
Abstract
Keywords
Highlights
There is a lack of research on COVID-19 mortality among older adults. Furthermore, the lack of knowledge about the relationship between nutritional status and COVID-19 mortality among older persons makes the study extremely relevant in the current situation. The majority of the COVID-19 deaths were among older people. However, due to its well-designed nutritional and care policies, Kerala was the only state able to successfully reduce COVID-19 mortality among older persons. Because of the limited research available on COVID-19 mortality among the older adults, the current study aims to prove that proper nutrition can help to prevent it. The present study will aid in the formulation of policies regarding the nutritional status of the older persons in the future, allowing them to live a longer and healthier life.What Do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What are Your Research’s Implications Towards Theory, Practice, or Policy?
Introduction
Older adults are at the highest risk of COVID-19 mortality and thereby demographically the most affected group worldwide. This is due to social exclusion and restrictions on certain rights, such as those which result from the imposition of quarantine or isolation that limit freedom of movement intending to contain the spread of the virus. It is due to the same reason that this category of the population faces a challenge and fear of illness and death in the wake of the COVID-19 pandemic. 1 Both population density 2 and the age profile of the population3,4 have been flagged as factors in the pandemic. Older adults have been medically identified as more susceptible to death. According to a meta-analysis of COVID-19 positive patients up to May 7, 2020, from China, Italy, Spain, the United Kingdom, and New York State, more than 23% of the subjects were aged 80 years and above. 4 The lowest per cent of octogenarians (90+ years) affected was in China, and the highest was in the U.K. and New York State.
Kerala’s public health authorities have long been mindful of the state’s susceptibility to global epidemics. This comparatively high uncertainty is attributed to the high degree of engagement with the global economy, the huge non-resident community residing in many parts of the world, 5 and the state economy’s dependence on domestic and international tourism. The Nipah virus epidemic in 2018 was one such incident that raised awareness of such a threat. Since then, Kerala has adopted a surveillance mechanism to aggressively search for emerging pathogens that may affect the state’s health. Kerala became alert as soon as the COVID-19 pandemic broke out in China and released appropriate guidelines like the ‘Break the Chain’ campaign. Through an active strategy of quarantining susceptible cases, testing all high-risk contacts and, if found positive, tracing their contacts and keeping them isolated, Kerala achieved low transmission rates initially, thereby increasing the rates of recovery among existing COVID-19 cases. Though positive cases were originally isolated in healthcare institutions, home-based isolation and management were introduced later in the state due to the increasing number of cases. Presently, symptomatic persons (except the mild ones) and high-risk positive cases (older adults, those with co-morbidities) are isolated and managed institutionally. Also, high recovery rates were achieved because of proactive management of cases with strict management guidelines in healthcare institutions wherever indicated. The rapid expansion of healthcare infrastructure to manage COVID-19 was also an important reason.
Being the Indian state with the highest number of older persons,6,7 Kerala was expected to have the maximum number of COVID-19 deaths as they were at the greatest risk of serious infection and death if infected. But strikingly, according to the Ministry of Health and Family Welfare, the state performed better than the nation and became a global example in containing the virus with the best recovery statistics (around 94.4% recovered and .4% died, which is less than the national average (1.5%) during the first wave. Though the primary reason for Kerala’s low case fatality is early diagnosis, isolation and comprehensive management, the current article tries to prove that nutrition played a significant role in bringing down COVID-19 deaths among older adults in Kerala during the first wave.
Conceptual Framework
The risk of survival or death among the older population arising from the COVID-19 virus is primarily determined by three major underlying causes, household access to quality food, health and hygiene, and the treatment/care habits practised by the household where an older person lives. But the immediate causes are individual food intake and health status or other underlying diseases. The combined effect of these variables influences individual food consumption and their health status (Figure 1). Also, the interplay between these variables determines the nutritional state of older adults, which regulates their survival, recovery or mortality from the virus. The conceptual framework used in the article is an adaptation of the UNICEF Conceptual Framework for the cause of malnutrition.
