
Abstract
We performed a pairwise and network meta-analysis to compare pathological complete response (pCR) among neoadjuvant chemotherapy in patients with triple-negative breast cancer. We searched PubMed for randomized clinical trials between January 1, 2000 and December 1, 2020. Abstracts from meetings were also searched. A frequentist random-effect model was applied to compare pCR and toxicities. The P-score was used to rank treatment effects. Nineteen trials with 16 treatments and 7794 patients were included. On the basis of SoC, the addition of carboplatin (OR = 1.82, 95% CI, 1.24 to 2.68, P < .01) and the addition of checkpoint inhibitors (OR = 1.69, 95% CI, 1.23 to 2.32, P < .01) increased pCR in pairwise meta-analysis; compared with paclitaxel, nab-paclitaxel did not improve pCR rates (OR = 1.81, 95% CI, .80 to 4.12, P = .16). The anthracycline-sparing regimen led to similar pCR compared with the anthracycline-containing regimen (OR = 1.50, 95% CI, .82 to 2.76, P = .19). In network meta-analysis, the addition of carboplatin plus a PD-1 inhibitor (pembrolizumab), carboplatin plus bevacizumab, and carboplatin plus veliparib ranked as the top three treatments for achieving pCR, with corresponding P-scores of .91, .84, and .72, respectively. Among patients with homologous recombination deficiency, the addition of carboplatin (OR = 1.31, 95% CI, .69 to 2.50, P = .41) or carboplatin plus PARP inhibitors (OR = 1.19, 95% CI, .58 to 2.47, P = .63) did not increase pCR. For triple-negative breast cancer, combining carboplatin with taxane-anthracycline-containing neoadjuvant chemotherapy could be the standard of care, and the combination containing checkpoint inhibitor is promising. However, their role in long-term oncologic outcome remains to be determined.
Keywords
Neoadjuvant chemotherapy with taxane-anthracycline-based regimens is a preferred approach for high-risk early triple-negative breast cancer.
Carboplatin-containing regimens as neoadjuvant chemotherapy for triple-negative breast cancer could be the standard of care and adding a checkpoint inhibitor to such regimens is promising.
A new standard of neoadjuvant treatment in triple-negative breast cancer should be supported by long-term oncologic outcome.What do we already know about this topic?
How does your research contribute to the field?
What are your research’s implications toward theory, practice, or policy?
Introduction
Triple-negative breast cancer is characterized by a lack of estrogen receptor, progesterone receptor, and human epidermal growth factor 2 expression, but it represents a highly heterogeneous subtype in breast cancer. 1 Neoadjuvant chemotherapy is a preferred approach for high-risk early triple-negative breast cancer. 2 Regimens with taxanes and anthracyclines are standard of care, resulting in a pathological complete response (pCR) rate in approximately 40% of patients. 3 pCR has been validated as a surrogate for disease-free and overall survival for patients with early triple-negative breast cancer who received neoadjuvant chemotherapy. 4
Platinum and poly (ADP-ribose) polymerase (PARP) inhibitors both exhibit antitumor activities against triple-negative breast cancer in the metastatic setting,5,6 and they have been shown to increase pCR rates in triple-negative breast cancer when added to standard neoadjuvant chemotherapy.7,8 In addition, breast cancers with homologous recombination deficiency, including BRCA1/2-proficient tumors, are relatively sensitive to platinum and PARP inhibitors. 9
Immunotherapy with checkpoint inhibitors has also shown antitumor activities when combined with chemotherapy in triple-negative breast cancer. 9 A phase 1b trial of neoadjuvant pembrolizumab plus chemotherapy reported remarkable pCR rates in triple-negative breast cancer. 10 Despite all efforts to improve pCR, the role of neoadjuvant chemotherapy on long-term survival remains undefined in triple-negative breast cancer, and pCR improvement is usually accompanied by increased toxicity.
By searching relevant trials investigating neoadjuvant chemotherapy in triple-negative breast cancer, we conducted a pairwise and network meta-analysis to compare pCR rates and toxicities among different regimens. We also performed subgroup analysis in patients with homologous recombination-deficient tumors.
