventions to improve willingness to work and 31 papers have explored factors that affected a willingness to work. The interventions used in the studies were categorized into five themes as Leadership, Partnership, Financing, Education, and Organizational policies. The most and least interventions were financial and partnership respectively. The review identified a wide range of feasible strategies and interventions to improve human resources for health’s willingness to work at times of disaster that are expected to be effective. Organizations should let the staff know these decisions and as a necessary step in every organizational intervention remember to evaluate the impacts.
Disaster and emergency conditions put health care professionals under extreme pressure. The 2019 Coronavirus pandemic showed that health care organizations without motivated and efficient human resources could not achieve disease control and prevention. Therefore, health managers and policymakers have an important role in implementing effective measures to improve retention and willingness to work.
This review revealed a wide range of approaches on how to address intervention improves willingness to work in times of disaster. The findings revealed a strong perception that the “Battle Buddy” system that is derived by the US military for psychological support should be implemented to increase the resilience of frontline health workers.
Generally, the result of study will help policymakers take steps to manage and mitigate the negative effects of emergency conditions and developing evidence-based roadmaps, strategies, and interventions for moving forward.Highlights
Background
Due to the nature of sensitive professions, health workers are constantly exposed to burnout, so the phenomenon of leaving the service is one of the main challenges for managers and policymakers of health care systems in many countries. 1
This becomes more of a problem when pandemics and emergencies occur because they must be available for rescue operations by wearing heavy protective clothing at all hours of the day and night, and therefore the most high-risk group in terms of susceptibility to disease, especially infections.
These factors cause stress and physical, mental, and psychological pressures on the treatment staff, which puts them in a dilemma of staying and going.2,3
Studies show that in Germany 28% of health care orkers (HCWs) would avoid reporting to work and providing service in pandemics. Other studies in the USA show that 42.6% of HCW are unwilling to respond to the future events of an influenza pandemic. This portion is 21.7% for the next SARS epidemic.4,5 Today, the world is struggling with the COVID-19 pandemic which has involved 112, 660, 768 people till February 24, 2021 as the WHO reports. 6
This outbreak sets new challenges in the way of human resource management including uncertainty, lack of preparation, financial limitation, exacerbating psychological problems, burnouts, and potential threats to both workers’ health and the safety of loved ones due to the contagious nature of the disease.7,8
Studies that consider the COVID-19 pandemic a long-term disaster suggest factors and interventions that can be used to increase HCWs’ willingness to respond as a vital part of managers’ plans for the future.9,10 Many studies have been conducted to find factors affecting willingness and effective interventions in similar situations and in recent years, the number of similar studies has shown significant growth in number which can be due to an increase in the occurrence of contagious disease outbreaks, wars, and other long-term and complex disasters.11–14
Since the start of the COVID-19 outbreak, health care professions have worked in the frontlines of the response to the pandemic for more than one year and the situation is yet to improve so there must be evidence-based plans to increase the system’s rate of recovery and preparation for next waves of the outbreak.
This study is a scoping review of effective interventions to increase HCW’s retention and willingness to work during long-term and complex disasters. It aimed not only to report major factors that affect the willingness and effective interventions that can be implemented to control these factors but also to consider and report evidence gaps to be focused on in future studies. It also focuses on finding appropriate interventions and using them to make policies that would help increase the workforce’s willingness to respond in many affected countries.
Methods
Design
This scoping review was conducted based on Arksey and O’Malley framework. It consists of five stages: scoping, searching, screening, data extraction, and data analysis.
15
Although these stages are stated linearly, a visualized figure was developed to fill any potential overlap (Figure 1). The Arksey and O’Malley steps for scoping review.
16

Among 14 types of reviews, 17 scoping review was selected because it is characterized by the inclusion of a wide range of study designs and outcomes, which enables exploration of the literature in a specific issue and displays the nature of background knowledge.
Scoping
To become familiar with the existing literature, an exploratory search in MEDLINE using MeSH term (Medical Subject Headings) was conducted. The objective was to examine examples of potentially relevant studies and based on that information, inform the development of preliminary eligibility criteria and generate a more elaborate search strategy. Authors screened titles and abstracts. Together, they developed eligibility criteria based on the research question.
Eligibility Criteria
Inclusion criteria
Articles considered disasters which engaged health care system directly, those studied HCWs as a target population, and only English articles are included in this study.