8
Conceptual framework of nutrition and COVID-19 mortality and survival among older persons. Source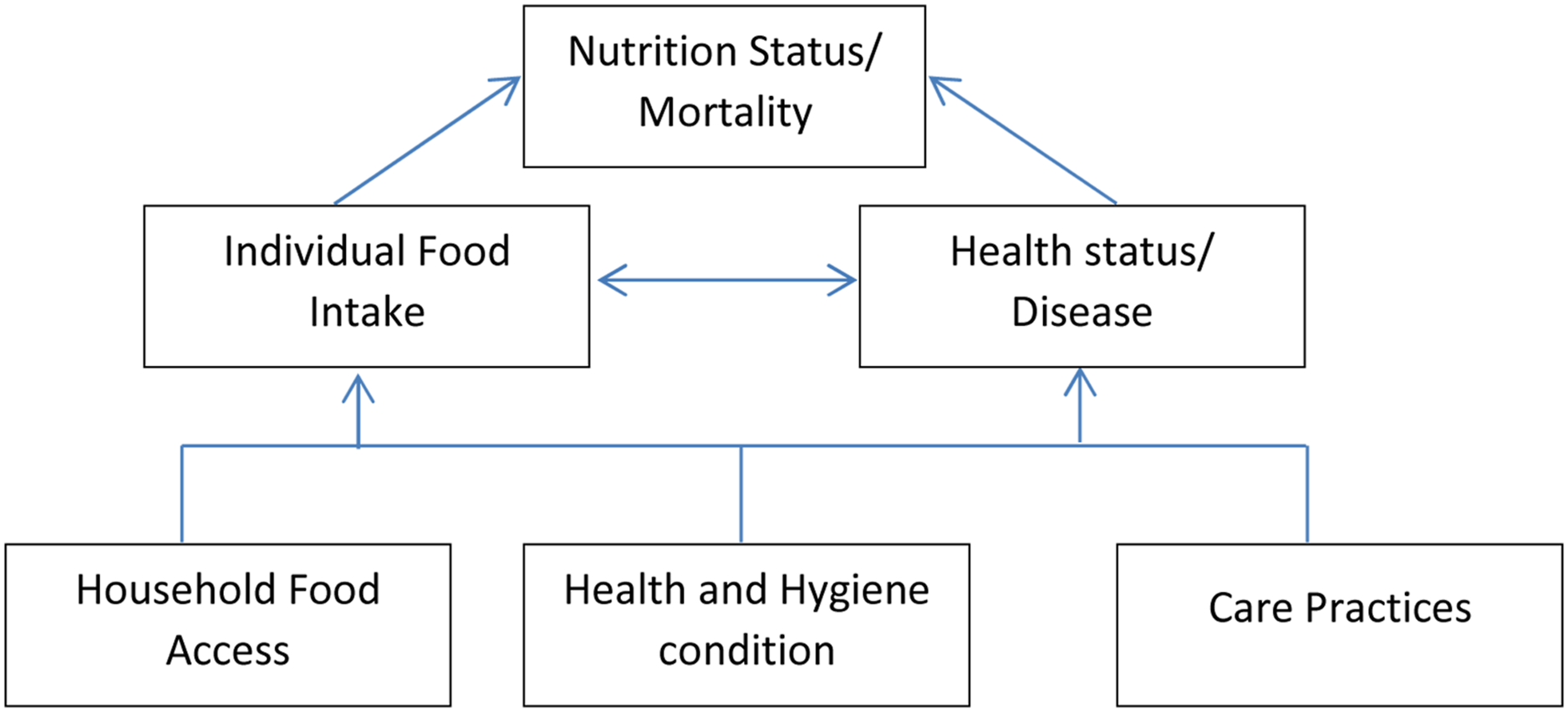
Material and Methods
Data
The paper analyses the Kerala Ageing Survey (conducted by the Centre for Development Studies over the last 15 years in Kerala) to study the pre-COVID nutritional level of older persons in Kerala. The survey covered a total of 4940 older persons in 2004 and continued as a longitudinal survey repeated every three years and has completed its 6th iteration in 2019. 6 The study uses data from 2004 as the baseline, while data from 2019 is considered a follow-up. The sample size covered in 2004 was 4940 older adults. However, in 2019, a gradual decrease in the number of people throughout the survey was noted, 988 adult persons were alive, and 238 adult persons had died in 2019. Individuals who were not interviewed, or those with missing data, were excluded. The paper also incorporates data on COVID-19 cases from the Government of Kerala dashboard 9 and the Directorate Health Services (DHS) website 10 Government of India, 11 Ministry of Health and Family Welfare, 2020 and the world data were taken from Global Change Data Lab. website 12
Measures
Methods
Cox hazard regression was used to analyse the effect of nutritional status on all-cause mortality, and logistic regression analysis was performed to assess the association between nutritional indicator BMI and incidence of co-morbidity condition among older adults in Kerala.
Preliminary Case Fatality Rate (CFR) for the period March 2020 to February 2021 were computed using the formula, CFR = (Number of COVID-19 death/Number of confirmed cases) * 100
In addition, to understand the role of nutritional status in averting infection and death of older persons amidst the COVID-19 pandemic, specific case studies were done with health professionals, ASHA (Accredited Social Health Activist workers), Kudumbashree members, COVID-19 survivors and family members of the deceased.
Results
Nutrition History of Older Adults in Kerala: Pre-COVID-19 Scenario
Nutritional level of the older persons in Kerala, KAS 2004-2019.

Source: Special Tabulations from Kerala Ageing Survey 2004–2019, co-ordinated by the first author.
Effect of Nutritional Risk Factors on All-Cause Mortality
Results from the Cox regression analysis showing the hazard ratio from Kerala Ageing Survey 2004–2019.

Source: Special Analysis from Kerala ageing survey 2004–2019, co-ordinated by the first author.
COVID-19 Pandemic
COVID-19 crisis had effects on lives of human beings, both at individual and community levels, in its various dimensions. The World Health Organization (WHO) declared Coronavirus Disease 19 (COVID-19) a pandemic on March 11, 2020. 15 Majority of COVID–19-related deaths occurred among older adults, particularly in individuals with two or more co-morbidities, with cardiovascular disease, diabetes, chronic obstructive pulmonary disease, malignancy and chronic renal disease being the most common causes. 16 Ensuring nutrition is the ‘best practice’ against COVID-19 pandemic and in fact is one of the most cost-effective strategies to assist healthcare systems in managing patients and individuals in their recovery from COVID-19. 17 Preventive measures taken to contain the spread of the virus such as repeated lockdowns brought economic disruption which threatened nearly half the world’s workforce with loss of their livelihoods (Impact of COVID-19 on people’s livelihoods, their health and our food systems). 18 This global economic downturn caused by lockdown has adversely affected people’s ability to access food. Movement restrictions and stay-at-home orders aimed at containing the virus have directly affect the household’s ability to purchase enough food. 19 According to Moseley and Battersby, 20 people with co-morbidities are more vulnerable to COVID-19 which often results in higher mortality and morbidly rates and thereby indirectly affecting other aspects like labour, income and food access. The virus and measures to contain its spread have had profound implications for food security, nutrition and food systems. Good nutrition is a key for backing up the human immune system and lowering the perils of infections. However, as people’s ability to access food declines in the crisis, this adversely affects their ability to manage a healthy diet. 21 This impact is mostly felt in low- and middle-income countries, where the poorest households typically spending more than half of their income on food compared to households in high-income countries. 22 The shift in consumption towards to poor nutritious food during the crisis could have underpinning effects, as people who are experiencing malnutrition are more vulnerable to contracting the disease and aggravating the situation.23,24 In this background, there is a need to understand food security and the nutritional implications of the crisis and its relation to COVID-19 vulnerability.