Methods
Study Eligibility and Identification
We searched PubMed and Cochrane Central Register of Controlled Trials for prospective randomized controlled trials that investigated neoadjuvant chemotherapy in patients with early triple-negative breast cancer. For unpublished studies, we searched abstracts from meetings of the American Society of Clinical Oncology, the San Antonio Breast Cancer Symposium, and the St. Gallen Conference. We limited our search between January 1, 2000 and December 1, 2020. This study was conducted under the recommendations of the PRISMA protocol.
The following terms were used for the search: breast neoplasm, cancer, or carcinoma; triple-negative; neoadjuvant chemotherapy; platinum; checkpoint inhibitor; PARP inhibitor; systemic review; meta-analysis; and randomized controlled trials.
Inclusion criteria of trials for this analysis were those with the following characteristics: (1) randomized controlled trials included triple-negative breast cancer; (2) early breast cancer; and (3) published with available data of pCR and toxicities.
Exclusion criteria of trials for this analysis were those with the following characteristics: (1) non-randomized trials; (2) phase-I trials; (3) without sufficient results for pCR; and (4) with metastatic breast cancer.
Data Extraction and Assessment for Risk of Bias
We extracted the following information from the included trials: study name, year of publication or meeting presentation, trial phase, sample size, pCR rates, and regimens. The numbers of patients who achieved pCR were directly extracted for analysis. A pCR (ypT0/isypN0) was defined as the absence of any invasive tumor cells in the breast and lymph nodes. Data extraction was conducted by 2 authors (X. L and J. L) independently, and disagreement was resolved by discussion with the third author (S.W). Cochrane Collaboration Recommendations for Assessment was used to evaluate the risk of bias (RoB2) by 2 authors, and discrepancy was resolved by discussion. The resulting plot was produced by the R software using the robvis package. Publication bias was assessed by the funnel plot and the Egger’s test.
Statistical Analysis
We conducted a traditional pairwise meta-analysis of pCR rates among 5 subgroups: taxane-anthracycline-containing regimens with carboplatin vs without; regimens with PARP inhibitors plus carboplatin vs without; regimens with checkpoint inhibitors vs without; regimens with nab-paclitaxel vs that with paclitaxel; and regimens with anthracycline vs without. The pooled OR was estimated using a general variance-based method.
Next, we performed network meta-analysis to rank the effects of treatments regarding pCR and toxicity (including neutropenia, anemia, thrombopenia, peripheral neuropathy, and vomiting). The pooled OR was estimated by the frequentist weighted least-squares algorithm, which is more user-friendly due to easier computation and programming but produces similar results and rankings for network analysis.11,12
Using the netrank function of the netmeta package in R, the P-score was obtained for each treatment and was used to rank treatment effects and toxicities, with higher scores indicating a greater probability for an event to occur.
Heterogeneity and inconsistency in the network were assessed by the Q total statistic, which can be decomposed into within-design heterogeneity and between-design inconsistency. The built-in net heat function enables the visualization of inconsistency between direct and indirect evidence in a network estimate, which was applied in this study. The red color in the corresponding graph indicates high inconsistency; blue indicates low inconsistency. When significant heterogeneity and inconsistency were found, a random-effect model was used; otherwise, a fixed-effect model was employed.
All analyses were performed with R (version i386.3.3.2). A statistical test with P<.05 was considered significant. Hypothesis tests were two-sided.
Results
For network meta-analysis, we identified 19 trials including 14 full publications13,15-22,24-26,29,31 and 5 meeting abstracts14,23,27,28,30 by the search strategy, as illustrated in the flow chart (Figure 1). Of the 19 trials (with 7794 patients), 15 were limited to patients with triple-negative breast cancer; for the 4 remaining trials (the GeparSepto,
13
GeparOLA,
14
ISPY2,
15
and the ETNA
16
trial), only patients with triple-negative breast cancer were included in the analysis. Three trials were designed with multi-arms (the CALGB 40603
17
and BrightNess
18
trials). The risk of bias for all included trials was low (Figure S1). The funnel plot and linear regression test (P = .052 for Egger’s test) both indicated little publication bias. (Figure S2) Flow chart of the literature search and article selection process.
For analysis of patients whose tumors showed homologous recombination deficiency, 2 studies limited to patients with confirmed status of homologous recombination deficiency (the TBCRC 030 32 and TBCRC 031 29 trials) and subgroups in 4 trials that reported pCR rates (the GeparOLA, 14 BrightNess, 18 GeparSixto, 19 and the GeparOcto 20 trial) were included, with a total of 551 patients.
