
Abstract
Critical care is a costly and finite resource that provides the ability to manage patients with life-threatening illnesses in the most advanced forms available. However, not every condition benefits from critical care. There are unrecoverable health states in which it should not be used to perpetuate. Such situations are considered futile. The determination of medical futility remains controversial. In this study we describe the length of stay (LOS), cost, and long-term outcomes of 12 cases considered futile and that have been or were considered for adjudication by Ontario’s Consent and Capacity Board (CBB). A chart review was undertaken to identify patients admitted to the Intensive Care Unit (ICU), whose care was deemed futile and cases were considered for, or brought before the CCB. Costs for each of these admissions were determined using the case-costing system of The Ottawa Hospital Data Warehouse. All 12 patients identified had a LOS of greater than 4 months (range: 122-704 days) and a median age 83.5 years. Seven patients died in hospital, while 5 were transferred to long term or acute care facilities. All patients ultimately died without returning to independent living situations. The total cost of care for these 12 patients was $7 897 557.85 (mean: $658 129.82). There is a significant economic cost of providing resource-intensive critical care to patients in which these treatments are considered futile. Clinicians should carefully consider the allocation of finite critical care resources in order to utilize them in a way that most benefits patients.
As decisions to prolong the lives of critical care patients who are unlikely to recover are known to cause disagreement between patients, caregivers and healthcare providers, there is a need to further characterize the benefits and drawbacks of each perspective.
This study will add to the available Canadian data demonstrating a need for additional guidelines and resources for the provision of futile care, and will contribute to the current lack of literature exploring this topic.
Our findings highlight the need for more careful resource allocation in the context of critical care medicine, which will contribute to ongoing debate regarding the delivery of futile care.
Introduction
Critical care involves the ability to invasively monitor and treat patients suffering from life-threatening illness. As it is a finite resource that costs on average 3 times more per day than care provision on a general ward, 1 a rational use of critical care is required. The use of critical care in order to prolong the life of patients who have little probability to benefit or recover is questionable. These situations have been described as non-beneficial, inappropriate or futile care, and merit evaluation as to the appropriateness of applying critical care resources.2-4 The determination of futility in these cases is often based on qualitative assessment, rather than a purely physiologic one, 5 and encompasses judgment on achievable quality of life, potential harms, and the opportunity-cost of delivering the care. There are negative consequences to the delivery of critical care, such as physical and psychological pain inflicted on the patient, as well as psychological distress experienced by family members and staff.6-8 The cases are often difficult and controversial with the potential for physicians and patients or their substitute decision makers (SDMs) to disagree despite all efforts at communication and second opinions.
In Ontario an avenue to address cases of disagreements such as these is via application to the Consent and Capacity Board of Ontario (CCB). The CCB is an independent provincial tribunal mandated to adjudicate various issues through the interpretation of the Health Care Consent Act, Mental Health Act, Personal Health Information Protection Act, Substitute Decisions Act, or Mandatory Blood Testing Act. Regarding the Health Care Consent Act, the tribunal will hear cases surrounding capacity to consent and review of an SDM’s compliance with the rules for substitute decision making. 9 Hearings are scheduled within 7 days of the receipt of the application in order to expedite decision-making. This avenue is rarely used as it can harm the physician-patient relationship, is time consuming and stressful for all parties involved. As a result, this option for resolving end-of-life care decisions is often reserved for extreme cases of disagreement between the treating team and the SDM.
Few studies that have looked at the frequency or impact of futile critical care.10-12 In the Canadian context, several qualitative surveys have demonstrated that poor healthcare provider-patient communication contributes greatly toward decisions for futile care delivery.2,13,14 Additionally, these studies have consistently concluded that new techniques for reducing nonbeneficial treatment are needed, the most promising of which is the improved education of providers and caregivers on the subject.2,13,14 In this study we describe the hospital length of stay (LOS), intensive care unit (ICU) LOS, cost, and long-term outcomes of 12 cases that have been, or were considered for, adjudication by the CCB.
