
Abstract
Background
Despite nationwide efforts to address the diabetes epidemic and reduce prevalence disparities, higher rates persist among the poor, especially those with limited literacy. Currently, individuals with abnormal glycemia who have pre-diabetes and diabetes qualify for different programs. However, evidence suggests that, for low-income Hispanic/Latinos, offering a single intervention to all those with abnormal glycemia may provide a more culturally acceptable and effective approach. Our objective was to explore the feasibility of such an intervention led by community health workers (CHWs) among low-income Hispanic/Latinos with diabetes and at risk for diabetes.
Methods
Using a quasi-experimental mixed method design, we assessed weight, glycosylated hemoglobin, diabetes knowledge, and behavior changes of Hispanic/Latinos participants with pre-diabetes and diabetes living in Southern California. Biometric measurements, blood tests, and surveys were collected at baseline and 3 months post-intervention. Interviews and focus group discussions provided qualitative data.
Results
Although the program was less costly, results exceeded those reported for low-income H/L attending the National Diabetes Prevention Program and did not differ between pre-diabetes and diabetes groups. Instead, including individuals at different stages of the dysglycemic spectrum seemed to have enhanced the intervention. Physician referral and attendance of family/friends were associated with better outcomes.
Conclusion
Our findings indicate that a joint prevention/self-management intervention led by CHWs for low-income Hispanic/Latinos with diabetes and with pre-diabetes is feasible and cost-effective, providing results that could help reduce the success gap. Incorporating suggestions and replicating this study on a larger scale could help determine whether or not results are reproducible.
Keywords
The currently available and widely promoted National Diabetes Prevention program and Diabetes Self-management Education and Support interventions, which accept individuals based on their diagnosis (pre-diabetes or diabetes, respectively), are less successful among low-income Latinos, and therefore may be contributing to an increase in the diabetes disparity gap in this population where basic survival and family support are paramount.
It provides evidence that a diabetes prevention and self-management intervention led by CHWs which promotes the same lifestyle changes among all family members at various levels of the dysglycemic spectrum is feasible and could provide better results and reduce diabetes disparities in low-income underserved Latinos communities.
Policies that support offering the same community health worker-led lifestyle intervention to all family members with abnormal glycemic levels, while addressing policy-driven social determinants of health (access to walk-able neighborhoods, affordable healthy food, and transportation), may result in a better return on investment among low-income Latinos communities since they have the potential of reducing the diabetes burden among those most affected by this condition.What do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications Towards Theory, Practice, or Policy?
The poor experience a disproportionate burden of diseases worldwide. 1 In the USA, where chronic diseases such as diabetes are inversely correlated with poverty and limited literacy,2,3 Hispanics/Latinos (H/L) earn less and have less formal education on average than non-Hispanic Whites (nHWs). 4 Not only are they more likely to develop diabetes they also experience worse complications.5-7
To reduce the health burden associated with type 2 diabetes,8,9 the Centers for Disease Control and Prevention 10 promote two different programs: one for individuals with pre-diabetes, and a separate one for those with diabetes. 11
The Diabetes Self-Management Education and Support (DSMES) program, for those with diabetes, consists of six to ten weekly meetings lasting two hours or less and is typically offered in clinical settings. Participants’ goals are customized. As for the National Diabetes Prevention Program (NDPP), a program offered to individuals with pre-diabetes, it is delivered in 12 months and usually held in community settings. 12 The latter is an adaptation of the Diabetes Prevention Program, a landmark intervention where 15.7% of the participants were H/L, mostly of high socio-economic status and literacy level.13,14 NDPP participants attend 16 one-hour-long weekly classes followed by monthly meetings and aim to lose 5% of their initial weight. Taught by diabetes educators or healthcare professionals, both programs promote healthy eating, exercise, self-monitoring, stress management, and problem-solving skills. Additionally, the DSMES promotes diabetes self-management (glucose monitoring, foot checking, regular physician visits, and proper medication use).
Evidence suggests that participants’ socio-economic status determines how much they will benefit from health promotion interventions.15,16 Some authors have even concluded that interventions focusing on individual behaviors increase inequality gaps proposing comprehensive and population-based policy interventions instead. 17
Both the NDPP and the DSMES programs, while evidence-based and reportedly successful overall, seem to have increased the inequality gap. 18 Not only do low-income H/L participants report challenges across both programs, 19 when compared to nHWs, they are less likely to enroll, 20 more likely to drop out if they enroll, and less likely to succeed despite accommodations (eg, eliminating cost and culturally adapting the material).21,22
A decade after the national launch of the NDPP, another challenge that threatens to further increase the diabetes health disparity gap 23 is selective lack of program funding: reimbursement to entities offering NDPP programs depends upon participants reaching the 5% weight loss threshold, a threshold rarely reached by low-income H/L programs. In our current crisis of ever-increasing diabetes and COVID-19 health disparities, this vulnerable population is in critical need of effective sustainable interventions.