Adequate nutrition is a crucial line of defence against viral infections. 25 Even modest deficiency of several micronutrients might affect the immune response.26,27 Relevant micronutrient consumption particularly of iron and vitamins B12, C and D have found to have an inverse relationship with illness incidence and mortality, particularly in populations with a genetic susceptibility to low micronutrient status. On the other hand, the global incidence of hunger and trace element insufficiency is expected to have an impact on COVID-19 results (Fedele et al 2021). 28
COVID-19 and Obesity
Obesity has been identified as a major negative prognostic factor for COVID-19. 29 Obesity may influence infection risk as well as overall clinical outcomes in individuals infected with H1N1 swine flu, as it was seen during the 2009 pandemic. 30 Obesity-related chronic illnesses (such as hypertension, diabetes mellitus and others) are linked to severe COVID-19 consequences; therefore, the influence of obesity on the severity of COVID-19 has attracted much interest. 31 Due to quarantine and social isolation, changes in food habits and lifestyle factors may result in nutritional deficiency. Obesity and concomitant co-morbidities are linked to physiological changes that increase susceptibility to infection, pathogenicity, and COVID-19 transmission (Figure 1). 32
COVID-19 and Nutrition
Malnutrition has been linked to increased hospital length of stay, mortality and re-admission rates and has been recognised as an adverse prognostic factor. 33 As a result, malnutrition and undernutrition are circumstances that may increase the severity and prognosis of the disease; nevertheless, suffering from COVID-19 generates a state that leads to body weight loss and malnutrition. 34 COVID-19 infection symptoms might influence food intake as well. 35 A significant link exists between vitamin D deficiency and severe COVID-19 symptoms. 36
Impaired nutritional status is linked to advanced age and comorbidities. 37 Due to changes in both innate and adaptive immune responses, the complex interplay between immunity and nutrition in ageing is clinically important and has a detrimental influence on antibody generation, vaccination response and infection susceptibility.38,39
Adults with greater rates of malnutrition were found to have an increased risk of pneumonia. 40 The new strands of COVID-19 appears to be linked to the nutritional condition of patients. Older adults, who are often malnourished, are particularly sensitive to this virus, and obesity has been linked to an increased risk of ill health and death following COVID-19 infection. 41
Malnutrition or co-malnutrition are major risk factors for many older COVID-19 patients, according to clinical findings. 42 Hospitalized older people with COVID-19 who are malnourished or have a low BMI have a higher risk of death. 43 The majority of elderly individuals admitted to hospitals for COVID-19 therapy are malnourished. 44
Co-Morbid Conditions Among Older Adults in Kerala and India
Self-reported prevalence (%) of diagnosed multi-morbidity conditions among older adults, states/uts, LASI wave 1, 2017-18.

Source: Longitudinal Ageing Survey in India 2017-18* Including spouse irrespective of age 1 multi-morbidity conditions refer to the presence of two or more chronic diseases which include hypertension, chronic heart diseases, stroke, any chronic lung disease, diabetes, cancer or malignant tumour, any bone/joint disease, any neurological/psychiatric disease or high cholesterol
In India, 26.3% of older adults aged 45 and above reported having been diagnosed with a single health condition and 17.5% with two or more health conditions. Around a quarter of older adults aged 60 and above had two or more health conditions (23.3%) compared with 12.7% among older adults aged 45–59. On the other hand, in Kerala, 28.2% of older adults aged 45 and above reported single health conditions and nearly 40% reported multiple morbid conditions. More than half of older adults aged 60 years and above have multiple morbid conditions compared with a quarter of older adults aged 45–49. This health profile suggests that Kerala has been going through an epidemiological transition with an unprecedented increase in the non-communicable disease burden. 49
Multiple comorbid conditions constitute a major public health challenge and the state is facing a high burden of NCDs and their risk factors. A systematic review of the prevalence of NCDs reveals that cardiac problems, diabetes, and all forms of cancers and chronic respiratory diseases are significantly high in Kerala. 52 One of the studies from Kerala pointed out that overweight was more predominant among the upper socio-economic class. 53 Another study observed that in Kerala, the risk factors for NCD start early in life. Kerala is a highly consumerist state in India which increasingly depends on commercially available food preparations with high content of salt, energy and trans-fats that favour the development of risk factors. 54
Results of logistic regression analysis using KAS data 2004–2019.
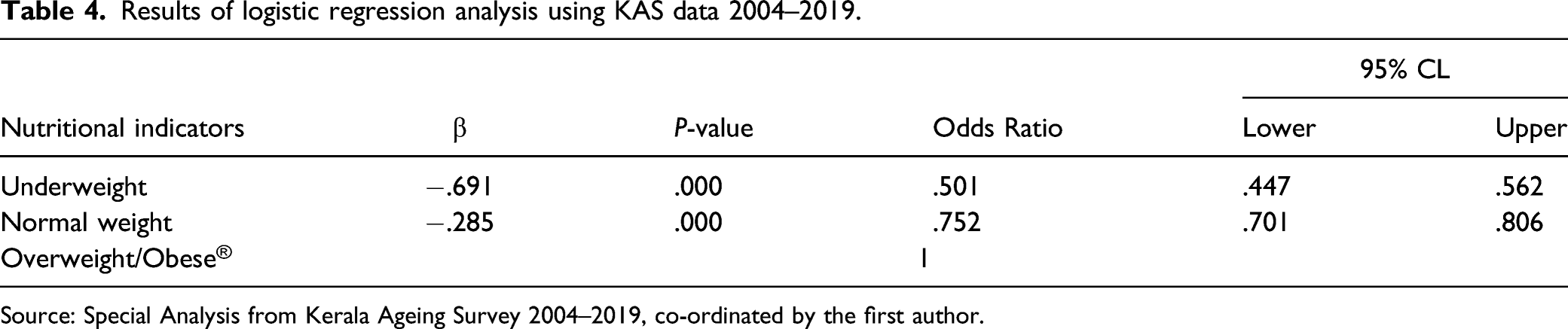
Source: Special Analysis from Kerala Ageing Survey 2004–2019, co-ordinated by the first author.
Existing health condition highlights how the on-going COVID-19 pandemic puts older persons and persons with co-morbidities at the highest risk of contracting the disease. According to the WHO, older people and people of all ages with pre-existing medical conditions (such as diabetes, hypertension, heart disease, lung disease or cancer) appear to develop serious illnesses more often than others.