Methods
The study was carried out at a large academic-affiliated tertiary care center in Ontario with 2 ICUs. A center chart review was undertaken to identify all patients admitted to the ICU from 2010 to 2017, where attending physicians felt that critical care was futile. The inclusion criteria for this study was consensus reached at a monthly divisional meeting to submit the case to the CCB due to the care being provided either not meeting the standard of care, being against the patient’s wishes, or not in the patient’s best interests. The definition of best interest is outlined in section 21 of the Healthcare Consent Act. 15 Cases were included if an application was submitted to the CCB, even if it was subsequently rescinded. Cases were rescinded in the event that the patient died prior to the hearing, were transferred to another hospital, or a compromise was reached with the patient’s SDM. Costs for each of these admissions were subsequently determined using the case-costing system of The Ottawa Hospital Data Warehouse, a standardized methodology developed by the Ontario Case Costing Initiative. 16 Costs were broken down into “direct” and “indirect” components. Direct costs include expenses to the hospital through fee codes linked to the patient chart, including salaries, equipment, and materials. Indirect costs include overhead operational fees associated with the service being provided to the patient. Costs were then indexed using consumer price indices in a validated manner.17-19 Costs include the total estimated costs from hospital presentation until discharge or death. Total costs were tabulated for each patient’s stay in hospital and average costs were calculated. Ethics board approval was obtained from the Ottawa Health Science Network Research Ethics Board.
Results
Twelve consecutive patients meeting the inclusion criteria were identified for a case series on the economic analysis of their hospital admission. The median age at the time of admission was 83.5 days and 8 of 12 patients were male (Table 1). All 12 patients had a LOS greater than 120 days, with the longest being 704 days. Eight patients in this cohort had advanced dementia at the time of their hospitalization, and 3 patients presented with a catastrophic neurologic injury. All patients underwent tracheostomy, 10 out of 12 had percutaneous endoscopic gastrostomies placed, and 1 was nasogastric tube dependant (Table 2). All patients developed pressure ulcers during their hospitalization despite standardized pressure ulcer preventive strategies. Prior to admission only 1 patient was on dialysis compared to 5 among patients who were transferred to other facilities, or at the time of death. No patients had tracheostomies or gastrostomies on admission, but all had tracheostomies upon being transferred to other facilities or at the time of death, and all but 1 were dependant on artificial feeding. One patient developed advanced dementia after admission to hospital, while another had a series of ischemic strokes causing irreversible and severe damage to their cognition. No patient in the study was discharged to an independent living situation. Seven patients died in hospital, while 5 were transferred, 3 to other acute care hospitals and 2 to specialized long term care facilities (Table 3). Four out of 5 transferred patients remained mechanically ventilated at the time of transfer. All patients ultimately died with none ever returning to independent living situations. Four out of 5 patients died within 3 months of discharge from our hospital. The remaining patient died, however the timeline is uncertain as they were transferred to a hospital in another country prior to their death. The mean direct costs were $500 086.59 (standard deviation [SD]: $303 245.48; total: $6 001 039.10) and indirect costs were $158 043.23 (SD: $98 650.62; total: $1 896 518.75), equating to a total cost of $7 897 557.85 for the 12 selected patients. The average cost per patient was $658 129.82 (SD: $401 489) which equates to $2702.42 per day (SD: $849.68) for the entirety of their stay.
Patient Characteristics on Admission to Hospital.

Patient Characteristics During ICU Admission.

Length of Stay and Costs Associated with Each Patient.