It is generally accepted that social support improves adoption and retention of healthy behaviors regardless of cultural background, and there is clear evidence of the critical nature of family support for lifestyle changes in both diabetes prevention and self-management programs.24,25 In patients with diabetes, adopting a healthier lifestyle is a greater challenge than adhering to a medication regimen, and the impact of social support on specific behaviors varies.26,27 This is even more critical in collectivistic cultures such as the H/L culture, 28 with family members’ support, or lack of it, often cited as an important source of motivation or a barrier to making lifestyle changes.29-31
Lifestyle changes benefit individuals at all levels of the glycemic spectrum (blood glucose range from normal to diabetes levels) and family members of individuals with diabetes (those in either of the above-mentioned programs and those who do not qualify for either) often struggle with similar lifestyle-related risk factors and barriers. Thus, regardless of their location on the glycemic spectrum all could benefit from an intervention that facilitates lifestyle changes. A “family inclusive” approach is supported by the American Diabetes Association
32
but the reality is that individuals with diabetes and pre-diabetes rarely qualify to enroll in the same program: for example, the NDPP program only accepts those with pre-diabetes
1
and, although some DSMES programs accept individuals with pre-diabetes, not all do.
33
Therefore, the following could happen to an average family (as illustrated in Figure 1) - individuals with diabetes would attend the six- to eight-week diabetes self-management program, - family members with pre-diabetes would enroll in the NDPP and attend for one year, - Others—who may well be at risk of diabetes since having a first-degree relative (sibling or parent) with diabetes is a known predictor of diabetes development—would not qualify at all for either of these programs.
34
Potential scenario in a family with a family member diagnosed with diabetes.

Even if they all qualified for either of these programs, differences in sessions content and timing could exacerbate transportation and coordination challenges within the family unit.
It would therefore seem desirable and cost-effective to have one program delivered to all family members so they could benefit from mutual support for lifestyle changes. The concept of a “joint” program has been suggested and considered in the past, but concerns have been raised: fear of barriers between physicians and family members of patients with diabetes, the cost of involving family members in programs, and the challenge of keeping participants with pre-diabetes engaged.35-37 However, in view of recent healthcare system trends, there is reason to believe that these obstacles may be surmountable, if still present.
Physicians are using a more patient-centered approach, which is believed to enhance patient/caretaker-physician communication. 38 Community health workers (CHWs) are increasingly given important roles in both diabetes prevention and self-management interventions. They are being integrated at several levels of clinical care, 39 reducing costs, and improving results, especially among low-income populations. 40 Because CHWs capture low-income participants’ perspectives and barriers and specialize in addressing social determinants of health, they may be more effective at helping them surmount challenges. Furthermore, their ability—often through the use of a popular education approach—to keep individuals engaged in programs that would otherwise experience attrition, makes them a perfect fit for interventions focused on underserved populations.
In reviewing the literature, while there are multiple diabetes prevention or self-management interventions led by CHWs among low-income Latinos, the authors found a paucity of programs available and accessible to both H/L at high risk of diabetes and those with diabetes. 41 The few interventions that allowed family members of individuals with diabetes to join showed promising results but did not report weight changes nor diabetes status of family members.42,43 Thus, little is known about the feasibility and potential impact of a joint diabetes prevention program/intervention (ie, intervention for individuals at various levels of the dysglycemic spectrum) for low-income Hispanics/Latinos.
The purpose of this study was to explore the feasibility of implementing a CHW-led culturally sensitive lifestyle intervention for low-income H/L with diabetes (DM group) and H/L at risk of diabetes (NDM group). Besides weight and glycosylated hemoglobin (A1C), participants’ engagement, program cost, and impact of physician-patient/family interaction were assessed. In addition, participants were encouraged to share perceived barriers to attendance and behavior modification.
Methods
Setting and sampling procedures: This pilot mixed-method study was conducted among low-income H/L residing in the Inland Empire Region of Southern California, an area with one of the largest H/L populations in the US, many of whom lack health insurance coverage. It also has one of the highest rates of diabetes-related mortality in California.44,45
Program recruitment: Participants were contacted via flyers posted at community centers, through personal invitations from CHWs and at a clinic. Patients at risk of diabetes or with diabetes were encouraged by a culturally homologous Hispanic/Latino physician to enroll by adding their names to a sign-up sheet.
Program inclusion/exclusion criteria: For quantitative analyses, the inclusion criterion was “having attended at least 80% of the Vida Vibrante (Vibrante Life) Diabetes Prevention and Self-Management Intervention (VV).” Participants were excluded if they were unable/unwilling to answer the surveys.
Eligibility criteria for the qualitative portion included (1) having attended VV—to qualify for focus group discussions (FGDs); or (2) being a CHW who taught VV—to qualify for a key informant interview (KII). Focus group participants (N=33) were recruited from all cohorts immediately following program completion. CHWs (n=3) completed KIIs for triangulation reasons within 10 days of course completion.
