
Abstract
Coverage of anesthetic and surgical capacities is still a neglected global health measure, although disparities in provision of safe surgical and anesthetic care are obvious in low- and middle-income countries. This is the first comprehensive assessment of anesthesia health system capacity in Pakistan. Results exposed a crucial deficiency of critical supplies and workforce for providing safe anesthesia and, hence, safe surgery, emphasizing the need for strengthening workforce.What do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications Towards Theory, Practice, or Policy?
Introduction
Effective surgical procedures can only be attained with access to standard anesthesia services. Unfortunately, anesthesia is often considered a necessity only at secondary- and tertiary-level medical facilities. 1 However, coverage of anesthetic and surgical capacities is still a neglected global health measure, although disparities in provision of safe surgical and anesthetic care are obvious in low- and middle-income countries (LMICs). 1 Feeble efforts in improving health care provision and sheer neglect of improvements in anesthesia health systems has deprived the access of five billion people globally to safe and affordable anesthesia.2,3 In high-income countries, safety of anesthesia has improved gradually over time—not only through improvements in training, provision of medications, and technological developments, but also with the progression in minimum standards for safe practices, updated guidelines, and checklists. 4 Comparable advancements have not been achieved in low-income settings with poor infrastructure and deficiencies of anesthesia workforce along with lack of essential equipment medication and supplies. Therefore, they are incapable of following the existing standards of high-income regions.5,6 It is estimated that at least 143 million added procedures annually are essentially required to decrease disability and death in LMICs from surgical diseases. 7 Although recommendations describing minimum standards for safe anesthesia practice exist, the number of hospitals fulfilling these standards is not known.
To overcome this issue, the Lancet Commission on Global Surgery recommended at least 20 surgical, anesthetic, and obstetric physicians per 100,000 population by 2030 2 and 5000 surgical procedures for a population of 100,000. The World Federation of Societies of Anaesthesiologists (WFSA) has developed criteria for safe practice of anesthesia on behalf of 150 countries. There recommendations have been endorsed by World Health Organization (WHO), and these standards are appropriate for anesthesia workforce globally. WFSA envisioned providing supervision and support not only to anesthesia providers, but also their proficient organizations, surgery providing hospital, health facility superintendents, and governments for escalating and improving the quality and safety of anesthesia throughout the world.7,8
These recommendations are also important for a country such as Pakistan, which belongs to the lowermost quartile of the Human Development Index.9,10 Within Pakistan, Punjab is the most populated province 11 with almost 3000 public level health facilities providing profoundly subsidized services to the public. Among these health facilities, only Tehsil Head Quarters (THQ), District Head Quarters (DHQ), and teaching hospitals provide anesthesia and major surgical facilities. In Punjab, there are a total of 88 THQ hospitals, 34 DHQ hospitals, and 23 teaching hospitals providing anesthesia and surgical care. 12
Currently, there is no detailed information about anesthesia health system capacity in Pakistan available. Such comprehensive data about health system capacity is an essential requirement as it could provide an insight into the system’s needs at administrative level. This study targets to develop a first detailed assessment of anesthesia capacity in public level hospitals of Punjab which can support the government in improving health facilities.
Methods
Study Design and Sample
This cross-sectional study includes a comprehensive survey of public level hospitals of Punjab Pakistan which are providing surgical services. We used Yamane’s formula to calculate the sample size for smaller populations for selecting the number of hospitals

Data Collection
Permissions for data collection was sought from the heads of each hospital. We collected data through paper-pencil–based approach between October 2020 and February 2021. In most secondary level hospitals, the head of the anesthesia department serves as the head of the operating room. Therefore, they were able to respond to each survey question easily, whereas in tertiary level hospitals, where every department has its own operating room, senior registrars of the anesthesia department were approached who gave answers after consulting with equipment and drug in charge of hospitals. We omitted four facilities from the study, because they did not have any anesthesia team of their own.