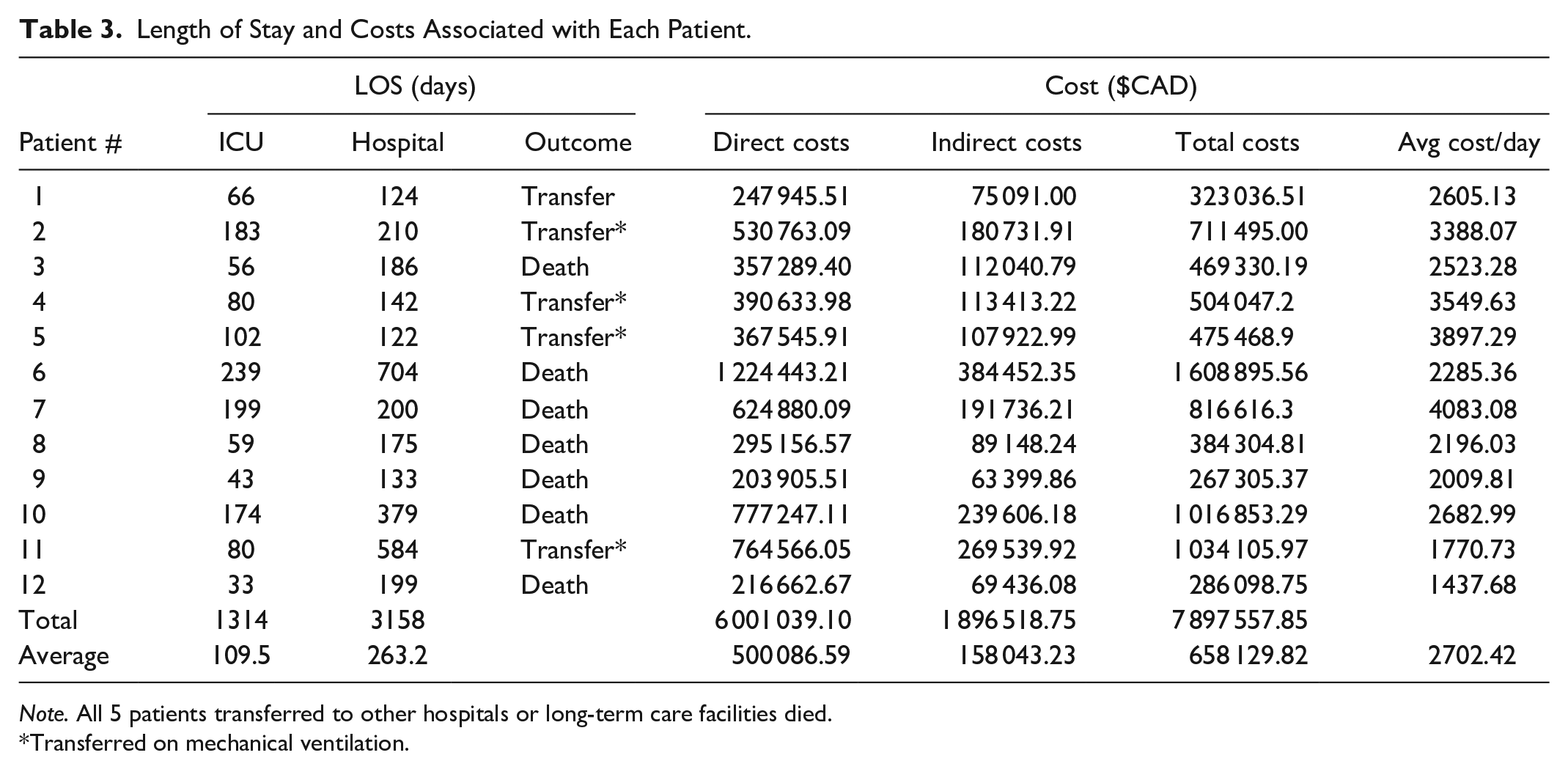
Note. All 5 patients transferred to other hospitals or long-term care facilities died.
Transferred on mechanical ventilation.
Interpretation
There is a significant economic cost to providing resource-intensive critical care to patients in which these treatments are considered futile. A high threshold for inclusion into this case series was selected in order to reduce any risk of debate about care futility. As a result this study does not reflect the total number of cases that could be considered as futile during the 7-year study period, but rather the most egregious cases that were selected to be brought before the CCB.