COVID-19 Death Among Older Persons in Kerala
As per the data released by the Kerala government through its COVID-19 dashboard, more than half of all COVID-19 fatalities in the state occurred in the age group of 60–79 years (Figure 2). Out of the total deaths that occurred in Kerala, 56.9% of estimated deaths are in the age groups of 60–79 years and 19.1% are in age groups of 80+ years. COVID-19 deaths were predominantly among older persons compared to other age groups. Gender differentials in COVID-19 deaths also vary significantly by age, with the gender pattern of death rate not being the same in all age groups. For example, among individuals aged 0–19, 20–39 and 80+ years, females have a comparatively higher COVID-19 mortality, whereas the death rate was high among males in the 40–50 and 60–70 years age group. Up to 80 years of age, the COVID-19 death rate rises by age for both males and females. Percent distribution of COVID-19 deaths by age and sex in Kerala 2020–2021. Source: https://dashboard.kerala.gov.in/deaths.php Deaths up to February 16, 2021, as of 21/02/2021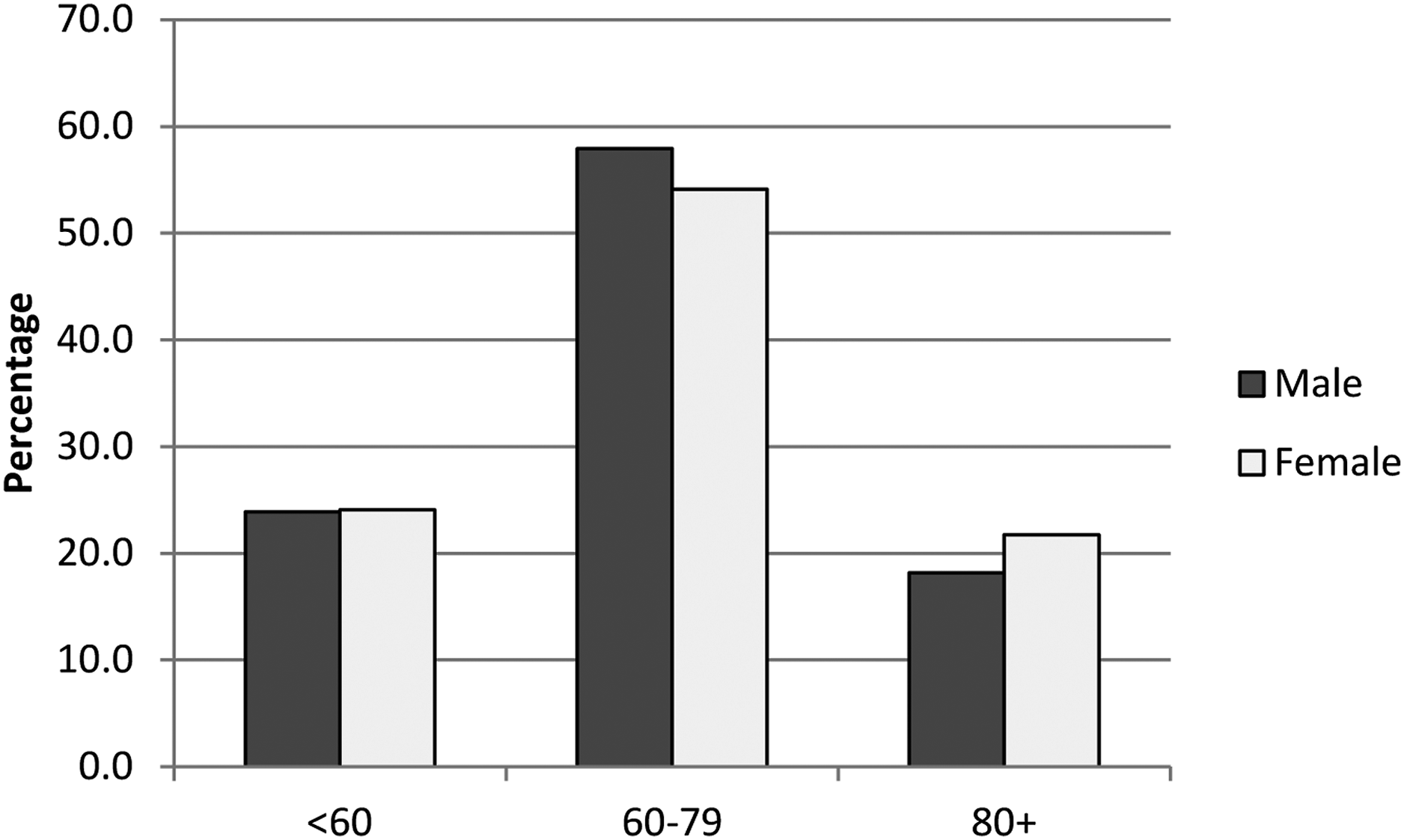
Figure 3 shows the monthly distribution of COVID-19 death among older adults in Kerala from March 2020 to February 2021. From May onwards, interstate and international travel was allowed, Keralites in Gulf and other foreign countries returned to Kerala, consequently the number of COVID-19 cases increased. However, the effective health system of the state was able to curb the death rate. From August onwards, a sudden peak in COVID-19 death was observed in Kerala and the maximum death rate was recorded between the month of October and December. Monthly COVID-19 deaths (%) among older persons in Kerala, March 2020 to February* 2021. *Deaths up to February 16, 2021 (As of 21/02/2021) Source: https://dashboard.kerala.gov.in/deaths.php
According to the Kerala Health department, most COVID-19 deaths were observed in cases without any known source of infection, while lower death rates were observed for those with a known source of infection. It was also revealed that the major co-morbidities found in Kerala’s COVID-19 death cases were cardiovascular diseases, diabetes, chronic respiratory diseases, hypertension and cancer and most deaths were diagnosed with multiple co-morbidities.
Comparison of Case Fatality Rate of COVID-19
The case fatality rate (CFR) is a measure of the ability of a virus to infect a host in infectious disease and is described as the proportion of deaths within a defined population, that is, the percentage of cases that result in death.
