
Abstract
This article presents an exploratory model to classify public attitudes towards health systems financing and organization. It comprises 5 factors (pay-as-you-use, solidarity, willingness to contribute, mixed financing, and public provision) measured by 17 indicators, selected through Exploratory Structural Equation Modeling (ESEM) applied to a sample of Chilean adults. Based on this model, cluster analysis proposed 2 groups: “Taxes-public” and “Insurance-choice,” representing 47% and 53% of interviewees, respectively. The results show differences between groups concerning the evaluation of both health care providers and insurers. The second cluster tends to evaluate them more harshly, showing less willingness to contribute further, less solidarity, more agreement with the current financing arrangement in terms of the mixture and its insurance (as opposed to purchasing of service based on health problems), and more support for choice of provider. These results highlight the need to consider people’s attitudes in the public discussion of health systems financing.
Introduction
The Human Rights Universal Declaration states the right to medical assistance. 1 Universal health coverage is justified mainly through values of justice and equity. 2 The possibility of universal access depends crucially on health financing and the organization of its provision. There are different ways of financing and organizing health services, with varying levels of tax funding and decentralization of public provision, role attached to private provision, level of user fees, and degree of autonomy of the medical profession.1-3 Only a few facts are well established, and they leave the menu of alternatives wide open. For instance, an increase in public health financing has been shown to improve health outcomes,1,4,5 especially among the poor and vulnerable, 6 while the introduction of co-payment systems is associated with negative effects on health coverage, 7 poverty,8,9 and concerns about the future regarding access and falling into poverty due to sickness.10-12 In lower-income countries, international donations are vital to sustaining sanitary coverage and access for the poor. 13
Choices in this area are eminently political, in the sense that there is no optimal “technical” solution but trade-offs that have to be weighted by the political system. Given the political nature of health financing and organization choices, it is important to consider public opinion on the matter and close the gap between these opinions and the prevailing situation. The present study contributes to the topic of health financing through reporting and analyzing citizen’s preferences to understand people’s attitudes toward this topic.
International studies shed light on citizen’s attitudes toward costs and health services financing. There is a big concern about healthcare costs (insurance, cost of services, hospitals, among others) by low-income users. In New York, 37% preferred governmental financing, 29% mixed financing, and 34% private financing. Support for National Health Insurance is inversely associated with income, education, and health condition. People whose healthcare costs are covered with public money favored the role of government. These results show a divide between those “who have” and those “who have not.” Despite empathy for those without resources among supporters of both alternatives (private vs governmental), many people on both sides opposed universal national health insurance. 10
A comparative international study conducted in Australia, Canada, New Zealand, United Kingdom, and the United States reported concerns about access and costs for uninsured people. The results show that exposure to high “out-of-pocket” expenses, difficulties in accessing medical attention, and fear about the quality of attention increases public dissatisfaction with health services. 11 Additionally, an overall positive perception about public healthcare’s moral commitment to the common good over individual self-interest seems to be a driver for public support toward public health services in the European Union.
The support to public healthcare was positively related to social democratic aspects of the Welfare State, while support decreases with higher degrees of liberalism or conservatism among UE citizens. Universal and publicly-funded welfare state programs enjoy more public support and lead to consensus about the public responsibility for such provisions. 14
Public disposition to decrease the consumption of private services to obtain better medical services was studied in Denmark, finding that primary and secondary prevention is rated slightly higher than the availability of possible treatments. These results are examples that the public is willing to give up current consumption to fund investments for future benefits. Danish public leans more strongly toward out-of-pocket payments than tax increases (in a context of already high tax rates). 15
These studies have delivered thoughtful results, but further research is needed. People must have a powerful voice and role in the decisions concerning systems that affect their health, and they need tools that can help them participate more actively. 16 In Sweden, a gap has been found between public expectations and medical attention resources, making it even more important to have clarity on who must be accountable for resource allocation in public healthcare. 17 Research about citizen’s opinions in developing countries has focused primarily on willingness to pay for health insurance, for example, Myanmar, 18 Ethiopia, 18 and Uganda. 18 More related to our work is the study of the associations between satisfaction with the health care system and its determinants in Armenia 19 ; public attitudes toward health insurance and its reform in Croatia 20 ; the analysis of public opinion on universal health care coverage on health care affordability and financing issues in South Africa 21 ; and the study of attributes of health insurance benefit packages in Iran. 21
This article aims to gain a deeper understanding of attitudes toward health financing through the application and analysis of a scale developed especially for this goal. It provides evidence on underlying dimensions and profiles in public attitudes toward health financing in Chile through statistical modeling. This research also makes a significant contribution by identifying public attitudes relevant to inform public policy on health system reform. Policymaking in the health sector is primarily the field of experts in Latin American and Caribbean countries, meaning limited or inexistent public consultation in its design. 22 As already argued, the fact that there is no optimal technical solution in these matters requires that political choices reflect citizens’ preferences if the democratic process articulates them adequately.