Exclusion Criteria
Conference papers and abstracts as well as studies that did not report strategies and interventions related to willingness to work were excluded. Also articles studied short-term disasters were excluded.
Searching
In the scoping step, a comprehensive search strategy was cooperatively developed by using the eligibility criteria provided and sharing exemplar studies with a medical librarian. This was according to the Peer Review of Electronic Search Strategy reporting guidelines.
Specific search queries, PubMed databases.

Screening
Initially, the titles of all articles were reviewed and articles that were incompatible with the aims of the study were excluded. Subsequently, abstracts and full texts of the articles were studied. Studies that did not meet the inclusion criteria and had poor correlation with study aims were identified and excluded, respectively. A researcher-made data extraction form was developed to extract data. At first, as a pilot for data extraction form, the data of 52 papers were extracted.
Since it was essential to study the full text of the included studies to extract data, this was conducted by the research team in two stages. However, in the third and fourth stages of the Arkesy and O'Malley frameworks after the initial extraction of the data from the selected studies, the research team re-examined the data in two sessions carefully and finally, the studies were re-screened by the research team to include precisely relevant and high-quality studies.
The authors independently screened all titles and abstracts and Inconsistencies were resolved by retrieving full‐text items, which were screened concurrently with data extraction.
Data Extraction
A data extraction form was developed by two of the authors to collect information on study characteristics including author, publication year, country, study objective, study design, main intervention, and findings. The authors extracted data from all articles.
Data Analysis
Framework analysis was applied to synthesize the data, which is a process for identifying, analyzing, synthesizing, and reporting patterns within the text and is generally used in qualitative data analysis. Therefore, the first and second authors qualitatively analyzed the included papers through framework analysis.
The steps for data analysis consist of: Familiarity with the text of articles (immersion in article results by reading several times), identifying and extracting primary codes, organizing codes into related themes, reviewing and completing the results of each theme with the use of results of the articles, and ensuring the reliability of the themes and the results extracted in each theme (In cases of disagreement between the two authors, the dispute was referred to the third researcher). Endnote X9 software was also utilized to organize, as well as identify duplicates. Textual data were analyzed using a thematic analysis approach manually.
Furthermore, to categorize the extracted data according to the areas of human resources for the health action framework,6,18 and the components of the health system (Figure 2), studies were again reviewed by three researchers and the areas and functions appropriate to the intervention were selected. In case of disagreement between researchers, the study was reviewed by a fourth person who was an expert, and with the authors’ consensus, the proper function was selected. Human resources for health action framework.
Results
From 6246 search results, 2890 were excluded as duplicate papers, and 3013 were omitted in the stage when titles and abstracts were reviewed. Also, of the 343 articles entered in the full-text review phase, 291 were excluded due to lack of appropriate information and lack of reporting of the required information as well as re-screening of the full-text. Finally, 52 articles were included in the study. Figure 3 displays the PRISMA flowchart. Among 52 studies, 21 papers discussed the interventions related to willingness to work under emergency conditions and pandemics and 31 papers elaborated the main factors that could be considered in the disaster status. PRISMA flow diagram.
Trend of Publication
The time trend of the studies’ publication shows that most of the studies were published in 2020 because of the COVID-19 pandemic. In addition, an aggregation of papers is observed in 2015–2017 that occurred as a result of Ebola epidemics around the world. We can see a plateau of studies on the chart between 2009 and 2014 that was the result of influenza and MERS pandemics. Other disparities in time trend of publication are related to ones conducted to study wars or other crises and disasters distributed in different years. (Figure 4) The time trend of studies’ publication on willingness to work under disaster condition.
Country of Study
Characteristics of included studies considering interventions to increase health care workers’ willingness to work in.