55
CFR helps to recognise the disease severity, identify the risk of the population and assess the quality of the healthcare system. Compared to other states in India, the case fatality rate of COVID-19 is very low in Kerala even as the state stands second in numbers of reported positive cases (Figure 4). Case fatality rates (%) of COVID-19 by states in India, up to February 16, 2021. Source: https://www.mohfw.gov.in/
Figure5 shows the CFR of COVID-19 for the state of Kerala in comparison to India and other countries. Here, the CFR is computed from March 2020 to February 2021. Even though Kerala is one of the states highly affected by COVID in the country, the number of reported COVID-19 deaths in the state is much lower than those in India as well as other highly affected nations. Kerala had a CFR of .4%; much lower than the national average (1.4%). Also, Kerala’s CFR is lower than that of the USA, UK and Italy. Thus, in comparison to India and other countries, the incidence of COVID 19 death was much lower in Kerala. Comparison of COVID-19 Case fatality rate of selected countries and Kerala. Source: https://ourworldindata.org/coronavirus
If we compare the Case Fatality Rate (CFR) of Kerala with Italy, where more than 23% of the population are older persons, Italy has a CFR of 3.4%. Applying Kerala’s (.4%) to Italy, there would be an 88% reduction in the current deaths of 96,974 (as of February 26, 2021). When a similar exercise was applied to the United Kingdom, we see an 86% reduction in total deaths. Furthermore, Figure 6 clearly states that Kerala shows a lower death rate among older persons compared to Italy. Percent distribution of deaths by age in Italy and Kerala. Source:https://www.statista.com/statistics/1105061/coronavirus-deaths-by-region-in-italy/; Source:https://dashboard.kerala.gov.in/deaths.php Deaths up to February 16, 2021, as of 21/02/2021 for both Italy and Kerala.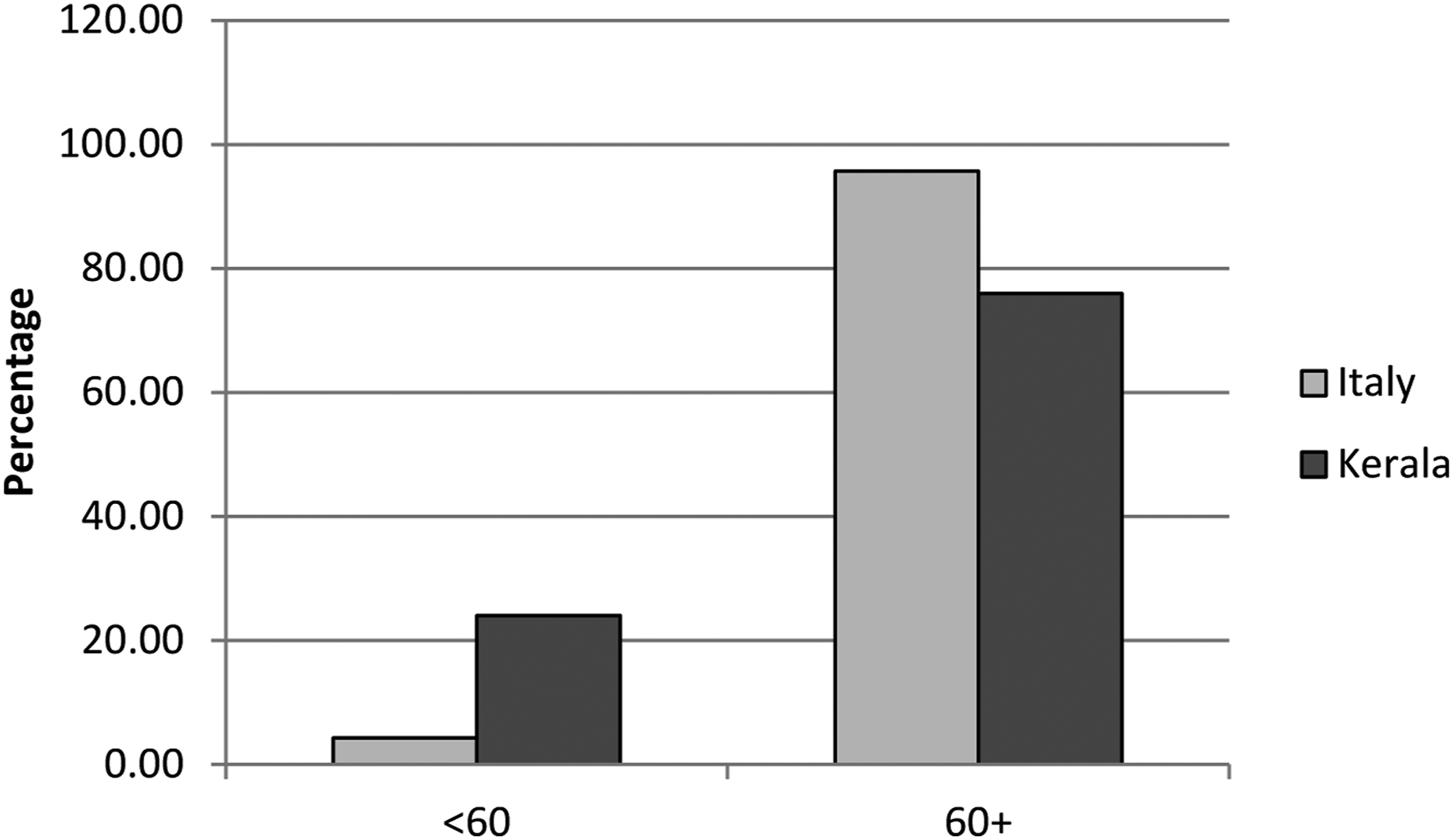
Kerala’s Approach in Controlling COVID-19
From the 1990s till now, India’s public health system was crumbling due to a lack of public investment and political commitment towards a positive social change. As a result, when the pandemic hit India, its health system as a whole was vulnerable and strained, unable to overcome new challenges. Kerala, on the other hand, has injected a new vigour into the public health system. Changes have been implemented in the state’s public health over the last four years through a primary care-centric health project called Aardram. 56 Modern public health facilities were constructed as part of the mission, with proportional enhancements in the numbers of physicians, nurses and other healthcare personnel. The programme also helped deepen neighbourhood management and strengthened hygiene and sanitation in the state. The strategy has been a huge success, and its impact was first showcased when Kerala warded off the Nipah virus outbreak in 2018. 56 Kerala’s recent accomplishment in combating the COVID-19 virus further strengthens this argument. Kerala witnessed the recovery of an old couple aged 93 and 88 years from COVID-19 with special care from a dedicated team of doctors and paramedical staff in the public health system, in stark contrast to the high COVID-19 mortality rate in the older population globally. 57
To encounter an infectious epidemic like COVID-19, the best approach is a participatory style of governance that can rapidly achieve population dissemination, and wherein the relationship between the state and its citizens is solid, trustworthy and organic. In Kerala’s approach, primary functions were discharged by local councils through active citizen engagement. To bolster this, the state also had a huge volunteer force of 377 308 that played a major role in ensuring the supply of food and relief material and also helped in maintaining steady surveillance of the population. 56 It is this powerful participatory governance mechanism that has helped Kerala’s COVID-19 control initiatives. A decentralised model of governance, a strong public health system and education are the three main pillars that influenced the nutritional and health-seeking behaviour of the population.
