
Abstract
Medical misinformation (MM) is a problem for both medical practitioners and patients in the 21st century. Medical practitioners have anecdotally reported encounters with patient-held misinformation, but to date we lack evidence that quantifies this phenomenon. We surveyed licensed practitioners in the state of North Carolina to better understand how often patients mention MM in the clinical setting, and if medical practitioners are trained to engage with patients in these specific conversations. We administered an anonymous, online survey to physicians and physician assistants licensed to practice in the state of North Carolina. Questions focused on demographics, clinical encounters with MM, and training to discuss MM with patients. We received over 2800 responses and analyzed 2183 after removing ineligible responses. Our results showed that most respondents encountered MM from patients (94.2% (2047/2183)), with no significant differences between clinical specialty, time spent in practice, or community type. When asked about specific training, 18% (380/2081) reported formal experiences and 39% (807/289) reported informal experiences. MM has been salient due to the COVID-19 pandemic; however, it was present before and will remain after the pandemic. Given that MM is widespread but practitioners lack training on engaging patients in these conversations, a sustained effort to specifically train current and future practitioners on how to engage patients about MM would be an important step toward mitigating the spread of MM.
Keywords
Introduction
With access to the internet available in many pockets and purses, the spread of information throughout the world has never been faster or easier. 1 This is also true for misinformation or information that is demonstrably false in comparison to scientific consensus but which may have been shared with or without an intent to deceive others. 2 Misinformation is present in many arenas, including discussion of politics, environmental issues, and health care; when it occurs in connection with health, health care, or medicine, we can refer to the phenomenon as medical misinformation (MM). MM may also be called health-related misinformation. 3 The onset of the COVID-19 pandemic has heightened the public salience of MM. This was evident not only in news headlines 4 but also in commentary and perspective pieces in scientific journals.5,6 The consequences of MM pose challenges for both patients and the overall public, which is especially prominent in public knowledge of vaccines, statins, and the COVID-19 pandemic.7-9
Social science has responded to misinformation in various ways, such as monitoring inaccurate claims in media outlets2,10 or studying misperception correction.11,12 Regarding MM specifically, Wang et al. recently published a systematic review focusing on the spread of health-related misinformation through social media, 3 and Kouzy et al. analyzed specific tweets on COVID-19 to track misinformation on the pandemic. 13 In addition to peer-reviewed literature, we can point to anecdotal reports and small sample studies of practitioner concern about MM, and encouragement for health care professionals to engage with patients on this topic now appears in a variety of sources.14-23
Despite this attention to MM, we have been unable to find sufficient population-level evidence of how often medical practitioners encounter MM directly from patients in while clinical settings. We also do not know the extent to which clinicians have received training to engage patients in conversations regarding misinformation, such as lectures, webinars, workshops, or informal advice from mentors. Available literature largely has not reported on clinician preparation for such situations. To obtain baseline data for how often MM is a factor in practitioner–patient exchanges, we surveyed practitioners licensed with a state medical board in North Carolina, USA. North Carolina is a diverse state on many levels. Geographically, residents live in mountain, coastal, or piedmont regions. In these regions, rural, urban, or suburban communities are found. The medical workforce of North Carolina is also diverse, not only across specialties but also among the different types of practitioners: physicians, physician assistants (PAs), nurses, nurse practitioners, pharmacists, etc. All of these practitioners speak with patients on a daily basis. For these reasons, North Carolina serves as an excellent microcosm to examine the exchange of MM between patients and practitioners.
The goal of this pilot study is to contribute data in the growing MM field on the following 3 questions: (1) Do licensed practitioners experience MM from patients in the clinical setting? (2) What types of MM do patients raise in the clinical setting? (3) Are licensed practitioners adequately trained to engage patients in conversations specifically about MM?