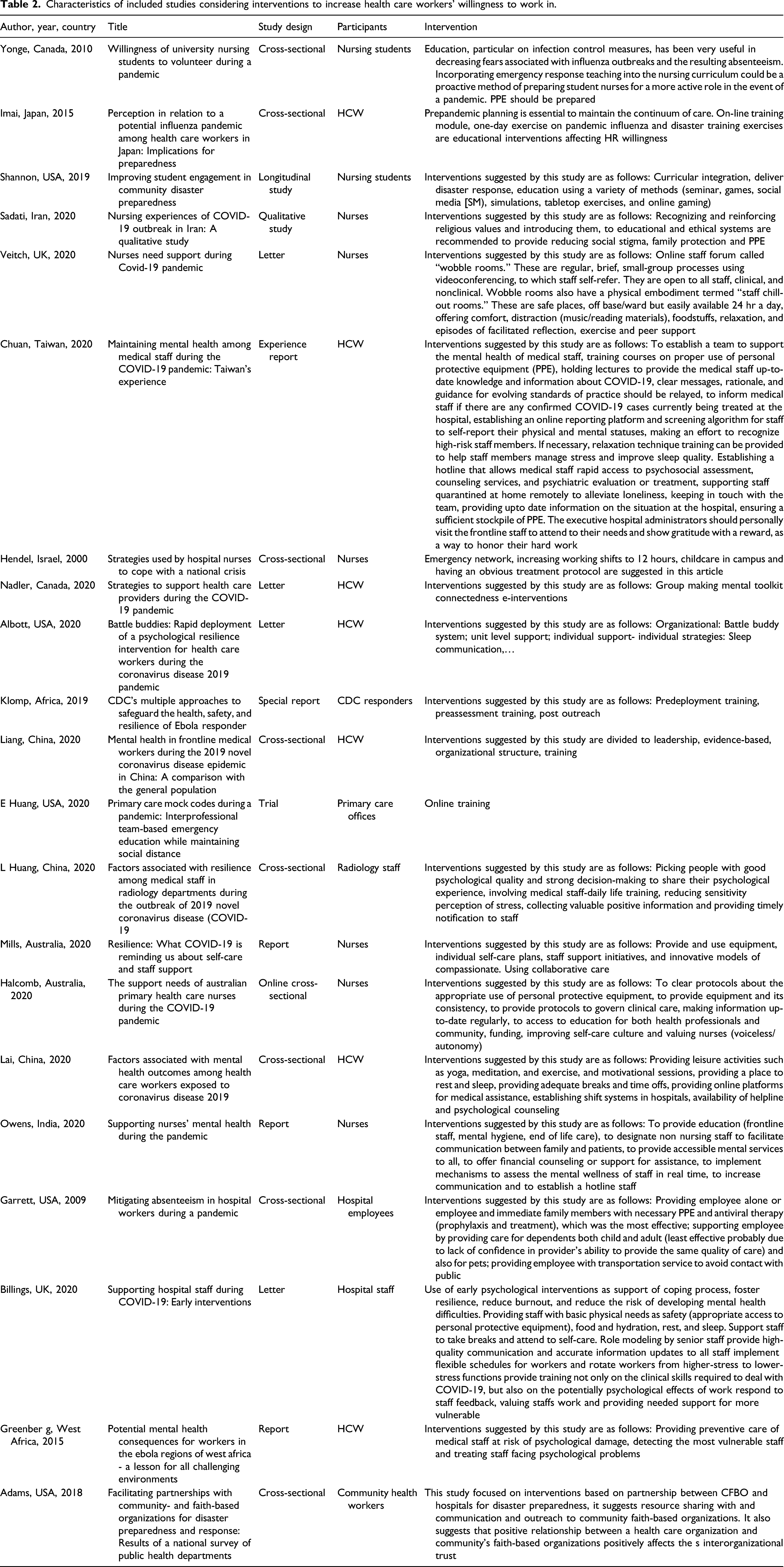
Interventions
According to the Human Resources for Health Action Framework, interventions from 21 studies were categorized into five main themes, including Leadership, Policy, Partnership, Finance and Education. The most and least interventions were financial and partnership, respectively.
Theme 1- Financial Intervention and Strategies
Lack of personal protective equipment is reported to be a major problem affecting the sense of personal safety and as a result, decreasing workers’ willingness. 19 Inadequate supply of personal protective equipment was reported as a problem during previous pandemics and epidemics.20,21 Without adequate physical protection, the perceived risk of employees’ contagion increases and this will affect the staff’s willingness to work. A study showed that protecting staff and their immediate family with PPE and antiviral therapy is expected to have the most effect on mitigating absenteeism. 22 Additionally, studies suggested training plans to meet the efficient usage of equipment.7,9,23–25
Some studies consider direct financial supports like an increase in wages to be ineffective in complex disasters. 26 However, indirect financial supports like childcare and elderly care services, special restrooms for frontline workers, free screening and treatment are reported to be effective. As family safety was a prominent factor in these findings, a greater amount of likeliness to work will occur when antiviral medication or vaccine is provided to both the nurses and their family.27–29
Theme 2- Organizational Policies
Psychological support, information, working environment, and employee assessment are its principal subthemes. These decrease cadres’ burnout, mental distress, and absenteeism. 30 Interventions involving psychological support can be divided into prevention, screening, and treatment strategies. 26 All interventions are considered at three levels: individuals, units, and organizational.