We used the Anaesthesia Facility Assessment Tool (AFAT) 13 for data collection. This tool addresses essential recommendations highlighted by WFSA and WHO in order to conduct safe anesthesia practices. It was established to evaluate anesthesia capacity on national level as well as individual capability of hospitals to meet international standards. 7 Although AFAT resembles numerous previously developed surgical and anesthesia capacity assessment tools,14–16 it is precisely focused on anesthesia resources. 17 Every hospital was assessed on the basis of capacity in terms of infrastructure, workforce, information management, surgical interventions, medications, and equipment. The questions posed to study participants are visible in the tables of the results section. A 6-point Likert scale was used to assess the capacity situation as per WFSA recommendations. The availability in hospitals are presented by frequency and percentage as “always” (100%) or “almost always” (76%–99%), “often” (51%–75%), “sometimes” (26%–50%), “rarely” (1%–25%), and “never” (0%).
Data Analysis
The collected data was transferred using SPSS Version 25. Descriptive statistics were calculated for the survey questions; categorical and continuous variables were reported in absolute numbers and percentages.
Ethical Concerns
The study is part of the doctoral dissertation of the first author. The ethical approval for this study was obtained from the Advance Study Research Board, University of the Punjab (1456/Acad.; February 22, 2020) and Departmental Doctoral Program Committee (D/588/ISCS; June 23, 2020), Department of Public Health, University of the Punjab.