Main characteristics of included studies.

A, doxorubicin; Ate, atezolizumab; Bev, bevacizumab; C, cyclophosphamide; Cb, carboplatin; Cis, cisplatin; D, docetaxel; Durv, durvalumab; E, epirubicin; F, fluorouracil; Gem, gemcitabine; M, non-pegylated liposomal doxorubicin; NabP, nab-paclitaxel; Ola, olaparib; P, pacalitaxel; pCR, pathological complete response; PD-1, program death-1; PD-L1, program death ligand-1; Pem, pembrolizumab; TNBC, triple-negative breast cancer; Veli, veliparib. *These 2 trials were not included in the network meta-analysis.

Network of comparisons of sixteen treatments. Each node denoted each treatment. The width of the lines was proportional to the number of trials comparing 2 treatments, and the size of the node was proportional to the sample size of each treatment.
The Q total statistic indicated heterogeneity and inconsistency in the network (Q = 30.56, P < .01). The subtotal Q statistic for heterogeneity indicated that the within-study design was the main source for heterogeneity (Q = 22.70, P < .001), whereas the subtotal Q statistic for inconsistency showed little between-design inconsistency (Q = 7.86, P = .09). Therefore, we used a random-effect model in this study for all network analyses, and the net heat plot indicated low inconsistency when a random-effect model was used (Figure S3).
In pairwise meta-analysis of pCR (Figure 3), adding carboplatin to the PA-based regimen increased pCR (OR = 1.82, 95% CI, 1.24 to 2.68, P < .01); adding carboplatin and PARP inhibitors to the PA-based regimen also increased pCR rates (OR = 2.64, 95% CI, 1.84 to 3.79, P < .01). The addition of checkpoint inhibitors to chemotherapy led to a significant improvement in pCR (OR = 1.69, 95% CI, 1.23 to 2.32, P < .01). Compared with paclitaxel, nab-paclitaxel did not improve pCR rates (OR = 1.81, 95% CI, .80 to 4.12, P = .16). The anthracycline-sparing regimen led to similar pCR compared with the anthracycline-containing regimen (OR = 1.50, 95% CI, .82 to 2.76, P = .19). Forest plot of odds ratios for pathological complete response of 5 subgroup analyses by pairwise meta-analysis. The squares in the figure represent odds ratios (OR) for each trial, and the horizontal lines indicate the 95% confidential interval (CI) for the OR. The diamond represents the pooled OR, as based on a random-effect method. All statistical tests were 2-sided.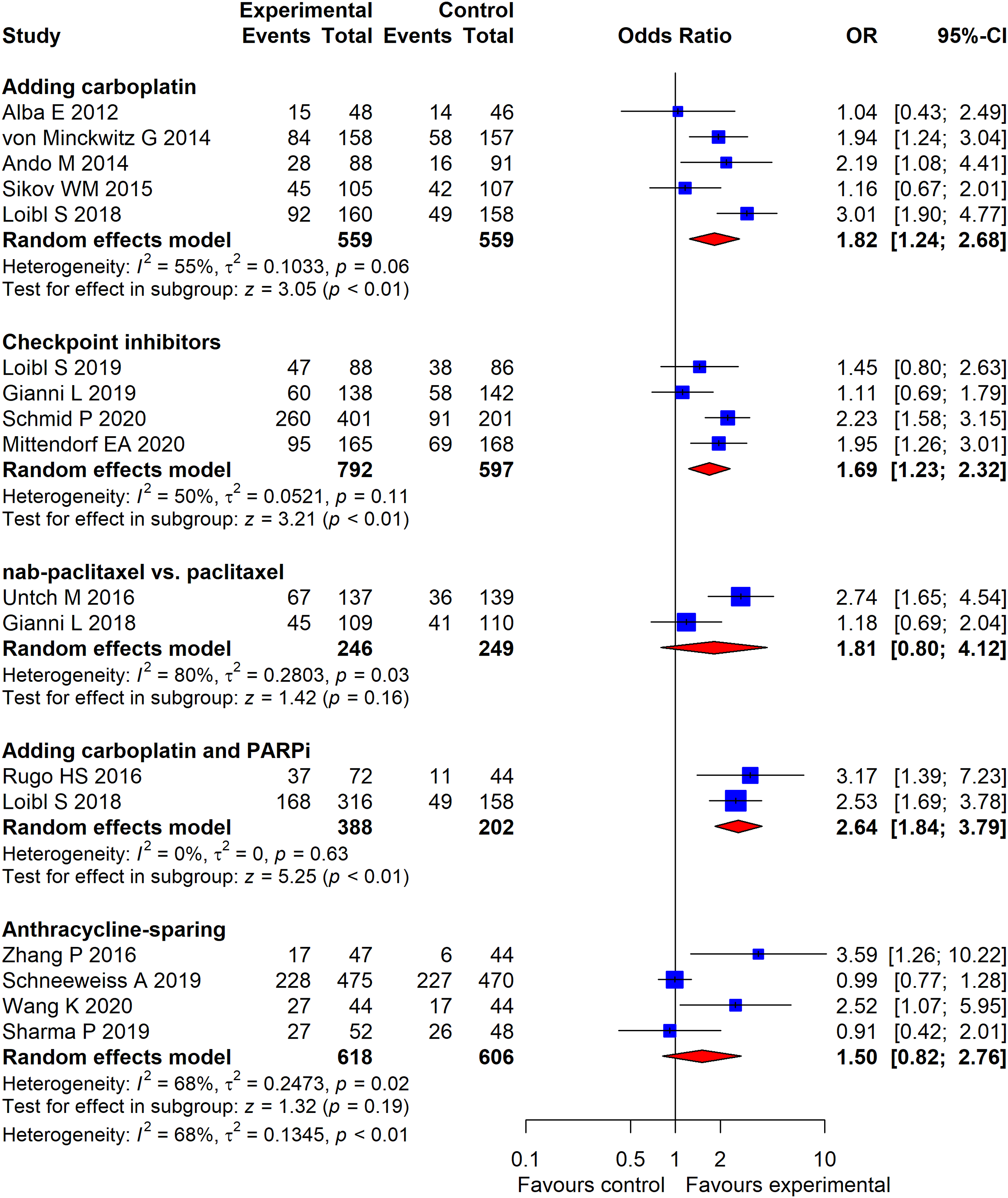