Most articles focused on prevention using planned meetings with psychologists for at-risk workers at individual level and group talks and sharing motivated workers’ experiences at the unit level. General psychological workshops are also suggested at the organizational level.20,23,31,32
There is also a significant amount of attention to screening programs especially the ones on the online platform. 33 Treatment strategies were not suggested as primary forms of intervention; however, free treatment services for workers and their family were suggested. 34
Information is considered in collection and function dimensions. Data collection is the primary step in all HRM functions. To have effective policymaking, data of risk factors affecting the staff and what they need should be gathered. 3 They should also create ways to become aware of evidence-based and innovative solutions. 8
Employees need clear, regular, and up to date information about the disease, mortality rate, and the supply of equipment. It is vital to create a trustworthy climate of situational awareness in hospitals and administrators are responsible to increase the data quality.26,35
There is a significant gap in knowledge on this subtheme. Although articles mentioned the importance of this factor, few interventions have been implemented in this area. Studies on working environment interventions suggested establishing hotline staff, using nonprofessionals as supportive patient care and to provide longer work hours especially during wars.25,26,36 The assessment of current, future, and quarantined workers seems necessary. 26 To keep in touch with quarantined workers and not to leave them alone, improve their sense of worth. Predeployment assessments help recognize those volunteers with psychological and physical risk factors. 32
Theme 3- Educational Intervention and Strategies
This theme is based on studies that focused on education and training, considering three subthemes: 1. 2. 3.
Theme 4 – Leadership
As stated in several articles the sense of being valued by the organization, authority in work as a professional and the possibility of expressing ideas, suggestions, and bringing conflicts to the leaders are the main willingness factors that can be discussed in this theme.3,20,26,41,42 Direct communication between managers and workers and frequent visits of units involved with disaster are recommended. 25 This theme is ignored by administrators despite its cost-efficiency. There is a need for more evidence and interventions to prove its effectiveness. 43
Theme 5 – Partnership
It mainly discussed communications. Inviting qualified, motivated, and successful cadres to exemplify, social and professional championship for frontline workers, and using battle buddy strategy are major interventions considered in this theme. The “Battle Buddy” strategy provides consistent psychological and professional support in an uncertain and stressful working environment. 8 Another suggestion has brought on by the articles focused on this theme was cooperation with community faith-based organizations that supported the sharing of knowledge and resources. 44
There is a narrow border between these themes. Some interventions can be placed in several themes. There is no clear quantitative data on interventions efficacy and effectiveness since most studies did not assess the outcomes. Besides, lack of attention to the ethical and legal condition of workers’ willingness in disasters is recognized which needs more researches in the future.
Our study is unique considering both factors affected willingness and interventions to improve it.45–49 This approach makes more comprehensive vision for researchers in analyzing data. In addition, we used common intervention themes with the HRH framework of the world health organization (WHO). The results of the included studies are summarized in Table 2 as a supplementary file (Appendix A,B).