RESULT
This study collected data among 106 public level health facility across Punjab that provided surgical care in 2020/21. The sample consists of 63 THQ, 25 DHQ, and 18 tertiary level teaching hospitals. Anesthesiologists from the surveyed hospitals consist of 66% specialist physicians and 34% non-specialist physicians. Overall, 12.3% said they had less than one year of experience of working at current facility, half of them (51.9%) had working experience of 1–3 years at the current facility, and 35.8% had experience of more than 3 years.
Infrastructure
Characteristics of the Hospitals (n = 106).

Infrastructure (n = 106).

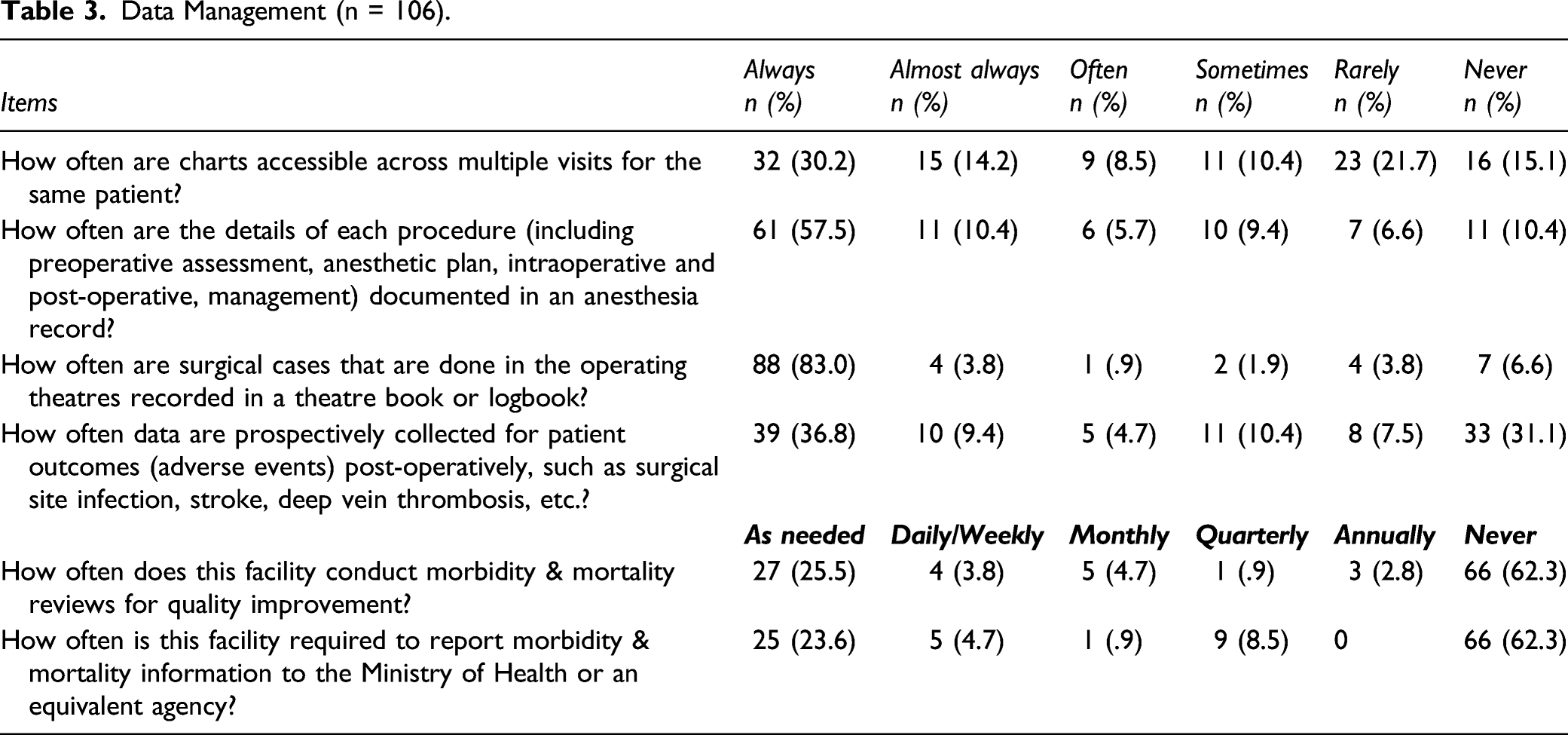
Data Management
Half of the hospitals keep records in paper form (50%, n = 53), 10.4% (n = 11) in electronic form, and 30.2% (n = 32) both in paper and electronic form. However, 9.4% (n = 10) keep their records neither in paper nor in electronic form.
Data Management (n = 106).
Surgical, Anesthesiology and Obstetric Workforce
Surgical, Anesthesiology, and Obstetric Workforce (n = 106).

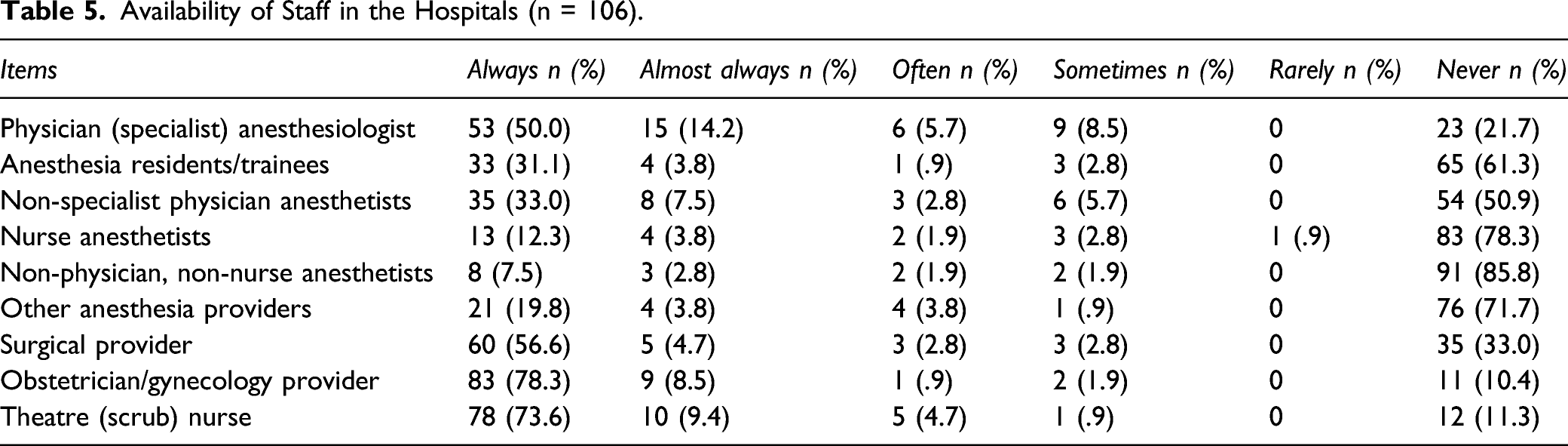
Workforce Availability
Availability of Staff in the Hospitals (n = 106).
Surgical Interventions
Response of Hospital Logbook Regarding Number of Surgical Cases (n = 106).

Surgical Interventions Offered by the Hospitals (n = 106).