In network meta-analysis of pCR (Figure 4), on the basis of a PA-based regimen, the addition of carboplatin plus a PD-1 inhibitor (pembrolizumab), carboplatin plus bevacizumab, and carboplatin plus PARP inhibitors ranked as the top three treatments to achieve pCR, with corresponding P-scores of .91, .84, and .72, respectively. Network meta-analysis also showed that three anthracycline-sparing treatments (paclitaxel plus carboplatin, docetaxel plus carboplatin, and nab-paclitaxel plus carboplatin) induced comparable pCR when compared with the standard PA-based treatment. Table 2 presents the pairwise comparisons of the 16 treatments. Forest plot of odds ratios for pathological complete response of neoadjuvant therapies compared with the reference arm (paclitaxel-anthracycline-based therapy) by network meta-analysis. The squares in the figure represent hazard ratios (OR) for each trial, and the horizontal lines indicate the 95% confidential interval (CI) for the OR. The diamond represents the pooled OR, as based on a random-effect method. All statistical tests were 2-sided. Pairwise comparisons of pathological complete response among the 16 treatments. Each cell represents the pairwise comparison of treatment in the column versus treatment in the row, which contains the odds ratio and its 95% confidence interval underneath. Significant hazard ratios are in bold. PA, pacalitaxel-anthracycle; PD-1, program death 1; Cb, carboplatin; Bev, bevacizumab; D, docetaxel; NabP, nab-paclitaxel; Gem, gemcitabine.

On the basis of paclitaxel and anthracycline, the addition of carboplatin (OR = 1.31, 95% CI, .69 to 2.50, P = .41) or carboplatin plus PARP inhibitors (OR = 1.19, 95% CI, .58 to 2.47, P = .63) did not increase pCR for patients with homologous recombination deficiency (Figure 5). Cisplatin yielded similar pCR rates as paclitaxel or doxorubicin-cyclophosphamide did (OR = .74, 95% CI, .43 to 1.27, P = .27). Forest plot of odds ratios for pathological complete response in patients with homologous recombination deficiency tumors.