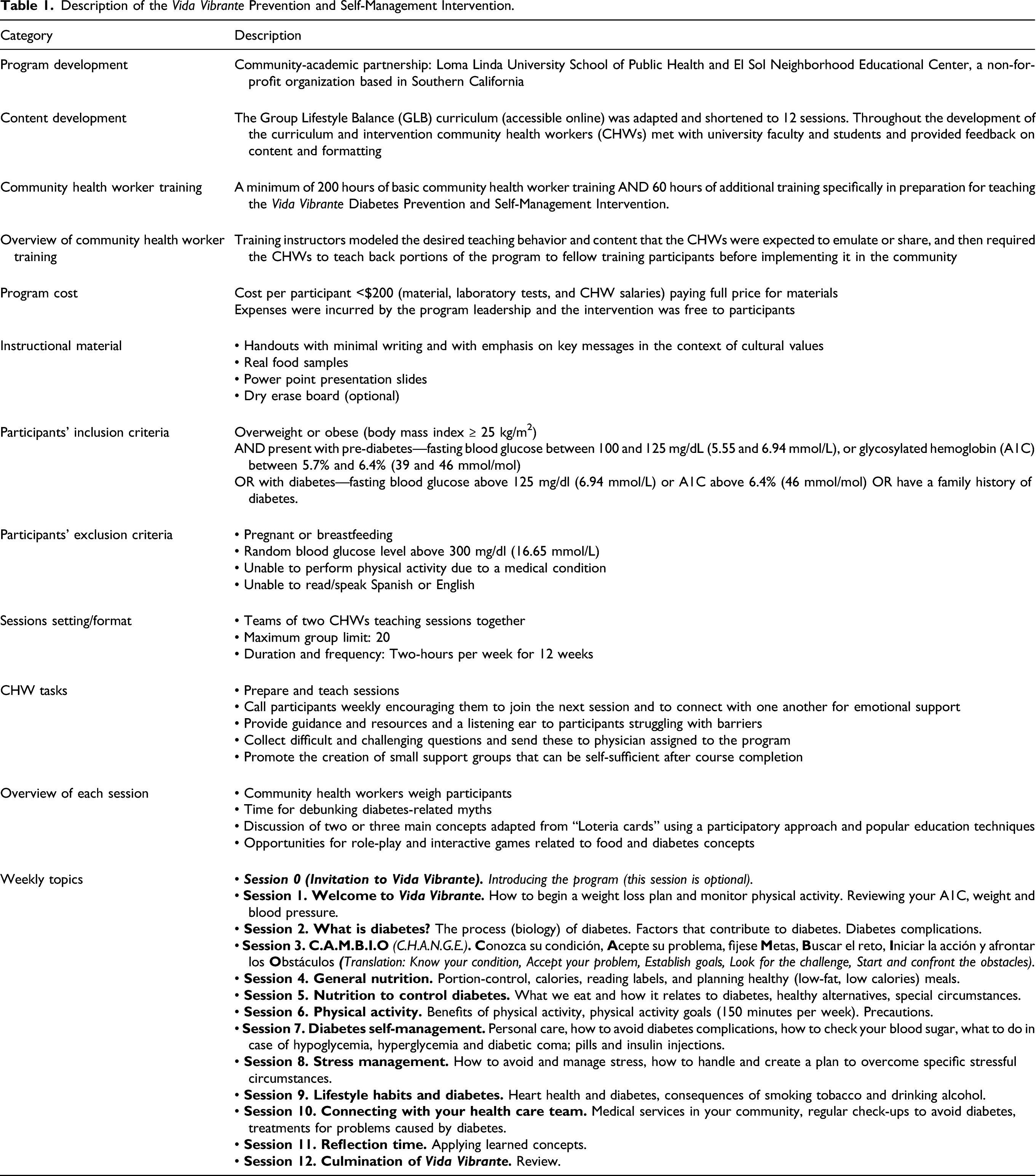
Vida Vibrante program description: The program content is a cultural adaptation of the Group Lifestyle Balance (GLB) curriculum (accessible online). 46 The core content of the GLB was consolidated to limit participant burden and program cost with the main content of the classes consisting of basic information about healthy eating, moderate physical activity, and diabetes. Key concepts were associated with Latino sayings and pictures adapted from “loteria” cards (used by permission of the New Mexico Department of Health Diabetes Control Program) 47 to facilitate understanding by a wider range of literacy levels.
Description of the Vida Vibrante Prevention and Self-Management Intervention.
Study procedures, measures, and data collection: The quantitative portion of the study used a non-equivalent comparison group design with dependent pre-test and three months’ post-test samples. CHWs recorded participants’ height and weight, and participants completed self-report surveys at baseline and immediately following the intervention. Average blood glucose level over the past 3 months (A1C) was determined from a finger prick. Questionnaires, which included basic demographic information, diabetes status, recruitment type (clinic or community), diabetes knowledge questions, and whether or not family or friends attended, were available in English and Spanish.
Variables used to assess average blood glucose, biometric measurements and self-reported data.