As soon as news began to spread about the COVID-19 virus, the Kerala state government began planning control measures. To prevent community transmission of COVID-19 in Kerala, the state government had to overcome various hurdles like high population density, a high proportion of older population and people with co-morbidities, and groups of internal migrants camping together (302, 02, 016 migrants were in relief camps during the first lockdown period, about 47.9% of the total migrants in relief camps/shelter homes all over India). 58 Furthermore, the government foresaw isolating the international migrant population returning to the state to prevent spread. Following international practice, the state government implemented a pre-planned state lockdown on March 23, 2020, one day before the Indian government announced a nationwide lockdown. The Government of Kerala released instructions for the control of the virus as soon as the virus outbreak was reported, and began recording, monitoring and quarantining suspected individuals arriving from possible epicentres and their contacts using its comprehensive ‘COVID-19 Jagratha’ portal to contain the spread of the virus.
Kerala was the first state in India to report a COVID-19 case on January 30, 2020; a student from Wuhan, China. After resolving the first case, the first wave started on March 10 with 12 cases in a family returning from Italy. On March 10, a day before the World Health Organisation declared the Coronavirus outbreak a pandemic, Kerala shut down all educational establishments and entertainment centres banned large congregations and called on people to stop visiting religious sites. As of May 1, 2020, Kerala had the lowest case fatality rate of .8% while the nationwide average was 3.23%. 59 By May 1, 2020, Kerala’s doubling time of 30 days was almost three times the national average of 11 days. 56 On 1st, 2nd and 5th May 2020, Kerala reported zero new cases. The state authorities had flattened the early curve through a series of steps that included creative contact-tracing and segregation, strict enforcement of lockdown measures and a comprehensive local public health system. The containment paradigm of the COVID-19 pandemic in Kerala was lauded not only in India but across the world.
The next phase of the pandemic started with the opening of international, national and state borders on May 7, 2020, and posed a significant challenge to holding the virus at bay, but the government again responded with committed preparation like proper documentation and screening at airports, institutional quarantine and proactive COVID-19 testing.
But merely placing people under a lockdown to prevent deaths and transmission was not easy. During the lockdown, all activities except the essential ones were to go into shutdown mode. With the economy at a halt and no daily income, families would go hungry and finally break lockdown protocols to satisfy their basic need of food. Thus, the Kerala government had to accomplish a herculean task to save lives from COVID-19 and tackle hunger in parallel.
Food Security
Among the 17 Sustainable Development Goals (SDGs) announced by the United Nations, the second one deals solely with food and nutrition, and categorically with stopping malnutrition, ensuring food security, enhancing nutrition, and fostering sustainable agriculture. India’s National Health Policy 2017 has also established a movement to shift away from ‘sick-treatment’ to ‘wellness’. This cannot be done without maintaining sufficient nutritional care for the general population, and children and women in particular. 60
According to FAO (1996), 61 food security is attained when ‘all people, at all times, have physical and economic access to sufficient safe and nutritious food that meets their dietary needs and food preferences for an active and healthy life’. The pandemic has affected food flow globally. This can be attributed to a number of reasons mainly ‘food availability’, prices and vendors and personal aspects, including geographical access, affordability, convenience and desirability”. 62
Nationwide lockdown in India to contain the spread of the virus caused economic disruption which has created unemployment in the informal sector. Since most Indians (more than 380 million) seek jobs in the informal sector are not supported by any labour laws, a formal work contractor steady income which is very likely anticipated to a decline in nutritional status. 63 According to Headey and Ruel, 64 the pandemic has acted as a catalyst for a ‘global malnutrition’. It is likely that the underprivileged will respond to the crisis by purchasing the cheapest calories they can find. The United Nations System Standing Committee on Nutrition 62 states that sustainable healthy diets with sufficient fruit and vegetables will be crucial in protecting people’s immunity against COVID-19. This is particularly important for those with pre-existing non-communicable diseases. 65 The measures to contain the spread of virus have had intense consequences for food security, nutrition and food systems. At the same time, malnutrition (including obesity) increases vulnerability to COVID-19. 24 Keeping this in mind, Government of Kerala has introduced the community kitchen and food kits through public distribution system as food security for all the people in Kerala whoever needed irrespective of their economic and social status.
The government of Kerala recognised that food security is the central threat to the population breaking lockdown protocols. They opened community kitchens on March 30, 2020, in collaboration with Kudumbashree self-help groups, local self-governments, public sector institutions, co-operatives and voluntary organisations. Under this scheme, any family or individual unable to prepare food at home was delivered meals through rapid response delivery chains, with special focus on individuals and families in quarantine/isolation, bedridden and older people, destitute persons and those living in temporary accommodation.
Contents of the grocery kit distributed by the government of Kerala and its calorie distribution.

The governmental policy of food security through grocery kits was indeed an effective strategy. It helped the internal migrant community as well as others to prepare food items of their own choice. It also had a significant impact on the COVID-19 situation in Kerala as it ensured that people stayed indoors and followed lockdown protocols, thereby reducing the rates of transmission. The delivery of food kits and food parcels through the volunteers also was a form of double-checking to ensure that none of the individuals under quarantine or lockdown broke protocols and thus helped develop an effective case monitoring mechanism.
Dietary Suggestions During the Pandemic From Various Branches of Medicine
Since nutrition is important in building the body’s resistance to infection, the former has an inevitable role in a pandemic situation. 66 Some dietary suggestions given by various bodies are the inclusion of fruits, vegetables, whole grains and nuts in the diet; ensuring that food is served at acceptable temperatures; reducing the intake of salt, sugar and oil; and avoiding fast food, bakery foods and soft drinks. Kerala also started the use of ayurvedic medicines and other natural remedies as a preventive measure in mitigating the spread of COVID-19. 67
The efficacy of the immune system is largely derived from the diet. Several vitamins (A, B6, B12, C, D, folate and E) and trace elements (zinc, copper, selenium and iron), as well as essential amino acids and fatty acids, play key roles in supporting to reduce the risk of infections, of which zinc and selenium seem to be particularly important for the latter. Dietary approaches to achieve a healthy microbiota can also benefit the immune system.
The older population of the state was the most affected because they were instructed not to go out of their homes due to their high probability of contracting the virus and developing serious infection leading to death. Similar was the case with bedridden persons, older people living alone, and those suffering from chronic illnesses and organ failures. Inability to access healthcare and procure food and other essential supplies made the situation much worse for them. The government of Kerala introduced what was known as reverse quarantine to meet the needs of these vulnerable sections of the population.