Regarding nonhematologic toxicities, the nab-paclitaxel-containing regimen ranked highest in neuropathy development (Figure S4), although no differences in vomiting were observed among all regimens (Figure S5). In terms of hematologic adverse events, carboplatin plus PARP inhibitors caused the most neutropenia (Figure S6) and thrombocytopenia (Figure S7), and carboplatin plus bevacizumab caused more anemia than any other treatments (Figure S8).
Discussion
Early triple-negative breast cancer is associated with a high risk of recurrence. 34 Neoadjuvant chemotherapy induces relatively high pCR rates, and Oxford meta-analysis has confirmed the role of pCR in prognosis in early triple-negative breast cancer. 4 Indeed, neoadjuvant chemotherapy in triple-negative breast cancer is an active area of research involving novel agents in the pursuit of higher pCR rates. This pairwise and network study compared pCR rates among 16 neoadjuvant regimens, with recent advances in early triple-negative breast cancer.
Nab-paclitaxel has been compared with paclitaxel in 2 large randomized trials.13,18 In the GeparSepto study, 13 nab-paclitaxel significantly enhanced the pCR rate by 22% (48% vs 26%), although the ETNA study was unable to repeat these results. 18 Based on pairwise and network analyses in our study, nab-paclitaxel did not increase pCR rates compared with paclitaxel. Regarding invasive disease-free survival, the updated GeparSepto study showed a significant benefit for nab-paclitaxel in the overall study population but not for patients with triple-negative breast cancer. 35 Taking toxicity and cost into account, nab-paclitaxel was not recommended as a substitute for paclitaxel, but it remained a reasonable treatment choice for patients who had contradictions to paclitaxel.
Platinum salts have been extensively evaluated in triple-negative breast cancer in both metastatic and neoadjuvant settings. The results of our study support incorporating carboplatin into taxane- and anthracycline-based regimens to induce higher pCR rates. A recent meta-analysis had the same recommendation. 36 However, platinum-based neoadjuvant chemotherapy is associated with worse hematological toxicities. Although the GeparSixto study found a significant improvement in disease-free survival, 37 the CALGB 40603 study did not. 38 Neither of these 2 studies demonstrated a benefit in overall survival.
When carboplatin is used as a component in the neoadjuvant setting, an anthracycline-free regimen is of substantial clinical interest.25,28,30 The advantages of anthracyclines include shortened treatment duration, avoidance of potential cardiac toxicity, and possible pCR improvement. The combination of a taxane (docetaxel, paclitaxel, or nab-paclitaxel) with carboplatin in our study resulted in comparable pCR rates when compared with taxane and anthracycline-based regimens.
PARP inhibitors exhibit synergistic antitumor effects when combined with carboplatin in triple-negative breast cancer. Two studies included in the present meta-analysis added veliparib and carboplatin to standard neoadjuvant treatment. The phase 2 I-SPY study reported pCR rates that nearly doubled in patients who received veliparib plus carboplatin compared to those who received a standard neoadjuvant AT-based regimen. 15 However, the phase III BrightNess trial showed that the addition of veliparib did not increase pCR rates in patients who received paclitaxel and carboplatin. 18 Similarly, our network meta-analysis detected no improvement in pCR rates when adding veliparib to a regimen containing carboplatin, taxane, and anthracycline. Overall, not all patients with triple-negative breast cancer respond to PARP inhibitors. Theoretically, only tumors with homologous recombination deficiency, such as alterations in BRCA 1/2 and ATM genes, are sensitive to PARP inhibitors. The GeparOLA trial enrolled patients with homologous recombination deficiency and showed that the addition of olaparib to paclitaxel resulted in pCR rates similar to those obtained with the addition of carboplatin to paclitaxel, though formal comparison between the 2 arms was not planned. 14
Nonetheless, our subgroup pairwise meta-analysis in patients with homologous recombination deficiency did not find an increase in the pCR rate with the addition of carboplatin or carboplatin plus PARP inhibitors to standard neoadjuvant. As anthracyclines inhibit DNA replication and transcription, they might be potent drugs against tumors with homologous recombination deficiency. 39 In this context, regimens containing anthracyclines were of sufficient efficacy for these tumors. However, these findings should be interpreted cautiously because they are based on patients from unplanned subgroup analysis from each included trial.