Availability of Anesthesia-Related Medication
Most of essential medication, proven on WHO-WFSA standards
Availability of Anesthesia-Related Equipment
Furthermore, 46.2% (n = 49) had 0–1 anesthesia machine, 20.8% (n = 22) had 2–3 machines, 12.3% (n = 13) had 4–5 machines, and 20.8% (n = 22) had more than 5 machines at their facility. In regard to mechanical ventilators, 53.8% (n = 57) of hospitals had 0–1 machine, 16.0% (n = 17) had 2–3 machines, 14.2% (n = 15) had 4–5 machines, and 16% (n = 17) had more than 5 mechanical ventilators at their facility.
A detailed overview on further equipment’s availability is provided in Supplementary Table 2. Some equipment is available at all hospitals at all times. However, for example, defibrillator, self-inflating breathing bag/mask, manual or electric suction pump, stethoscope, and thermometer are always available only at 80–90% of hospitals. Furthermore, functioning X-ray machines (34.9%, n = 37) and functioning ultrasound machines (19.8%, n = 20), blood gas analyzers (16.0%, n = 17), continuous waveform capnography (17.9%, n = 19) and spot check capnography (15.1%, n = 16), as well as hemoglobin measurement devices (15.1%, n = 16) are seldomly always available.
More than half of the respondents (56.5%, n = 60) reported that non-functioning equipment cannot be repaired onsite by staff at the facility. However, there is also a large fraction (37.7%, n = 40) which cleans and re-uses disposable equipment (e.g., endotracheal tubes or laryngeal airway mask) (Supplementary Table 2).
Discussion
This research defines existing anesthesia capacities of Punjab, Pakistan—the province with highest population and considered advance in terms of health and education facilities. The areas with leading concern were recognized in terms of workforce insufficiencies, basic anesthetic infrastructure deficiencies, as well as medications and lack of equipment.
This study found that the majority of hospitals across Punjab reported uninterrupted oxygen, electricity, and running water supply, which is considered as minimum standards for safe provision of surgical and anesthetic care among hospitals. 7 However, there are also other countries, which do by far not meet the standards, such as Afghanistan, where only 40% of hospitals have access to running water 18 and Gambia with 50% permanent availability of water. 19 Almost one third of the public hospitals in Punjab have a single operation theatre (mainly in THQs), which roughly makes one operating theatre per 250,000 population. This is far from international standard of two operating theatres per 100,000 population.20,21 Likewise, a deficiency of proper PACU and ICU was also identified. Previously, there has been data scarcity on post-operative anesthesia care, pain management, and critical care services in low-income countries of South Asia.1,22 Though, a study from Africa found that the majority of post-operative deaths occurred in anesthesia recovery rooms and ICUs, thus putting a light on the significance of standardized perioperative infrastructure. 23
As for workforce WFSA recommends, a minimum of five consultant anesthesiologist for a population of 100,000 is needed. 24 In Punjab, unfortunately along with non-specialist physician anesthetists, anesthesia trainees, and non-physician anesthesia providers, the workforce density is almost one per 100,000 people, which is more than in neighboring countries like Bangladesh (.58 per 100,000 population) and Afghanistan (9 anesthetist in total), but slightly less than India (1.27 per 100,000 population).24,25 This deficiency of anesthesia workforce is substantial, as it results in decreased surgical capacities, along with poor surgical outcomes.26,27 According to our study, the problem is more evident in rural areas of Punjab, where the maldistribution of anesthesia workforce is more distinct. This is also evident in neighboring countries.18,23–25 In addition, SAO density is also extremely lower than the value of 20 per 100,000 population recommended by the Lancet Commission on Global Surgery. 2 Most of the hospitals (mainly THQs) have a SAO density of 5 per facility which is serving a population of more or less 1,000,000, where there is one anesthetist mostly, one or no surgeon, along with three or more gynecologists. Although for serious and extensive cases, DHQ or teaching hospitals are available, having a saturation of surgeons, gynecologists, and anesthetists; this startling inconsistency between secondary- and tertiary-level hospitals greatly affects surgical outcomes and increases morbidity and mortality ratios. 28 However, the condition is still better than in other LMICs, like in Sierra Leone, only 10 surgeons are available for a population of 5.7 million, and in Afghanistan, only 9 anesthetists for a population of 32 million, 27 in Uganda for a population of 27 million, and 8 in Bhutan. Moreover, 30% of hospitals in Afghanistan do not have a gynecologist.24,28,29
This study found that more than 90% of the public hospitals in Punjab have at least one anesthetist. Although this is insufficient, the situation is still better than in many other LMICs. 30 On the other hand, this study indicates maldistribution of anesthesia providers in addition to insufficiency, with THQ hospitals suffering the worst. There is a dire need for provision of incentives to upscale the anesthesia workforce at THQ and DHQ. Non-physician anesthesia providers (anesthesia technologists) are also seen in few DHQs and THQs, which share a substantial burden of the anesthesia provision in densely populated areas like other LMICs.1,22,24 Government-controlled efforts are required to improve opportunities for anesthesia technologists and nurse anesthetist training to overcome the service provision gap in THQ hospitals, particularly in southern Punjab.
