
Abstract
Background: This study was designed to investigate whether psychological status is associated with upper-extremity health status in an elderly general population. Methods: Using Quick Disabilities of the Arm, Shoulder, and Hand of the Japanese Society for Surgery of the Hand (QuickDASH-JSSH), we evaluated 200 Japanese elderly people (76 men, 124 women; mean age, 71.6 years, 60-98 years) to assess their upper-extremity-specific health status. Each had completed a self-administered questionnaire including gender and dominant hand items. As an indicator of hand muscle function, we measured their bilateral hand grip. Study participants were assessed for depressive symptoms using the Geriatric Depression Scale Short-Japanese Version (GDS-S-J). Statistical analyses were applied to clarify associations between self-assessed upper-extremity dysfunction and screening results for depressive symptoms in an elderly general population. Results: Those reporting no complaint of an upper extremity were 72 (36 men and 36 women) (36.0%). The GDS-J score was found to have significant positive correlation with age (r = 0.20, P= 0.0045) and the QuickDASH score (r = 0.25, P = 0.0004). The GDS-J score was found to have significant negative correlation with dominant grip (r = −0.15, P = 0.04) and non-dominant grip strength (r = −0.21, P = 0.004). For all participants, multiple regression analysis revealed the QuickDASH score as associated with the GDS-J score. Conclusion: Self-administered upper-extremity health condition as assessed using QuickDASH is correlated with depressive symptoms in elderly people. Objective pathophysiology and subjective illness behavior must be identified in daily clinical practice. A biopsychosocial approach must be used when advising and treating patients.
• ○ Scores of patient-reported outcome measurements in patients with specific upper disorders are correlated with depression symptoms. • ○ This report describes depressive conditions and the self-assessed upper-extremity health status of people in an elderly general population. • ○ When advising patients in clinical daily practice, one should recognize biopsychosocial factors affecting the patient’s mental health condition.
Introduction
Psychological factors affect patient expressions and their pain and disability complaints. Depressive disorders are especially common among patients with chronic pain such as back pain and headaches.1,2 Depression is known to amplify the expression and perception of pain. 3 Patients who have depressive symptoms or who have less-effective coping with their illness might have diminished capability for adaptation to painful difficulties. 4 An earlier study of patients with specific upper disorders investigated a relation between upper-extremity health status and psychological factors. Results indicated correlation between depression and pain anxiety symptoms and scores of patient-reported outcome measurements for the upper extremities. 4 Osteoarthritis, a common degenerative musculoskeletal disorder, causes joint pain. Various inflammatory cytokines such as interleukins (ILs) and tumor necrosis factor-alpha (TNF-α) influence the etiology of OA. 5 Reportedly, depression is associated with a chronic, low-grade inflammatory response. Cytokines have been found to induce depressive symptoms. 6 Some relation might exist between depression and the degenerative musculoskeletal disorder. Several studies have assessed the association between the psychological features and upper-extremity health conditions among a patient population.4,7 Nevertheless, few reports have described these relations among the general population. In daily clinical practice, hand surgeons must understand interactions between the health condition of upper extremities and the underlying psychological status of patients. In Japan, the share of elderly people (aged ≥65 years) among the general population is expected to exceed 30% in 2025 and to reach 39.9% in 2060. 8 Given increasing trends of general population aging in Japan, we expect to be increasingly likely to see elderly patients in daily clinical practice.
Grip strength measurement is a simple and inexpensive method used as a reliable index for whole body muscle strength, but not for functional integrity of the forearm and hand. 9 Earlier studies have demonstrated a significant association between grip strength and mental health condition, such as depressive and anxiety status.10–14 Lower handgrip strength was associated with depressive symptoms in both cross-sectional and longitudinal analyses.10,12,13 In order, adults, malnutrition, social isolation, and poor overall physical activity were reported as factors that interact with grip strength and depression.15,16 Furthermore, some common pathophysiological pathways mediated by oxidative stress, chronic inflammation, metabolic dysfunction, and decreased concentration of brain-derived neurotropic factors share contributing to the statuses of depression and dynapenia. 17
This study investigated the relation between upper-extremity-specific health status and psychological factors in an elderly general population. We hypothesized that the self-assessed health status of upper extremities is associated with depressive conditions in an elderly general population.
Material and Methods
Local medical examinations intended for the early detection of cancer and for the prevention of lifestyle-related diseases are conducted regularly for residents of a mountain village in Japan, where agroforestry and tourism are the main industries (total population 4573 in 2017, comprising 2230 men and 2343 women). In 2017, 946 people (436 men and 510 women) underwent medical examinations of their own will. From these 946 residents, 200 people (76 men and 124 women; average 71.6 years of age, range 60–98) participated voluntarily in the orthopedic examinations reported for this study. Each had completed a self-administered questionnaire with items related to gender and the dominant hand.