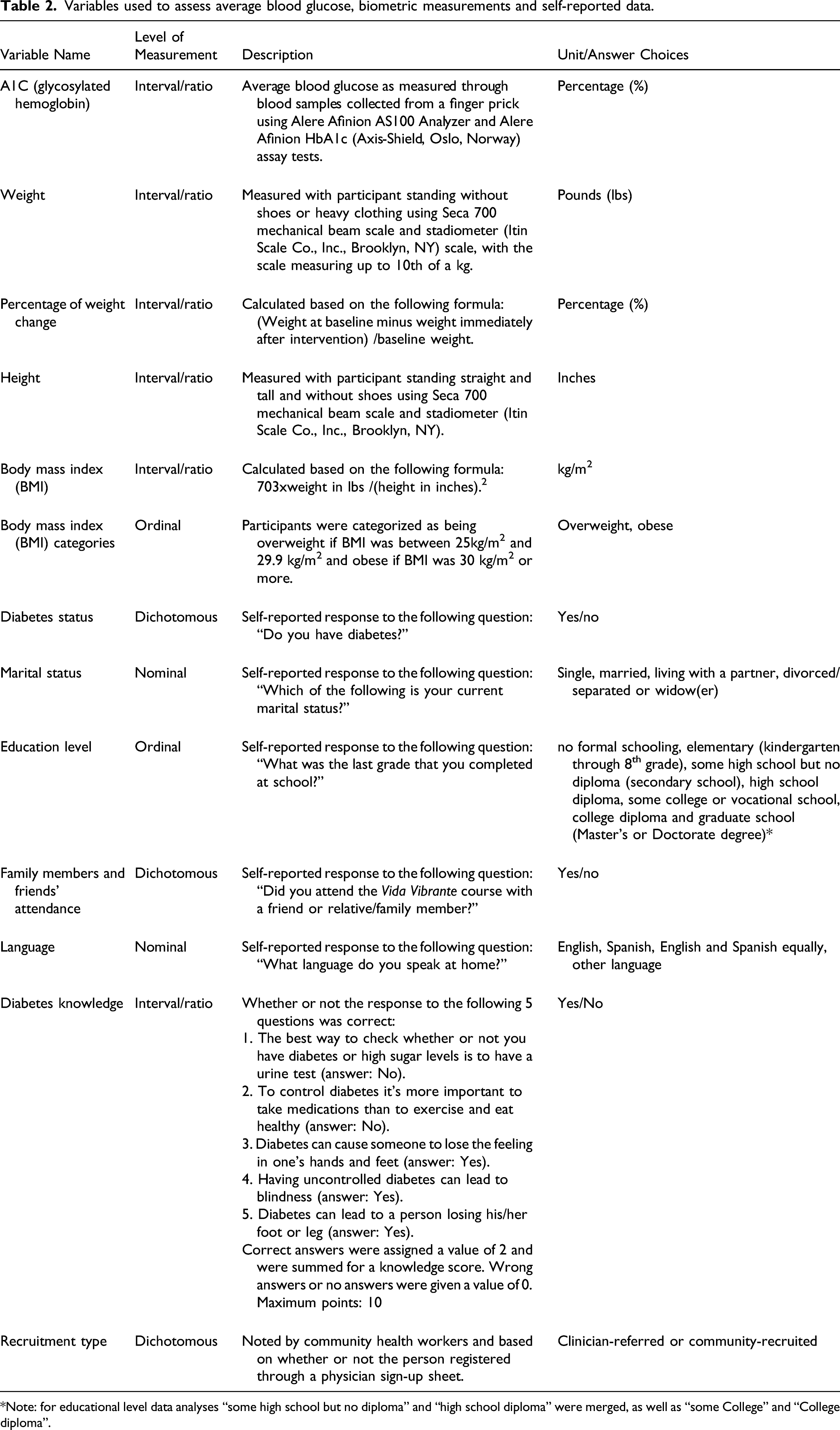
*Note: for educational level data analyses “some high school but no diploma” and “high school diploma” were merged, as well as “some College” and “College diploma”.
For the qualitative data collection, nine FGDs, each consisting of three to seven program participants, and three KIIs (with CHWs who taught), all lasting between 15 and 55 minutes, were conducted in Spanish by three trained bilingual interviewers (researchers) at two community centers upon program completion. Non-completers were also invited to provide feedback but did not. The semi-structured interview guides for the KIIs and FGDs were created based on Charmaz’s (2006) grounded theory approach 48 using a social determinants of health perspective. Questions encouraged participants to share perceived barriers to healthy behaviors and attendance. Participants were also asked to share changes they experienced since program enrollment, perceived impact of fellow attendees with a different diagnosis on their attendance and success, and about interaction with their physician (or the physician of a family member with diabetes). Probes were used to expand the exploration and allow new issues to be identified.
Data analyses: Quantitative data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 22. The primary outcome was change in weight. Chi-square tests were used to assess baseline differences between gender, diabetes status, recruitment setting (physician-referred or community-recruited), and family and friends’ (FF) attendance. An independent t (or Mann–Whitney) test was performed to evaluate weight, A1C and knowledge differences between groups, and sample paired t (or Wilcoxon) tests assessed pre- and post-changes. Data were inspected for outliers and inconsistencies before analyses.