Under the domain of surgical interventions, the condition for gynecological interventions seems satisfactory, as 93% of hospitals across Punjab provide caesarean facilities and the remaining still offer normal vaginal deliveries, unlike many African and Asian countries (i.e., Gambia, Tanzania, and Afghanistan) where almost half of the hospitals do not provide these facilities. 31
While discussing the supply of medications in hospitals of Punjab, it was robust as compared to other provinces and many other LMICs.1,21 Though insufficiencies are still present, especially at THQ and DHQ, where anesthesia-related drugs are unavailable. Fortunately, most of intraoperative monitoring standards were fulfilled by the majority of health facilities in Punjab. For example, pulse oximetry was described as always available in 99% of hospitals which is quite better when compared to outcomes of multiple other global surveys LMICs.1,22,31 However, capnography was scarce, even after availability at many facilities, but showing maintenance issues. Its availability was not relatable with the location or size of hospital. Moreover, defibrillators in operating theatres was non-existent at many Tehsil level hospitals. Overcoming this gap is immediately required in order to improve the safety of patients.
Limitations
Regardless of being the first most extensive anesthesia capacity assessment in Pakistan, our study still has numerous limitations. First of all, it just covers a province of Punjab, whereas it is required all over the country to get a real picture of available resources. Secondly, it did not cover private, non-profit, social security, or military hospitals. Moreover, this data was reported by heads of anesthesia departments or senior registrars at each hospital instead of autonomous observers. This may lead to biases, but can also offer a useful way where hospitals can respond to the tool themselves. Finally, only quantitative tools might not completely apprehend the actual cause behind surrounding resource insufficiency. Therefore, qualitative analyses are needed to better apprehend the origins of anticipated problems and suggest solutions.
Conclusion
This is the first ever province wide, comprehensive evaluation of anesthesia capacities in public hospitals of Punjab, Pakistan, which reveals key insufficiencies in terms of workforce, infrastructure, medicines, and equipment. This study brings into notice the fragile condition of public level hospitals in Punjab, where the majority of hospitals meet only a few WHO-WFSA criteria. There is a critical deficiency of anesthesiologists (both physician and non-physician) including other SAO providers. This study reveals that dedicated investments in terms of escalating anesthesia workforce and accessibility to anesthetic/pain managing medications and equipment would not only improve surgical outcomes but also patient satisfaction in addition to decreasing surgical disease burden. This assessment undoubtfully provides ground level data to reform policies for guaranteeing the accessibility of vital resources and makes a base for improving upcoming service delivery regimen for provision of safe anesthetic and surgical care in Pakistan.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580211059740 – Supplemental Material for Anesthesia Health System Capacities in Public Hospitals of Punjab, Pakistan
Supplemental Material, sj-pdf-1-inq-10.1177_00469580211059740 for Anesthesia Health System Capacities in Public Hospitals of Punjab, Pakistan by Sumbal Shahbaz, Rubeena Zakar and Florian Fischer in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author’s Contributions
Sumbal Shabaz and Rubeena Zakar conceptualized the study. Data collection and analysis was performed by Sumbal Shabaz and supervised by Rubeena Zakar and Florian Fischer. The first draft of the manuscript was written by Sumbal Shabaz; and Rubeena Zakar and Florian Fischer revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval for this study was obtained from the Advance Study Research Board, University of the Punjab (1456/Acad.; February 22, 2020) and Departmental Doctoral Program Committee (D/588/ISCS; June 23, 2020), Department of Public Health, University of the Punjab.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.