The 12 patients identified in this study were all considered to be patients who would never benefit from ICU level care. Despite this, critical care was provided to them for up to 2 years. Even with extensive and prolonged care all patients died without regaining independence. This cost nearly $8 000 000 for 12 patients alone, with an average cost of $658 129.82 per patient. Measured on a per day basis the patients in this study accrued costs of an average of $2702.42 per day over their average 263.2 days.
This study supports previous American 10 and Australian 11 study findings of significant costs associated with the delivery of futile care across these differing health care models. Together these findings demonstrate that use of healthcare funding to provide futile care is widespread and represents a global economic issue. There are both financial and non-financial opportunity-costs associated with providing futile care. Millions of healthcare dollars in our hospital alone were spent delivering futile treatments when this funding could have been re-allocated elsewhere.
It is important to note that all patients in this study suffered irreparable and severe loss of function and independence. On admission only 1 patient required dialysis and none were artificially fed or had tracheostomies. This is in stark contrast to the fact that all patients were dependant on tracheostomies and all but 1 required permanent artificial feeding at the time of transfer or their death in hospital. The extreme loss of function in every patient led to pressure ulcers, suffering, and ultimately death. Patient suffering was clearly documented by nursing staff and physicians in each chart.
On top of the economic burden and significant loss of patient quality of life is the moral injury sustained by ICU healthcare providers including physicians and nurses. Moral injury, a term originating in the military context, refers to experiences of serious inner conflict arising from what one takes to be grievous moral transgressions that can overwhelm one’s sense of goodness and humanity. 20 In the medical context, it is increasingly used to describe situations where providers feel that they are causing a patient pain and suffering without any hope of benefit to the patient, thereby causing inner conflict. Accordingly, the literature suggests that the potential suffering involved in futile care delivery is often not fully understood at the time of decision-making. 21 Moreover, one 2015 Canadian survey found that 83% of futile care patients felt that their life-prolonging treatments were inconsistent with their goals of care. 2 These are likely under-recognized, but critically important elements of providing futile care6,22 and warrant further investigation in order to fully characterize the impact of providing futile care within the health system. These findings would also help contribute toward developing more comprehensive guidelines for the provision of futile care, and ensuring genuine and mutual understanding among providers, patients, and caregivers.
This study is limited by the pooling of ICU and ward costs. While the data does not illustrate the ICU-specific costs associated with futile care, given that the patients’ lengths of stay were a result of futile care provided within the ICU, the total stay cost is an important figure for the economic analysis of these cases. This study also does not include the costs incurred by transferring the 5 surviving patients to other hospitals or long-term care facilities. The healthcare costs associated with these patients would likely be significantly higher, despite providing no benefit to the patient. These uncounted additional costs further support the argument for proper utilization of medical resources. Another limitation is the use of estimated direct and indirect costs rather than exact costs. It was not feasible to obtain exact costs for the study, however we employed a standardized methodology developed by the Ontario Case Costing Initiative in order to quantify cost. While fixed costs such as staffing are often unmodifiable, nursing costs in this center are not entirely fixed given that staffing levels fluctuate to match patient demand. This methodology also does not allow us to differentiate between costs accrued during ICU vs subsequent floor stays. However, despite this we saw a 3-fold higher per day costs in our study compared to a standard floor visit, which demonstrates that critical care costs are the main drivers of the total cost. 23 The majority of floor costs were also directly attributable to inappropriate critical care received as many patients spent significant time on the floor after transfer out of the ICU. If we were to assume an even average daily cost between floor and ICU days (which would significantly undervalue ICU costs) then those days would still amount to $295 914.99 per person, or $3 550 979.88. Future research examining the patient factors that contribute most to higher costs in futile care (ie, dementia, neurologic injury, dependence on renal replacement) would be instrumental in improving our understanding of cost drivers in futile care provision.
The determination of medical futility remains a controversial topic and requires further debate. Despite this lack of clarity, in a climate of budget cuts and limited funding, we can no longer pretend that there is no price tag on healthcare. We as clinicians must carefully consider the allocation of these valuable and finite resources in order to utilize them in a way that most benefits patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.