FGDs and KIIs were audio-taped with the participants’ permission and transcribed verbatim by bilingual individuals. The transcripts were then analyzed for emergent themes supported by critical quotes using the 2017 computer software program MaxQDA® (v.12, Berlin, GDR) 49 to code the transcripts, using an a priori code book but allowing for new codes to emerge. A team of three research assistants developed the codebook which was later expanded as emergent themes were identified and organized. Analyses were conducted in Spanish, and relevant quotes were translated prior to inclusion in this manuscript.
Results
Participants’ baseline characteristics.

*Statistically significant differences between groups at baseline, p<.05.
a. Sensitivity analyses (only those with baseline A1C³5.7%).
b. BMI = Body mass index.
c. MD = Physician.
Between-and within-group differences at baseline and at 3-months follow-up.
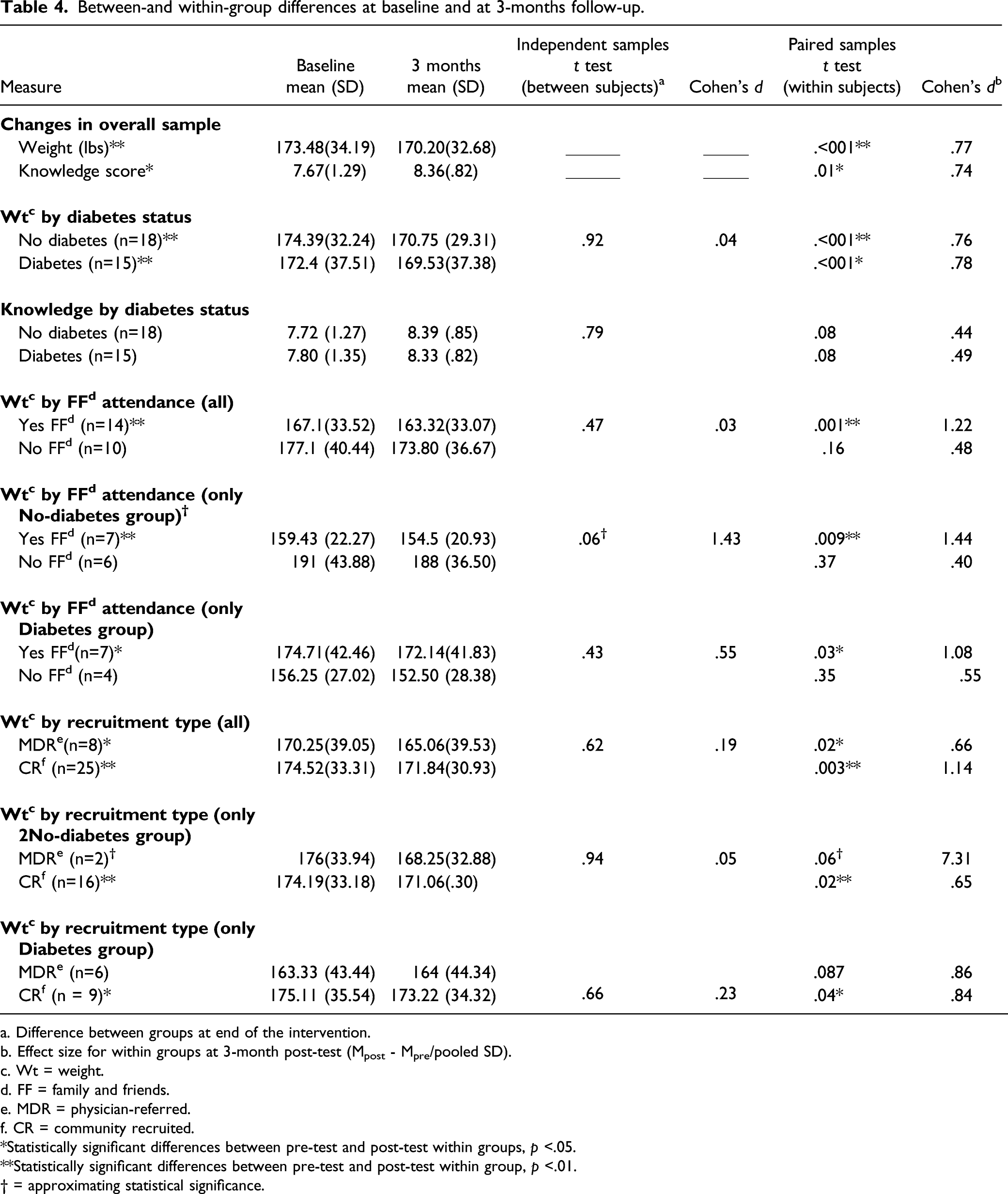
a. Difference between groups at end of the intervention.
b. Effect size for within groups at 3-month post-test (Mpost - Mpre/pooled SD).
c. Wt = weight.
d. FF = family and friends.
e. MDR = physician-referred.
f. CR = community recruited.
*Statistically significant differences between pre-test and post-test within groups, p <.05.
**Statistically significant differences between pre-test and post-test within group, p <.01.
† = approximating statistical significance.