Methods
We created an anonymous, online survey to assess frequency and content of MM encounters, as well as training among physicians and PAs (herein referred to collectively as practitioners). In the survey, we defined MM as “information that is factually inaccurate or not supported by current evidence-based medical literature and/or practices.” The survey was comprised of 22 questions to gauge how long participants had been in practice, the type of community in which they practice, and field of specialty (Supplementary Appendix 1). Questions relating to practitioner experience with MM were based on respondents’ own perceptions and recall. Practitioners in the Duke Academy for Health Professions Education and Academic Development initially assessed survey usability and functionality prior to fielding with our target population. We received permission to administer the survey to all licensed practitioners in the state of North Carolina from the North Carolina Medical Board (NCMB) and contacted practitioners via email. Duke University School of Medicine staff administered the survey over 3 weeks in May 2020 using RedCap. The Duke Health Institutional Review Board designated the survey as exempted research. Practitioners voluntarily submitted complete or partially complete responses. No compensation was provided, and responses were de-identified for analysis.
We analyzed data from eligible responses in a χ2 test to compare patterns of MM encounters. (We also attempted Fisher’s exact test for appropriate comparisons, but that test was computationally intensive and did not converge in a reasonable timeframe. This was due to the large number of specialty categories being compared.) In addition, for all participants combined, we computed the proportion and 95% confidence interval 14 for those who reported an encounter with MM and for those who received formal or informal training to address patient MM as a way of comparing frequency of encounters with MM and training experiences. We reported survey results in accordance with the Checklist for Reporting Results of Internet E-Surveys. 15
Results
We received 2889 unique responses. We removed largely incomplete responses and responses from practitioners not currently practicing in North Carolina, which left 2183 responses to analyze. The response rate was 8.9% (2183/24 571).
Frequency of Practitioner Encounters with Patient Medical Misinformation by Topic.

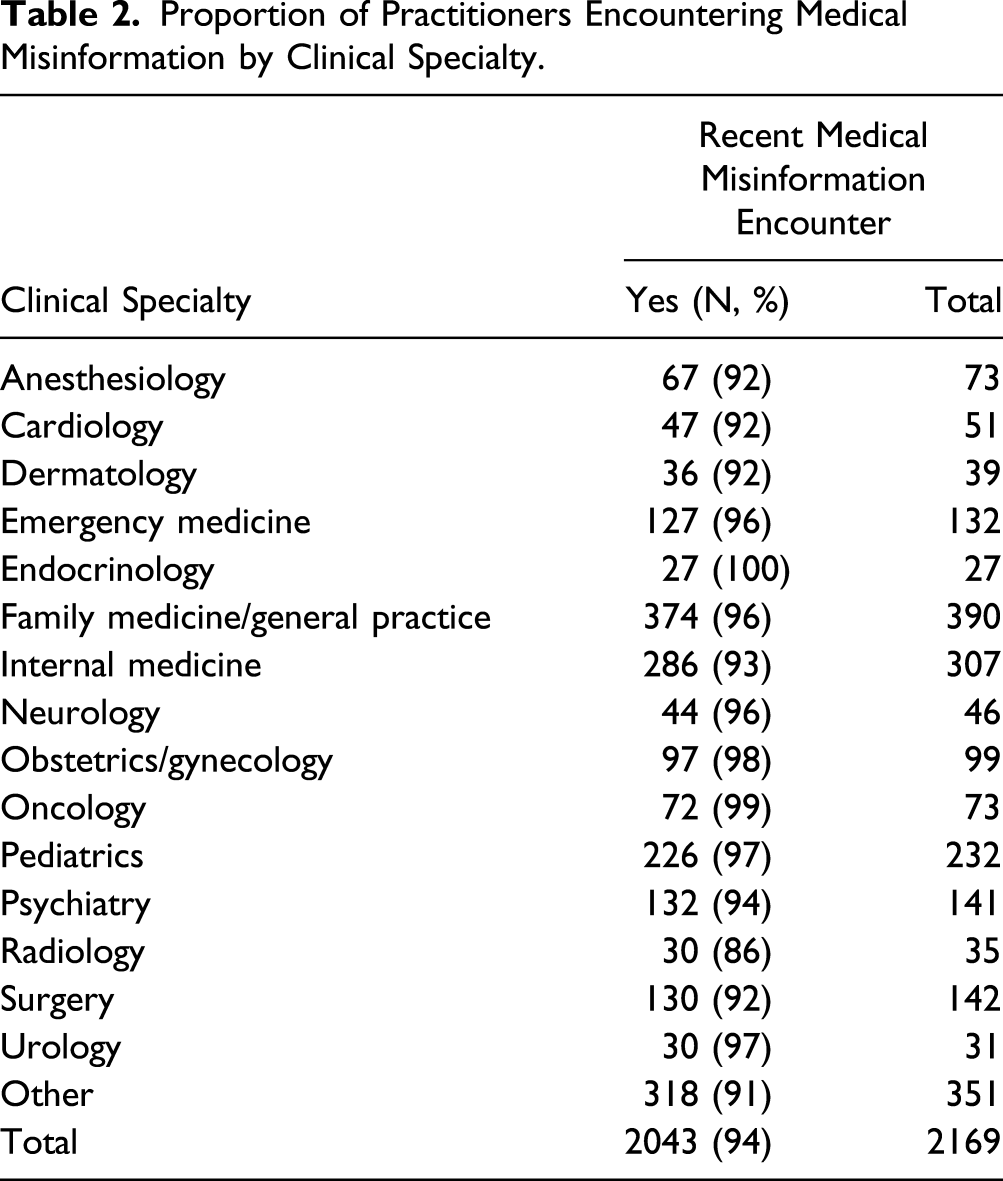
Proportion of Practitioners Encountering Medical Misinformation by Clinical Specialty.
Proportion of Practitioners Encountering Medical Misinformation by Training Type.

Discussion