QuickDASH Assessment
The QuickDASH-JSSH is an 11-item questionnaire that measures arm-specific disability. The Japanese version of DASH (DASH-JSSH) was adopted cross-culturally and was developed to produce QuickDASH-JSSH by extracting 11 of 30 items of DASH-JSSH related to disability and symptoms. After Imaeda et al. 18 evaluated the reliability, validity, and responsiveness of QuickDASH-JSSH, they reported that QuickDASH-JSSH has equivalent evaluation capacity to that of the original QuickDASH. That evaluation was used because the elderly participants in our study were expected to have an increased burden imposed by increasing questionnaire length.
Short Geriatric Depression Scale Assessment
Depressive symptoms were measured using the 15-item Short Geriatric Depression Scale.19–22 The diagnostic accuracy of the GDS-short and the original version demonstrated that the accuracy of both versions of GDS is similar to that of the CES-D for diagnosing depression. 19 We assessed psychological functions using the 15-item Short Geriatric Depression Scale-Japanese version (GDS-J), for which scores 0–5 indicate no depression, 6–8 show mild depression, 9–11 show moderate depression, and 12–15 show severe depression.19–22 Yoshitomi evaluated their validity and reliability for a Japanese elderly population. 23 On this scale, a score of 6 or higher might be indicative of depressive status. 24 All items in GDS are rated by self-report as 0 or 1, where 0 represents yes and 1 represents no. Item scores are summed, yielding a possible total score of 0–15. Higher scores signify a severe depressive condition. Participants with >1 missing item were excluded from analyses.
Grip Strength Measurements
A digital dynamometer (Takei Scientific Instruments Co Ltd, Tokyo, Japan) was used to measure grip strength. Grip testing was conducted using the standardized position recommended by the American Society of Hand Therapists. Participants were seated with the shoulder in adduction and neutral rotation, elbow flexed at 90°, forearm in a neutral position, and the wrist between 0° and 30° of extension and 0° and 15° of ulnar deviation.
Statistical Analysis
We compared age, height, weight, BMI, gender difference, dominant, and non-dominant grip strength, and the QuickDASH score among participants in the degree of GDS-J-score. The Spearman rank correlation coefficient was used to elucidate the relation between age, anthropometric variables, dominant, and non-dominant grip strength, the GDS-J score, and the QuickDASH score. Correlation was categorized as slight (r = 0.10–0.29), medium (r = 0.30–0.49), or large (r = 0.50–1.00). 25 Multiple regression analysis was used to identify the association of GDS-J score using several factors as explanatory variables: gender, age, height, weight, grip strength of the bilateral side, and the QuickDASH score. Data are presented as means and standard deviations (SDs). A P value of <0.05 was inferred as statistically significant. This study was approved by the regional ethics board. Informed consent was obtained from all participants.
Results
Characteristics of Participants According to Age Cluster.

Mean values are shown with the standard deviation.
SD: standard deviation.
aSignificantly different (P < 0.05) from values of the 60s age group.
bSignificantly different (P < 0.05) from values of the 70s age group.
Results of Correlation Between Clinical Findings for Participants.

Values are means (SD).
Significant P < 0.05.
Significant P < 0.01.
Characteristics of Participants in the Degree of GDS-J Score.

Values are means (SD).
Significantly different (P < 0.05) from values of the GDS score 0-5 group.
Multiple Regression Analysis of Factors Associated with the GDS Score.
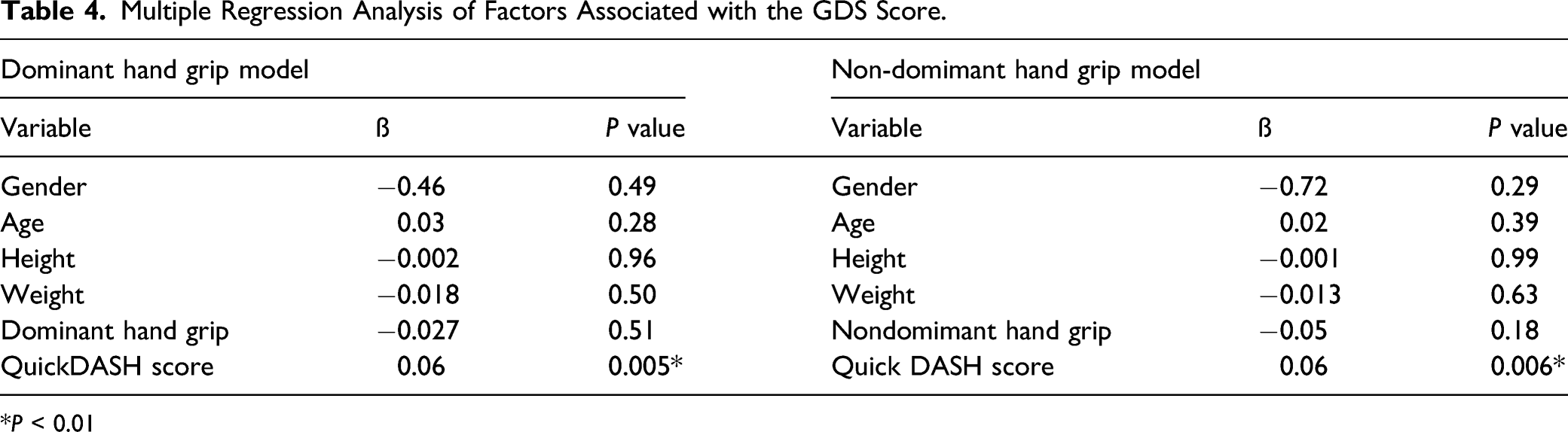
P < 0.01
Discussion
One distinguishing characteristic of our study is our evaluation of the relation between upper-extremity health status and depressive symptoms in an elderly general population. Earlier reports have described correlation between the total DASH or QuickDASH score and psychological factors in patients with specific diseases of upper extremities.4,26–28 Ring et al. 4 reported the degree of depression as an independent predictor of the total DASH score in 235 patients with common and self-limiting hand function impairment (mean 52 years old, range 21–86 years). They advocated attempts to improve doctors’ capabilities for identifying objective and physical problem of patients and of interpreting psychological factors that keep patients from coping with self-limiting problems. However, a chronic pain condition can contribute to the prolongation of depressive symptoms. 29 Furthermore, earlier studies demonstrated an association between pro-inflammatory cytokines and depression. 6 Increased pro-inflammatory cytokines such as IL-1β, IL-6, tumor necrosis TNF-α, and interferon-γ might play important roles in the pathophysiology of depression. 