Intervention effects—overall study sample: Weight loss—which ranged from 1 to 18 lbs—and improvement in diabetes knowledge were statistically significant (p<.001 and p=.01, respectively). Average weight loss was 3.29 (±4.26) lbs and had a large effect size (Cohen’s d=0.77). Among those with an abnormal baseline A1C (≥ 5.7%), there was a non-statistically significant trend towards improvement (p=.28) from 7.2% (±1.8) to 6.95% (±.48).
Intervention effects based on diabetes diagnosis: Weight loss average for the NDM group was 2.87 (±3.66) lbs or 1.69% (±2.24) of initial weight, whereas DM group participants lost on average 3.65 (±4.78) lbs or 1.91% (±2.31) of their initial weight. But group differences were not statistically significant (p =.92). Besides statistical significance (p<.001), weight loss effect sizes were large (Cohen’s d=.77 and .78). Figure 2 displays relative weight loss among participants based on certain characteristics. Improvements in diabetes knowledge and A1C within the NDM or the DM groups were non-statistically significant and did not differ between groups. Percentage of weight loss at program completion based on certain characteristics.
After determining pre-post changes within the DM and the NDM group, the authors explored the impact of family/friends’ attendance (also social support) and recruitment type.
Intervention effects based on family and friends’ attendance: Overall, individuals who attended with friends and family had a statistically significant weight loss of 3.75(±3.08) lbs (p=.001) with a large effect size (Cohen’s d = 1.22), while participants who attended with no friends or family members experienced a non-statistically significant weight loss (p=.16). This translates to losing 2.26% (±1.85) and 1.60% (±3.40) of their initial weight, respectively. Group differences were statistically significant (P =.06). Even within each group (NDM or DM) weight loss was only statistically significant among those whose family and friends attended. Effect sizes were large (Cohen’s d= 1.44 and 1.08, respectively).
Intervention effects based on recruitment type: Both the physician-referred group and the community-recruited group experienced a statistically significant weight loss. Although the former lost nearly twice the weight as the latter (5.19±4.54 lbs, p=.01 vs 2.68 ±4.88 lbs, p=.003)—a weight loss which translates to 3.17% (±2.88) and 1.38% (±1.86) of the initial weight, respectively—effect size was larger for community-recruited participants (Cohen’s d=1.14 vs .66). When analyzing weight loss by recruitment type within each group (NDM or DM), weight loss within the DM group was only statistically significant for the community-recruited group. As for the NDM group, weight loss was also statistically significant for community-recruited participants but only marginally statistically significant for physician-referred participants.
Themes derived from key informant interviews and focus group discussions.

NDM = participant with no diabetes. DM = participant with diabetes. All quotes were transcribed in Spanish and then translated. The three CHWs who taught the intervention were interviewed for the key informant interviews (KIIs). Focus group discussions (FGDs) were conducted with program participants (n=33). Unless followed by “KII”, quotes are all taken from FGDs statements.
Discussion
This study sought to explore whether a joint diabetes prevention and self-management intervention—for individuals with diabetes and those at risk for diabetes—could benefit low-income H/L with limited education and reduce the success gap between them and other populations known to respond better to lifestyle interventions.
Because of previously expressed concerns about such an endeavor being too costly, lack of interest among those with no diabetes and strained physician/family members relationships, the authors also assessed the impact of physician involvement and cost of implementing such program. We also sought to assess if the presence of participants with diabetes discouraged engagement from others without diabetes.
While enrollment of H/L in interventions has historically been low (a number that varies depending on source and setting)27,50 most classes were filled to capacity in our study. Trust has been cited as the most important factor in enrollment and we believe that recruitment by a trusted physician and/or community health worker in this study was a key factor. 51
According to our findings, H/L of low to medium educational level could indeed benefit from a “joint” program, regardless of their location on the dysglycemic spectrum, especially if attending with family or friends and when there is physician engagement. Overall, our study sample benefited from the intervention in that participants lost weight, increased their diabetes knowledge, had a trend towards A1C improvement, and adopted healthy behaviors. Approximately half of all participants lost at least 2.2 lbs at 12 weeks (program completion), a clinically significant weight loss.
Social support is known to play an important role in promoting healthy behavior. In our study sample, a higher proportion (57%) of those attending with family or friends reached clinically significant weight loss compared to those who attended with neither (30%), suggesting that having a family or friend was helpful. Due to survey limitations, it was not possible to differentiate those who attended with family from those attending with friends in the quantitative analyses; however, during the FGDs, several individuals with diabetes identified relatives who attended the course with them, and participants from both categories stated that the presence of friends and/or family members helped motivate them to engage in healthy behaviors. Weight loss differences were even greater when comparing clinician-referred and community-recruited participants (75% vs 40%, respectively), suggesting a positive correlation with physician engagement.
A1C sensitivity analyses showed a trend towards improvement but these changes were not statistically significant in the overall group nor within each of the groups. We believe this is because changes in nutrition and physical activity were not started until the fifth session, therefore allowing less than 8 weeks for A1C to reflect glucose improvement. 52 Furthermore, the relatively low group baseline average A1C level and the small sample size may have played a role.