Through this scheme, any older individual (bedridden, living alone, those suffering from chronic illness and organ failures) was delivered food, medicines and other essential items through volunteer groups, local self-government (LSG) institutions and the Janamaithri Police. Primary health workers, also known as ASHAs (Accredited Social Health Activists), played a pivotal role as intermediaries between the individual and the LSG and local primary care institutions. They reported to these institutions, made lists of potential beneficiaries in their area of jurisdiction, and ensured that all essential items were delivered on time as per need. Through this mechanism, the government not only ensured minimum contact for the above-mentioned group of individuals but their nutritional and other essential needs as well, helping curb COVID-19 spread and mortality in the state.
Qualitative Study Report
Qualitative response of health professional, ASHA workers, older COVID-19 survivors and family members of the deceased older persons were collected to investigate the changes in lifestyle and dietary pattern during the pandemic.
Responses from health professionals reveal that infected patients at home or in ICUs, as well as persons under surveillance, were advised to follow a specific diet with vitamin supplements. They were also advised to drink plenty of water and follow personal hygiene and ensure proper sleep. This helped them to improve bodily defence systems and thereby reduce their vulnerability to infection. For older persons and those with advanced co-morbidity, reverse quarantine was advised. Older persons with co-morbidities were also advised to follow a disciplined lifestyle, eat healthy meals, take medications without fail and closely monitor their health condition. They were advised to report immediately to the health facilities if they noticed any suspected symptoms.
The information collected from ASHA workers revealed that close monitoring of older persons who were in reverse quarantine was done, and ASHAs were actively willing to help with their needs regarding medicines, food and other essentials. These persons were visited frequently to enquire about their health conditions and encouraged to follow a proper nutritional diet and good personal hygiene.
Interviews with older COVID-19 survivors indicated they followed the advice of health professionals and ASHA workers properly by changing their dietary patterns. During their reverse quarantine period, they were forced to change their lifestyle behaviour through intake of timely dietary food, and natural herbs and other ayurvedic medicine as preventive measures. Even with co-morbidities, the change in their nutritional behaviour improved their ability to cope with the infection.
Interviews with family members of deceased older persons revealed that most deaths occurred while under treatment for co-morbidities. Older persons admitted for the treatment of co-morbidities got infected through their bystanders or by other means.
The qualitative report of the study clearly revealed that during the pandemic period the state population fought against the virus by changing their lifestyle behaviour like by taking a healthy and nutritional diet. Eating home cooked food, drinking plenty of hot water, avoiding overuse of junk and other processed foods not only helped the population to improve their nutritional level but also enhance their resistance to infection. There are several situations during the pandemic that could have compromised access to adequate nutrition due to social isolation; a necessary measure to contain the spread of COVID-19. However, the effective implementation of the food security system through proper decentralisation of work dissemination helped the government manage this situation efficiently. The main preventive public health strategies of the state in response to COVID-19 was to provide essential health services and social services including integration of sustainable food system interventions to promote the production, distribution and consumption of healthy diets. Thus, the state was able to manage the low fatality rates of COVID 19 through evidence-based strategic plans.
Discussion
The Government of India formulated the National Nutrition Policy in 1993. In general, major nutrition problems in Kerala are undernutrition, anaemia, overweight, obesity and dietary/nutritional disorders. Disproportionate dietary and nutritional disorders in older adults make them more vulnerable as they pass through multiple ailments. The state of Kerala has a nutrition policy to reduce these problems based on a ‘life cycle approach’, which was formulated in 2014 with the technical support of UNICEF. According to the National Family Health Survey (NFHS – 4), Kerala reported, overweight and obesity as most prevalent in older adults. Several non-communicable disease (NCD) risk factors, including obesity, diabetes and cardiovascular disease, are associated with an increased risk of serious illnesses and death from COVID-19. This has evidence from the words of a family member of a deceased older adult that the patient had chronic co-morbidities such as heart problems and diabetes. Also, this study proved that the post–COVID-19 condition is highly vulnerable to co-morbidities and may lead to death. This was proven by the words of an ASHA worker who was directed to take the information of a deceased older woman aged 70 years and had no serious diseases before COVID-19. Coming home with a negative certificate of COVID-19 infection, she again was admitted to the hospital after 15 days with severe heart and kidney problems and eventually died. To rectify this issue, the state health department of Kerala launched a major mission for COVID-19 recovered through post-COVID-19 outpatient clinics with the assistance of ASHA workers and health staff. 68
Another older person who had been admitted to the hospital with a history of respiratory problems died, and only after his death did the family realise that he had COVID-19. COVID-19 infection is associated with the risk of malnutrition, and malnutrition due to illness puts immune-compromised people at a higher risk of acquiring the infection. Older age and the existence of comorbid disorders are considered to be linked with impaired nutritional status and sarcopenia. 69 A high body mass index with COVID-19 also tends to be correlated with a bad prognosis and indicates that sarcopenic obesity plays a significant role. 70
Higher IFR (Infection Fatality Ratio) is mostly coupled with co-morbidities like diabetes, obesity and heart diseases. However, countries with improved healthcare systems will be able efficiently care for people infected by COVID-19 and thereby have better chances of survival. 71
On the other hand, the COVID-19 Case Fatality Rate is very low in Kerala for the general population as well as for older persons. Community kitchens during the lockdown period and grocery kits delivered every month through the public distribution system ensured that the population met the nutritional needs to prevent COVID-19 along with ayurvedic and homoeopathic preventive medicines and natural herbs. One ASHA worker remarked that the community kitchen was introduced particularly for those who are old, destitute, bedridden and living alone. Under their guidance, three meals and two snacks were prepared daily and distributed – breakfast, lunch with leafy vegetables, and dinner at optimum temperatures – through volunteers. A senior official at the Health Department said that through community kitchen services, they not only fulfilled nutritional needs but also ensured beneficiaries were following lockdown and quarantine rules by not giving them a reason to step out of the house. Recent evidence shows that individual nutritional status has a substantial effect not only on individual response to pathogens but also on the viral genome’s genetic make-up, viral intensity and reproducible genome mutations. Micronutrient intake in combination with a well-balanced macronutrient diet can help boost the resistance of the body to fight off viruses. 72
A doctor pointed out that even if the person does not have vitamin supplements, actual nutrition demands were met through their food. Thus, it has been proven by the analysis of the pre-COVID-19 situation among older persons that nutrition has a significant role in determining mortality. In other words, older persons who are at risk of nutrition have higher chances of dying. In the analysis, overweight or obese conditions of older persons have no significant role in determining mortality. However, things have changed in the COVID-19 period. Though an older person with normal nutritional levels has a lesser risk of mortality during the pandemic, older people with comorbid conditions and who are overweight/obese have a higher risk of mortality. COVID-19’s association with the global increase in chronic disease and associated risk factors, such as obesity, elevated blood sugar, cardiovascular disease and other non-communicable diseases (NCDs) elevate the risk of serious illness and death from COVID-19.73,74
The study is undertaken from a socio-epidemiological perspective and hence the study could not dive into any clinical nutritional assessments of the COVID-19 patients. The study utilises the KAS and LASI datasets to analyse how nutritional status associates with the comorbid conditions and mortality of the older population in the pre-COVID-19 period. For comparative purposes, the study rather relies on the data collected through qualitative interviews with surviving COVID-19 patients as well as families of the deceased, leading health practitioners and frontline health workers in the state.