Factors Affect Willingness to Work
Thirty one articles discussed factors that affect human resource willingness to work in disaster condition. Researcher categorized these factors into demographic factors (4 subtheme), working environment (1 subtheme), employees’ self-condition (7 subthemes) and organizational factors (5 subtheme) in order to comprehend the relation of these factors’ themes and intervention’ themes better (Table 3). Characteristics of included studies that considered factors associated with health care workers’ willingness presented to Table 4 in the supplementary file. Countries included in the study. Characteristics of factors affect willingness to work (N = 31). Characteristics of included studies considering factors associated with health care workers’ willingness.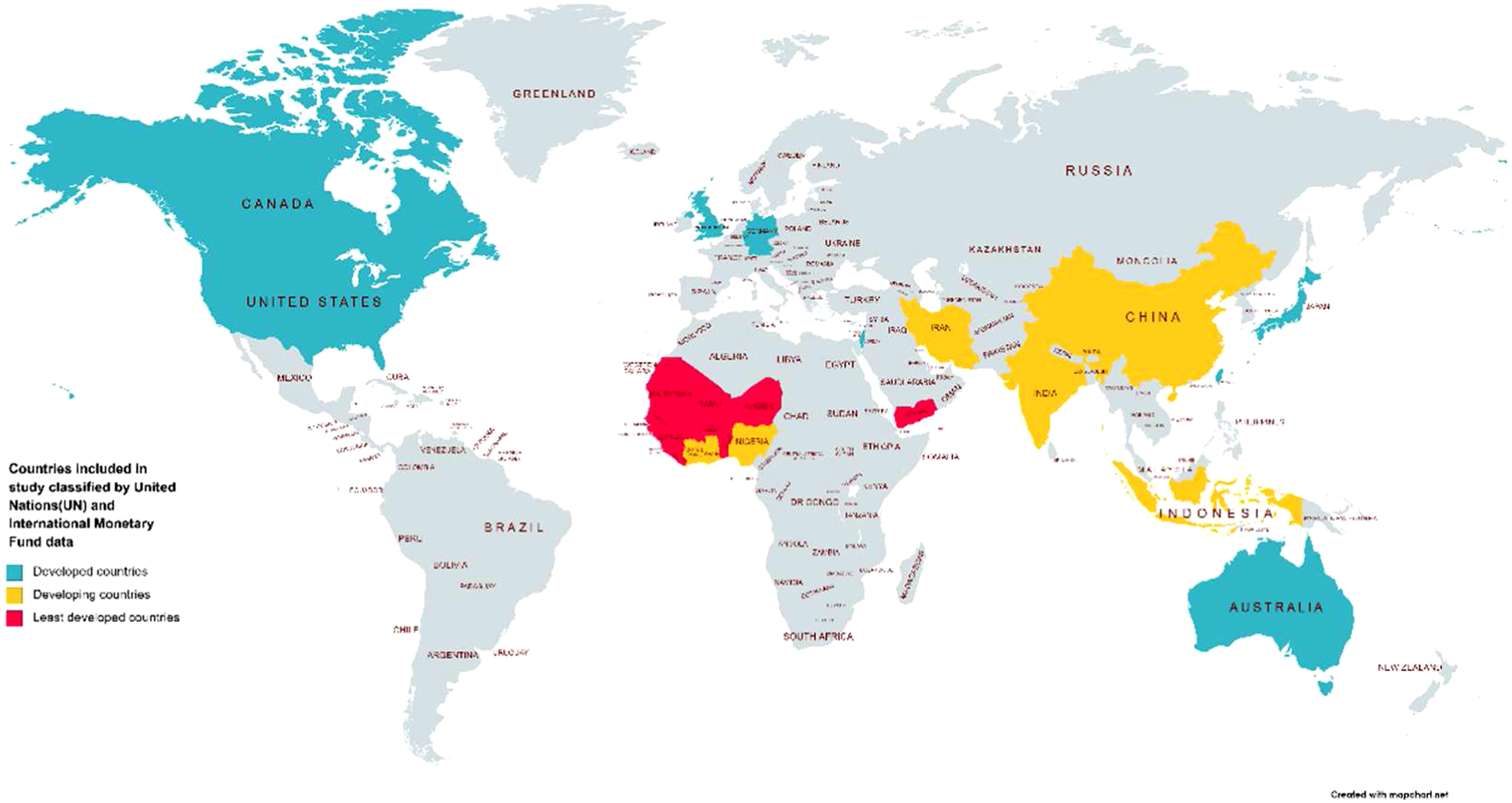


Gaps in Research
This study found a significant ignorance of partnership as interventions and themes were discussed only in the health care system while willingness and hesitation factors caused by disasters were also connected with other aspects of workers’ life.50,51 This study suggests more researches to be conducted on organization policies, leadership and partnership themes and interdepartmental cooperation (Figure 6) Gaps in knowledge.
Discussion
This study focused on determining strategies and interventions implemented to increase the resiliency and willingness to work in HCWs during complex disasters. At the time of writing, many countries throughout the world are struggling with the COVID-19 pandemic affecting all aspects of the health system functions and decreasing the workforce’s willingness to work.