When comparing groups with and without diabetes both groups lost weight and no statistically significant group differences were detected. Among the DM group, 53.3% had a clinically significant weight loss, thus reducing their risk of cardiovascular disease by at least 4 to 8%.53,54 Weight reduction in this group (2.87±3.66 lbs) was comparable to that reported in a 12 week study implemented among H/L adults with diabetes (n=34) living in the same geographical area as this study’s participants (2.07 lbs). 55
Among the NDM group, 44.4% lost clinically significant weight which translates to at least a 16% diabetes risk reduction. 56 Diabetes knowledge in this group increased as much as that of the DM group, suggesting similar engagement, since knowledge increase is a good reflection of engagement. 57 Indeed, judging from their diabetes knowledge, attendance and qualitative statements at program completion, the NDM group seems to have benefited from exposure to the DM groups. Higher attendance rates in the NDPP and other interventions have been associated with improved results. 58 Our results also indicate that family and friends attending improve success rates within both NDM and DM groups.
While most diabetes-related reports describe either diabetes prevention or self-management, two studies reported the results of interventions delivered to H/L individuals at varying levels of the glycemic spectrum. In one study where most participants were from Mexico, each person with diabetes enrolled with a family member with no diabetes. The eight week intervention was taught by nurses. 42 Attrition and knowledge changes were similar among participants with and without diabetes and there was a statistically significant decrease in A1C 10 weeks after baseline. However, weight changes were not reported. Another study conducted among Mexican American dyads (one participant with diabetes and a family member without diabetes) used a 12 week DSME/S intervention led by a nurse diabetes educator and a CHW (only for the social aspect and to make phone calls). Only changes among participants with diabetes were reported and A1C improvement was not statistically significant. 43
The VV intervention was unique in that it encouraged participants to develop a new social network (support group) within the larger group and was intended to promote weight loss and behavior change equally in both participants groups, rather than having family members focus on supporting another “sick” family member. It also differed from the above-mentioned studies in that it was CHW-led. We also assessed and reported weight changes in different subgroups.
Although concerns have been raised about family members-physician interaction, we were unable to identify—quantitatively or qualitatively—any ongoing communication barriers between physicians and patients’ family members. An article on the NDPP reported less physician referrals of monolingual Spanish-speaking to prevention programs (compared to those who spoke English).18,21 However, upon examining retention, engagement, and results of physician-referred participants in VV, they seem to have benefited more: not only was the percentage of weight loss among those recruited by a physician close to double that of the community-recruited group, the weight loss (3.17% ±2.88 at 12 weeks) was somewhat comparable to the average for non-Latinos NDPP participants (a dose response of .30% per session attended and 3.4±3.61% of initial weight lost at 16 weeks). VV participants’ results were also better than results from a recent NDPP report among mostly Latinas in Los Angeles, California (2.15% at 16 weeks).18,59,60 Whether or not the difference is due to characteristics of providers, of those who visit their physicians, or of patients’ family members is beyond the scope of this study. Certainly, the role of clinicians has been noted as a powerful motivator for healthy behavior in H/L culture, 61 especially among monolingual Spanish-speaking Latinos. 28
While quantitative data showed some advantage among physician-referred participants qualitative data revealed that physician-patient interactions are more complex. It was obvious that participants preferred using alternative medication and that some felt the need to justify seeking medical help. There was skepticism about traditional medicine as practiced in the USA, and a reluctance to spend time caring for oneself. Some went as far as to state that they may not pay attention to their physician unless he/she engages them actively in the decision-making process. Thus, referral from a physician would not, in and of itself, motivate these participants to adopt new lifestyle habits in the absence of a positive physician-patient interaction. Nevertheless, our study suggests that healthcare providers can have a positive influence on low-income at-risk H/L individuals and may promote more permanent results if they make referrals to diabetes prevention and self-management programs a priority.
In addition to their hesitation to seek medical care, H/L have the highest uninsured rates (32%), 62 making early diagnosis of asymptomatic conditions such as pre-diabetes a challenge. Moreover, despite recent interest in Family DSMES programs, 35 these interventions target individuals with diabetes, and requirements are more stringent than those in our study. Allowing for a mixed program approach would facilitate the process of addressing the needs of two important and potentially costly groups. Clearly, the benefits of interventions for low-income H/L would provide a wider net to “catch” individuals who would otherwise never be screened or served before they develop the disease.