We sought to assess if North Carolina medical practitioners encounter MM from patients in the clinical setting. Results show this was the case: such experience is almost universal among our respondents, with 94.2% reporting encounters with patient MM within the previous year. We provided our respondents with several broad topics and asked them to recall if patients referred to inaccurate medical information on these topics. We chose our specific topics based on a combination of factors. In May 2020, we wanted to assess how often practitioners were hearing misinformation regarding COVID given its status as a new disease. A long and documented history of vaccine misinformation exists,16,17 and misinformation regarding statins has been rising based on anecdotal reports from physicians. 18 Finally, the use of complementary and alternative medicine (CAM) by patients is well-established in the United States and other countries,24,25 and the approach of integrative medicine combines conventional medicine with complementary therapies. 24 However, the evidence supporting CAM treatments is often not as strong as that for conventional treatments due to several inherent challenges with researching CAM. 25 These include, but are not limited to, participant bias in clinical trials, 26 distinguishing therapeutic vs placebo effects,25,26 a lack of supporting pilot data, 27 and the association of CAM treatments with non-specific effects, such as the provider–patient relationship. 25 This lag in evidence-based efficacy may serve as a breeding ground for misinformation about the effectiveness of CAM treatments. 28
The topic of vaccines had the most frequent recollection of misinformation among our respondents. This may reflect either the strong roots that vaccine misinformation has in the United States, the large number of family medicine and pediatric practitioners that responded to our survey, or a combination of both. Given that our survey was administered in May of 2020 and asked for recollections of MM within the previous year, it is unlikely that misinformation related to the COVID-19 vaccines was the prominent source.
We were interested to see the diversity of specialties represented in our respondents (Table 2) and the universal agreement regarding reported encounters with MM. Because this is a pilot study, we cannot provide a valid statistical test of significance to say the reported percentage of those who encounter MM than those who do not is significant, but our data clearly show those who do report it is greater than those who do not. A larger study would likely provide enough data to determine statistical significance on this issue. The proliferation of MM has become more well-known as a problem in the medical field in recent years. However, we are not aware of any studies that attempt to distinguish if different specialties of practice are subject to different types of MM. This would be an interesting area for follow-up studies as it could inform potential training avenues. For example, suppose multiple departments in an academic medical facility would like to create a webinar focused on MM. Such a webinar can cover general considerations, but specific examples would likely be more effective for each department. For example, the cardiology group is likely to see more examples of MM related to statin use than the neurology group.