30 Tatebe et al. measured the inflammatory cytokines of 38 patients with chronic conditions of the wrist who had undergone arthroscopy. They particularly assessed the association with cytokine and chemokine levels in the synovial fluid and synovial membranes and patient-rated evaluations of pain, function, and depression. Their results revealed positive correlation among concentrations of TNF-α, depression, and chronic conditions of the wrist. 31 Our data indicate that participants who scored ≥9 on the GDS-J questionnaire had significantly higher scores than those who scored <6 on QuickDASH (P= 0.04). Multiple regression analysis revealed the QuickDASH score as associated with the GDS-J score for all participants. Physicians need some ability to identify physical factors objectively and need to enhance quality of life through intervention to alleviate upper-extremity difficulties of elderly patients.
Handgrip strength assessment has been used as a reliable index for whole body muscle strength, but not for upper-extremity muscle strength and function. 9 Earlier studies have demonstrated that grip strength is inversely related with incident depression and have suggested the importance of maintaining grip strength in later life, with greater benefits for depression in a general population. Those studies have implicated handgrip strength as a predictor of depressive symptoms.10,12,13 Depression and lower grip strength share interaction factors such as malnutrition and decline in systemic physical functioning and social isolation.15,16 This status might support the conjecture that the association between lower grip strength and depressive symptoms is bidirectional. However, other distinguishing characteristics of our study have demonstrated that grip strength is not associated significantly with the GDS-J score in multiple regression analysis. As the cause that led to our results, it might be true that the subjects of this survey were originally a group with high interest in their own health, and it might be a group with few factors that interact with lower grip strength and depression. Additional studies must be undertaken to elucidate associations between pathological conditions such as pain and disability of the upper extremities and lower grip strength and depression.
Our study demonstrated that GDS-J scores have correlation with age (r =0.20, P = .0045) and QuickDASH scores (r = 0.23, P = 0.0004). Age, upper-extremity disability, and depressive symptoms might be influential as confounding variables in our study. Aasheim and Finsen 32 reported for a general population in Norway that mean QuickDASH scores for women and men rose with increased age. However, it has been reported that no statistical significant association exists between age and depression. Moreover, it has been proposed that vulnerability to mood disorders, early life adversity, social stress, harmful lifestyle, comorbid disease, and intermediate health hazards might facilitate the expression of depression during the lifespan in review. 33 Our study demonstrated that participants having no complaint related to upper extremities were 36.0%. However, upper-extremity symptoms might occur naturally among elderly people. People might have upper-extremity symptoms and might be adaptive to their symptoms. It might be difficult to adapt to their symptoms during times of diminishing mental capacity.
Several limitations of this study must be described. First, our study was conducted using a cross-sectional design, which might not provide definitive information about cause-and-effect relations. A prospective longitudinal study should be undertaken to investigate relations between changes in upper-extremity health status and psychological factors in a large general population. Second, the use of different self-administered questionnaires to assess depression might engender overestimation or underestimation of depressive symptom responses. Another psychosocial assessment tool might affect results related to depression status. Third, we did not assess other related factors for depressive symptoms such as Japanese cultural factors, education level, socioeconomic status, or other organ-related complaints. 13 Fourth, we were unable to investigate whether treatment of upper-extremity disease can improve psychosocial symptoms in elderly people. Further investigation might provide additional results related with upper-extremity health status and psychological factors in a prospective study.
In conclusion, the present study has demonstrated the self-assessed health status of upper extremities as associated with depressive symptoms in an elderly general population. Physicians should recognize that biopsychosocial factors are affected by mental health condition when facing patients in clinical daily practice.
Footnotes
Acknowledgments
The authors thank the participants, medical staff, and public health nurses of the regional health center for their assistance with and support of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.