A program such as VV could offer an option for many more individuals desperately needing the support of an intervention, especially in view of the program’s relatively low cost. The cost incurred for each participant of this 12 week intervention was a little under $200, which seems competitive when compared with the cost of the NDPP intensive first 16 weeks (between $500 and $800 per person).63,64 We posit that engaging CHWs to implement a shorter “hybrid” diabetes intervention, similar to “family therapy,” may be financially viable and a worthwhile return on investment, especially considering that a minimum of $14,000 can be saved per person for each year of delay in diabetes onset. 65
The focus group and KII participants corroborated the existence of several policy-related “barriers” to enrollment and behavior modification previously identified by other studies: lack of transportation, limited access to healthy food options, and lack of safe environments for physical activity. Less access to healthy food and safe places to exercise, and fewer transportation options are all known to be associated with poor neighborhoods. Other factors associated with less attendance and success were male gender, financial constraints, little time and energy due to long work hours, and family resistance to change. Men were a minority in this study and did not participate in the FGDs; however, according to available literature, men tend to generally attend lifestyle programs less frequently. 66
Strengths and limitations: Several limitations of this study need to be acknowledged. Since this was a pilot feasibility study, our sample size was small. Participants were mostly women of Mexican descent; furthermore, although it was obvious from the focus group statements that the great majority of participants had financial challenges, we could not confirm participants’ income. In addition, whether referral from a non-Hispanic/Latino physician would produce similar effects as that of a cultural homologous physician could not be ascertained. Thus, applicability to other low-income H/L may be limited. This program allowed family and friends to attend, with no differentiation between categories. Also, because our design did not allow us to dismantle our data to gather that information, we were unable to determine whether or not individuals who did not attend with friends and family lived alone or had any family members at all. The subcategories and differences in circumstances could have affected social support and should be explored in future studies.
One strength of this study is that we were able to compare two groups attending the same program taught by CHWs. Other strengths included having qualitative data confirm and further contextualize quantitative data (e.g., participants describing behavior changes and attendance of friends) and CHWs corroborating participants’ statements. Lastly, access to physician-referred participants allowed the authors to assess the impact of collaboration between clinicians, CHWs, and program development specialists.
Conclusions and Implications for Practice
There is an urgent need for effective, sustainable diabetes prevention, and self-management programs that are well attended by, and effective for, low-income H/L. Unless the current trends reverse, the continued lack of success of nationally promoted interventions among low-income H/L threatens to increase the diabetes health disparities in this population and in the country. Our findings show that both groups were engaged to the same degree and benefited equally from a joint program led by community health workers. Furthermore, the presence of family and friends, and referral from a physician improved results, showing the promise of closing the H/L success gap.
Rather than accommodating the shorter DSMES program for low-income H/L at risk of diabetes, or “forcing” participants to commit to a 1 year diabetes prevention program—when most H/L attend less than eight times even when they do not have to pay for the program—our results indicate that a “hybrid” shorter program offered to both groups may be worth considering, especially if it includes members of the same social network. A combined program may have the advantage of providing everyone within the dysglycemic spectrum with social support, a critical component in promoting success. Moreover, this would avoid duplication and help create a more unified message regarding the behaviors required to achieve glycemic control.
Finally, the results indicated that CHWs can successfully lead a “diabetes prevention and self-management intervention,” even in the presence of barriers associated with policies. Furthermore, as an integral part of programming, they may even compensate for the often less-than-ideal physician-patient interactions inherent in our healthcare system.
On a broader policy-making level, reducing barriers should be a high priority: providing incentives to physicians and reimbursement for CHW-led, culturally relevant lifestyle-based interventions, allowing family members and friends to attend, increasing access to healthy food and reliable transportation, and creating safer “walkable” communities in H/L neighborhoods. Programs should also be available year-round to facilitate enrollment shortly after referral. 66
Community/healthcare system partnerships which combine “hybrid” culturally sensitive CHW-led lifestyle-based diabetes prevention programs with supportive healthcare entities and progressive policies have the potential of dramatically reducing the risk of diabetes and diabetes complications, among those most afflicted in the Hispanic/Latino communities.
This study expands the literature by providing viable cost-effective options to health educators, healthcare professionals, and policymakers seeking to address the US health disparities and the diabetes burden among the most vulnerable. Replication of this study on a larger scale and extended for a longer time period (a year) may help confirm our findings and provide guidance to policymakers as our nation struggles to reduce health disparities among those bearing the heaviest burden of chronic diseases.
Footnotes
Acknowledgments
First of all, many thanks to community health workers Monica Acevedo, Beatriz Castro, Vanessa Rivera, Miriam Valero, Lidia Benitez, Juandretta Hern and Erika Marroquin who implemented the intervention, and to our community partner and Executive Director at El Sol Neighborhood Educational Center, Alex Fajardo. We are also grateful to Dr Toni Fernandez of Hesperia Clínica Médica Familiar, Dr Marino De Leon, Director of the Loma Linda University Center for Health Disparities and Molecular Medicine and Dr Eddy Jara from Loma Linda University School of Public Health. Lastly, we’d like to thank Noemi Avalos, Jessica Camacho, Suhail Hashim, Maria Anaya, Kelsy Escalante and Lily Lee who assisted with curriculum editing, training, recruiting, data analyses and interviews.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was partially funded by El Sol Neighborhood Educational Center, Loma Linda University Behavioral Health Institute and the National Institute on Minority Health and Health Disparities of the National Institutes of Health under award number P20MD006988.
Ethical Approval
All program participants provided written informed consent in Spanish or English, as approved by the Loma Linda University Institutional Review Board (#5150145), the same board that approved this study.