Finally, we wanted to know if respondents received training, either formal education or informal instruction, on addressing MM. Licensed medical practitioners typically have 2 distinct components of their education: formal instruction, as found in typical classrooms, and informal instruction, as in the form of advice or observations from senior mentors in hand-on practice. Although most respondents encountered MM with patients, only a small minority received training on how to engage patients in this context (Table 3). More respondents indicated that they received education about MM during informal instruction. This finding could be due to the direct interactions with patients in these settings. While “learning by doing” with senior practitioners, patients may bring up MM, providing the opportunity for discussion between a trainer and trainee.
As Trethewey et al. 19 noted in a survey of UK-based primary care providers, patients show a high level of interest in online health information. Given the high number of reported encounters with MM in our study, our results offer resonant evidence. We are not aware of any other studies that show to what extent medical practitioners have been trained to discuss MM with patients.
Sturgill 20 provides an excellent summary of the fraught information environment patients encounter. Many patients may have difficulty navigating the sheer volume of health-related information due to poor health literacy, but this online landscape is complicated by biased search algorithms, confirmation bias, politics, and intentional spread of disinformation. As Trethewey et al. and Sturgill19,20 have both noted, health care practitioners have the unique opportunity to direct patients to high quality, evidence-based medical information. Wu and McCormick 21 write that practitioners have a professional obligation to correct patient-held MM due to the combination of scientific training and licensure to practice medicine. We have shown that patients do in fact discuss MM in the clinical encounter. When we add this to the data from Kouzy et al. 13 showing that the highest levels of COVID misinformation in tweets were from informal personal/group accounts, this strengthens the argument that the process of mitigating MM calls for a focus on patient–provider encounters.
Patients likely believe MM for a variety of reasons, but one critical factor may be their need for hope, 29 particularly in dire medical circumstances. If medical practitioners, current and future, are only trained in strict evidence-based methods without knowing tactics to discuss MM with patients, the potential for patient confusion and mistrust between patients and practitioners may only grow. We believe focused training on MM must include an historical perspective on misinformation and a summary of patient psychology, coupled with practical application. As educators, we also advocate the incorporation of MM awareness into undergraduate medical education and in other health professions training, which can be easily done with standardized patient scenarios.
Limitations
Our results are limited by our response rate, which mirrored that of many mail surveys but nonetheless reflected a small minority of licensed practitioners in the state. That may be due to several factors. Our contact list was obtained from the NCMB, which regulates the licensing of practitioners in North Carolina. Many large medical facilities use administrative staff to process these requirements for their practitioners, so our survey invitations did not reach some of our intended recipients. A second factor is participant bias regarding the subject as interest in the subject matter might have predisposed practitioner participation. We note, however, that the respondent pool included practitioners from across the state representing a wide range of clinical specialties. We were also limited by the lack of standard MM definition by licensing medical boards or academic medical societies and provided our own definition of the concept for respondents. Finally, our survey was administered in May of 2020, in midst of the COVID-19 statewide lockdown in North Carolina. We believe many of our intended recipients were significantly engaged with matters related to telehealth and additional lifestyle adjustments the lockdown required.
Conclusions
Medical misinformation predates the COVID-19 pandemic and will persist after its resolution. As health care practices undergo a shift toward value-based care, our health care practitioners are in excellent positions to serve as bridges between scientists and laypersons. Their extensive training, grounded in the basic science of the body, combined with communication techniques focused on empathy and active listening could make them an ideal ally in addressing MM held by patients. Because sources of misinformation, such as internet and social media sites, are not going away, specific training on the context of misinformation is necessary. With a stronger background on the topic, practitioners should be more likely to engage in meaningful conversations with their patients and further strengthen the trust in their relationships.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580211035742 – Supplemental Material for A Pilot Study of Medical Misinformation Perceptions and Training Among Practitioners in North Carolina (USA)
Supplemental Material, sj-pdf-1-inq-10.1177_00469580211035742 for A Pilot Study of Medical Misinformation Perceptions and Training Among Practitioners in North Carolina (USA) by Jamie L. Wood, Grace Y. Lee, Sandra S. Stinnett and Brian G. Southwell in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Our complete survey is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.