It defines five major areas of action based on intervention types of 52 articles involved in our study and the WHO framework of HRM. 18 Although there are demographic factors like gender and age that affect employee’s willingness to work, this study does not discuss them because these factors are not changeable for current workers.52–55 These factors are considered while recruiting workers in a time of disaster or while changing workers’ tasks to cover the extra workload.
Managers need to guarantee a sense of safety and health for health care workers and their families. Evidence shows that simply providing adequate personal protective equipment for workers increases their willingness to work. A related but less expensive option is to offer nurses scrubs and a place to shower before returning home. 27
Knowledge of the disease and self-care are also powerful tools. They increase both the nurse’s ability to feel safe when caring for patients and the likelihood that effective infection control measures will be followed.
The need for ongoing education is essential as more data becomes available both on disease and on ways of protection against it. Staying informed of official recommendations for care of the patient require frequent and continuous updates for staff. Nashwan et al also suggested some remunerative models for nurses based on knowledge and attitude. 56
Another important aspect to consider is the workplace atmosphere. Evidence shows that communications are highly correlated with mental health; and the resilience of a team may be more related to the bonds between team members than the coping style of any individual. Peer relationships with colleagues provide opportunities for staff to talk about their experience to enhance support and social cohesion. These sessions should not involve anyone being forced to talk about his or her thoughts or feelings. These sessions should be provided during a staff member’s shift (not afterward) so as not to encroach on rest and recovery time. These findings are supported by those of the other studies during Ebola 57 and MERS outbreaks. 58
The social stigma was another theme, which is in line with the MERS-COV outbreak, indicating that both stigma and hardiness exert direct effects on the nurses’ mental health. 59 It is suggested that the nurses’ experiences in these epidemics are to be transferred to a section of nursing textbooks and taught in nursing schools. These experiences can provide an acceptable guideline for nurses all around the world to deal with the epidemics more effectively as it is also a valuable experience for nursing and hospital managers. Further training of psychological skills among medical staff is also recommended. 38
Finally, recent studies include that increasing nurses’ knowledge about pandemics, paying attention to their financial benefits, and especially focusing on their perceived value are the most important willingness strategies in COVID-19 pandemic. 60
These implications were not intended to be an exhaustive list of recommendations but are intended to inform planners, managers, and leaders that are likely to be helpful in supporting staff during the COVID-19 pandemic.
Limitations
Since the purpose of this review was to understand findings and trends in the published literature, the major limitation of the study is that gray literature was not reviewed, whereas gray literature covers a wide array of information relevant to a willingness to work such as policy, action plans, and reports. Second, the search was limited to those published papers in the English language. Third, the search was done in three main databases; thus, it is possible that some studies were lost if they were indexed exception PubMed, Scopus, and WOS. Finally, these interventions are quite various in different organizational cultures in different regions and countries, and because of time and source limitations, these cultural differences were not considered in this study.
Conclusion
The studies included in this review show a wide range of approaches on how to address intervention improve willingness to work in conditions like a disaster. While most respondents reported their willingness to work during this pandemic, it is anticipated that as the severity of an event increases, willingness and ability to work will decrease. This study demonstrated a distinct decrease in the willingness to work as PPE available for workforce diminished and when they considered their immediate family at risk of illness or death. The findings revealed a strong perception that the “Battle Buddy” system should be implemented to increase the resilience of frontline workers. This research also demonstrated the important role that the safety of a worker’s family plays in the HCWs’ willingness and performance. Managers can potentially increase the commitment and likelihood of HCWs caring for patients through interventions focusing on maintaining the safety of both the employees and their families. If organizations were to implement these strategies and interventions, they should let the staff know these decisions and as a necessary step in every organizational intervention remember to evaluate the impacts.
Footnotes
Acknowledgments
We acknowledge the support and cooperation received from the gifted and talented student center in Iran University and Medical Sciences. We also acknowledge the anonymous reviewers for their deep and thorough review which led to a much-improved version of the paper.
Author Contributions
NKD, AFA, MRL, SS, and SG had the main idea for the study.
All authors devised the search strategy and eligibility criteria.
SS conducted the database search strategies, MRL, AFA, and NKD conducted the exclusion of studies and the eligibility assessment of the full-text articles, extracted data and drafted the synthesis of results.
AFA and NKD drafted the initial study, and SG provided critical revision of study.
All authors approved the final study.
Declaration of Conflicting Interests
The authors declare that they have no competing interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article