Conclusion
Kerala has ensured a good nutritional status to its population, especially its older population which helped in enhancing their ability to resist infection and serious complications during the COVID-19 pandemic, leading to low COVID-19 mortality in the state. However, non-communicable diseases and underlying risk factors such as obesity are high among older persons, making them a particularly high-risk group. Obesity has a significant role in determining COVID-19-related mortality while its role was statistically insignificant during the pre-COVID-19 situation.
The COVID-19 outbreak has brought a great challenge for communities and healthcare systems across the world. Considering the absence of specific therapeutic treatment or an effective vaccine in the initial stages of the outbreak, countries were forced to take strong precautionary measures to contain the spread of COVID-19, ranging from social distancing to community quarantine. With no sudden end to the pandemic, and with new strains and variants emerging globally, it is important to alter people’s behavioural and dietary patterns to fight against current and future pandemics. Therefore, the study suggests there is an utmost need for alerting the general population about the nutritional impact on COVID-19 outcome. In addition, nutritional status must be considered as a key indicator while drafting the COVID-19 health policy to ensure the better good of the community.
Post Script – Updates After First Wave
The second wave of the COVID-19 pandemic hit India around April–May of 2021. It was much bigger than the first, in terms of caseload, mortality and the way it affected not just the poor and vulnerable but the rich and healthy as well. The second wave, at its peak, pushed health systems in many parts of the country to the brink of collapse. Popular media was rife with reports of people from all walks of scampering to arrange beds, ventilators and oxygen cylinders for loved ones. Hospitals reportedly overflowed with patients, and NGOs and voluntary organizations operated drive-through oxygen parlours to support dying patients with prized sniffs of the life-saving gas. Through gory images of dead bodies floating on the Ganges and empty parking lots turning into mass funeral pyres, the second wave painted a picture of gloom and doom over the whole country.
One small corner of India, however, was managing to keep its nose above the water through the cataclysm. Through its successful management of the first wave, Kerala had learned that decentralized management was the cornerstone of any success against this deadly virus. It had, in anticipation of the exponential increase in cases through the second wave, set up more than 1.5 lakh beds in field hospitals across more than one thousand panchayats and municipalities (local governance regions) to bolster the existing healthcare system. It had ensured the availability of adequate centralized oxygen beds, Medical Oxygen storage capacities, ICU beds, and ventilators in all districts. As the second wave gained momentum, the government in Kerala set up a centralized Oxygen War Room to streamline the production, transportation, distribution, storage, and usage of Medical Oxygen. As a result of this rigorous effort, there was not a single COVID-19 death due to the unavailability of Medical Oxygen or Intensive Care in Kerala.
In addition to stepping up medical care facilities, an important lesson that Kerala had learned through its first wave experience was the importance of nutrition and food security in effectively managing the impact of the pandemic. Multiple studies and reports, including the present one, had highlighted the impact of nutrition and food security not only in helping build immune resistance but also indirectly ensuring adherence to quarantine and isolation guidelines. The ‘Grand Care’ elderly protection programme implemented jointly by the Health Department and the Kudumbashree Mission had, through its syndromic surveillance during the first wave, found out a significant reduction in cases among elderly persons in districts where their mobility was lower, and also identified a similar positive correlation between reduced mobility and doorstep availability of food and long-term medication. 74 Such evidence, coupled with its overall success in ensuring availability of food through its community kitchens and Public Distribution System, prompted Kerala’s government to continue its efforts at ensuring availability of food, adequate in quantity and quality, to its population.
With the easing of lockdown measures and increasing mobility of the population following the decline of the first wave, community kitchens were phased out and replaced by ‘ration kits’ containing adequate supplies of grains, pulses and other essentials. The government ensured universal access to these kits through its extensive public distribution network, with the assumption that any method of targeting would result in exclusion of some communities, an outcome that was untenable in the midst of the second-wave crisis. Serendipitously timed with Kerala’s general elections, this strategy was widely touted as an important reason for the government’s landslide re-election to power, in addition to being critically important in ensuring resilience to the vastly more devastating second wave. 75 Having successfully overcome the second wave and cases and mortality declining steadily, the government in Kerala seems to have decided that the nutrition route is here to stay. In a recent announcement by its Chief Minister, Kerala’s government decided to continue the expansion of ‘Janakeeya Hotels’. These budget restaurants, initially transformations of COVID-19 community kitchens and later included in the annual budget as part of the ‘Hunger-free Kerala’ programme, are run by the grassroots women’s collective Kudumbashree with a 50% subsidy support from the government, and provide packed meals at affordable rates (20 Indian rupees or .27 USD) to the public. As on October 11, 2021, more than 1.76 lakh daily meal packets were served through 1132 such budget restaurants. 75
Kerala’s policymakers have realized, through experience, the importance of nutrition and food security in the resilience of its community against unprecedented shocks such as the COVID-19 pandemic. Through strategies such as community kitchens and ration kits, Kerala was able to adequately support its health system in effectively mitigating the effects of the pandemic. More importantly, however, the experience has ensured the centrality of nutrition and food security in Kerala’s policy discourse in the long term.
Footnotes
Author Contribution
The corresponding author conceptualised the main idea for the manuscript and encouraged all the authors to investigate the cause. All the authors contributed equally in drafting, analysing, revising and approving the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The consent for case studies was obtained verbally via telephone.