The TBCRC 031 and TBCRC 030 trials both only enrolled patients with homologous recombination deficiency and used investigational cisplatin in a comparison with doxorubicin-cyclophosphamide or paclitaxel,32,33 respectively, showing similar pCR rates between the cisplatin and control arms. The results from the meta-analysis of these 2 trials in our study were in line with these reports. However, neither trial used established regimens that usually contain a taxane-anthracycline backbone. Available evidence did not support platinum alone as neoadjuvant therapy for TNBC.
The addition of checkpoint inhibitors to chemotherapy can improve efficacy in patients with metastatic TNBC,40,41 prompting trials to investigate such agents in the neoadjuvant setting. In the phase 1b trial KEYNOTE-173, neoadjuvant pembrolizumab and chemotherapy induced a pCR of 60%. 10 The subsequent phase III KEYNOTE-522 trial validated data from the KEYNOTE-173 trial. Our meta-analysis included 3 studies investigating three checkpoint inhibitors, with 1 study using the anti-PD-1 antibody pembrolizumab 29 and 2 using the anti-PD-L1 antibodies atezolizumab 27 and durvalumab. 26 The conventional pairwise meta-analysis showed increased pCR with the combination of checkpoint inhibitors and chemotherapy, but the network meta-analysis showed that only the combination of an anti-PD-1 antibody (pembrolizumab in this study) and chemotherapy led to higher pCR, whereas the combination of an anti-PD-L1 antibody (atezolizumab and durvalumab) and chemotherapy did not. It should be noted that the chemotherapy backbones in these trials were different, which may impact the efficacy of checkpoint inhibitors. Moreover, the duration of immunotherapy and the patients’ baseline characteristics varied among trials. Finally, the effect of immunotherapy might be better measured by survival outcomes, not only among patients with pCR but also among those with residual disease. Currently, no study in this area has reported conclusive evidence of improved long-term survival outcomes in patients with TNBC who had received neoadjuvant checkpoint inhibitors.
Several limitations existed in the present study. First, significant heterogeneity was detected. Some obvious factors contributed to such heterogeneity: different study designs, multiple treatment arms, and various patient characteristics. Five included trials were presented as abstracts without detailed information. In addition, some trials enrolled small proportions of patients other than those with TNBC who were excluded from the analysis. Accordingly, a random-effect model was used. Second, our study compared pCR among different neoadjuvant regimens in TNBC but was unable to evaluate survival outcomes, which is a substantial limitation for most meta-analyses. Long-term oncologic outcomes were the goal of neoadjuvant therapy for this patient population, which has a high risk of relapse. However, in most trials, follow-up was insufficient to assess survival. We believe that a meta-analysis based on individual patient data would yield more informative results.
Conclusion
In conclusion, the results from our pairwise and network meta-analysis did not support nab-paclitaxel as a routine substitute for paclitaxel but do support the addition of carboplatin to standard neoadjuvant regimens. The role of PARP inhibitors remains to be investigated. For tumors with homologous recombination deficiency, taxane-anthracycline-containing regimens should still be the standard of care. Finally, the combination of anti-PD-1 antibody pembrolizumab and chemotherapy was associated with the highest pCR rates, but its impact on long-term survival remains to be determined.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580211056213 – Supplemental Material for Neoadjuvant Chemotherapy in Early Triple-Negative Breast Cancer: A Pairwise and Network Meta-Analysis of Pathological Complete Response
Supplemental Material, sj-pdf-1-inq-10.1177_00469580211056213 for Neoadjuvant Chemotherapy in Early Triple-Negative Breast Cancer: A Pairwise and Network Meta-Analysis of Pathological Complete Response by Zeng-Jie Weng, Sheng-Xi Wu, He-San Luo, Ze-Sen Du, Xu-Yuan Li and Jia-Zhou Lin in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580211056213 – Supplemental Material for Neoadjuvant Chemotherapy in Early Triple-Negative Breast Cancer: A Pairwise and Network Meta-Analysis of Pathological Complete Response
Supplemental Material, sj-pdf-2-inq-10.1177_00469580211056213 for Neoadjuvant Chemotherapy in Early Triple-Negative Breast Cancer: A Pairwise and Network Meta-Analysis of Pathological Complete Response by Zeng-Jie Weng, Sheng-Xi Wu, He-San Luo, Ze-Sen Du, Xu-Yuan Li and Jia-Zhou Lin in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.