Chile represents an interesting case that achieved a robust and efficient public health system following the NHS model well before the Coup d’État in 1973. The Dictatorship reformed the health system in the 1980s, inspired by a vision of society focused on individual initiative and preferences, 23 promoting choice between private insurers and providers by creating a mixed financing model. The system operates with 2 sub-systems, 1 public, the Fondo Nacional de Salud (FONASA), and 1 private, with a predominance of the Instituciones de Salud Previsional (ISAPRE), for-profit insurers serving less than 20% of the population, mainly from higher-income groups. The legislation stated that active workers should devote a minimum of 7% of their gross salaries to pay for health insurance. Individual workers had the right to choose between allocating this amount either to FONASA or ISAPRES. 24 The latter offers different plans according to the risk of its beneficiaries, which might require a higher payment to the fixed percentage mentioned above. High-income young males were the privileged target of ISAPRES.
On the other hand, FONASA was held responsible for all the population not covered by ISAPRES, including non-contributing informal sector workers or the homeless. Research shows that the main reason for the perception of non-protection for FONASA users is the perceived quality of the system and, among ISAPRE users, the cost of services and coverage. 25 In 2016, Chile’s health system users reported that they spent $500,000 on average (a little over US$700) during the last 12 months for treatments outside of their medical insurance plan (FONASA or ISAPRE), an amount that matches the national average monthly income and is equivalent to 1.43 times the median income of workers. 25 The last wave of the Latin America Public Opinion Project (LAPOP) survey included, in the case of Chile, a question about the quality of medical and health services, rated primarily as unsatisfactory. 26 Chile’s life expectancy is, nonetheless, 80.6 years in 2019, the highest in Latin America.
Methods
We developed an exploratory questionnaire to identify the main attitudinal dimensions associated with health financing. The questionnaire was applied to a random sample of 1201 persons over 18 years of age living in Gran Santiago, Gran Valparaíso, and Gran Concepcion in Chile. These zones correspond to the urban areas of the homonymous provinces, which concentrate roughly 70% of the country’s urban population. 47.6% of those surveyed were men and 52.4% women, the mean age being 42.82 years (standard deviation: 17.87). The study followed a cross-sectional design. The sampling technique was probabilistic with 3 stages (housing block, dwelling, and person), with an associated error of 2.85% (IC: 95%). The selection for the 2 first stages was random, and the third (person) made use of a Kish table. The questionnaire comprises 22 statements with a rating from Strongly disagree (1) to Strongly agree (7). It was developed through experts’ consultation. The included and excluded statements, as well as descriptive statistics, are presented in Table 1. Imputation of missing data was performed using the median of each item.
Descriptive Statistics of 22-Item Health Financing Attitudes’ Original Scale.

Item deleted from original scale.
For factor extraction, a parallel analysis was used. This factor selection procedure is based on a scree plot of the eigenvalues obtained from the sample data and estimated eigenvalues from a set of random numbers. The observed sample and random data eigenvalues are plotted; the point where the 2 lines cross indicates the appropriate number of factors. 27 Parallel analysis is usually more accurate than other approaches for factor selection. 28 Also, we used Exploratory Structural Equation Modeling (ESEM) as a factor selection procedure. The main advantage of ESEM is the combination of Exploratory Factor Analysis (EFA) and Structural Equation Modeling (SEM): estimation of usual parameters, loading rotation, and transformation of structural coefficients. It also provides errors and overall tests of model fit. 29
For factor rotation, we used Geomin to maximize the magnitude of primary loadings and minimize the magnitude of cross-loadings. Geomin is recommended to produce factor loadings and factor correlations without having to specify the factor loading pattern and structure.29,30 This rotation was preferred over orthogonal rotation because the former increases the values of primary loadings, and the latter may produce misleading solutions when the factors are correlated. 27
For group identification, we performed cluster analysis using the k-means method. Cluster analysis is used here within the context of exploratory analysis.31,32 The objective of cluster analysis aims to identify groups underlying a more extensive set of data when the number of groups is initially unknown. 33 Regarding cluster algorithms to enter cases into groups, k-means is an iterative partitioning method, which assigns cases to the cluster with the nearest centroid (collection of variable means for a group of variables). 31 R+ was the software used to carry out the analyses.
Results
Factor Analysis
Parallel analysis results suggest a 5-factor structure (we also estimated 6 and 7 factors solutions. They were difficult to interpret and showed a worse performance in some goodness of fit indices. Therefore, a 5-factor solution was retained, following the criteria that substantive and statistical considerations should guide the appropriate number of factors) could be proper for the data (Figure 1).
27
Model parameters were estimated using the Maximum Likelihood Estimation (ML) method. We examined model fit in terms of multiple fit indices: root mean square error of approximation (RMSEA), Tucker–Lewis index (TLI), standardized root mean square residual (SRMR),
34
and chi-square ratio (

Parallel analysis.
A first estimated model comprising 5 factors and 22 indicators showed a low performance of fit indices. Therefore, a second model was estimated, excluding 5 items (P1, P2, P6, P12, and P15). Its primary loadings were strong in more than 1 factor, or they have a magnitude under 0.3 (considered as non-important loadings).
27
This second model, with 17 items exhibits a better goodness of fit:
Standardized Factor Loadings of 17-Item Health Financing Attitudes’ Scale.
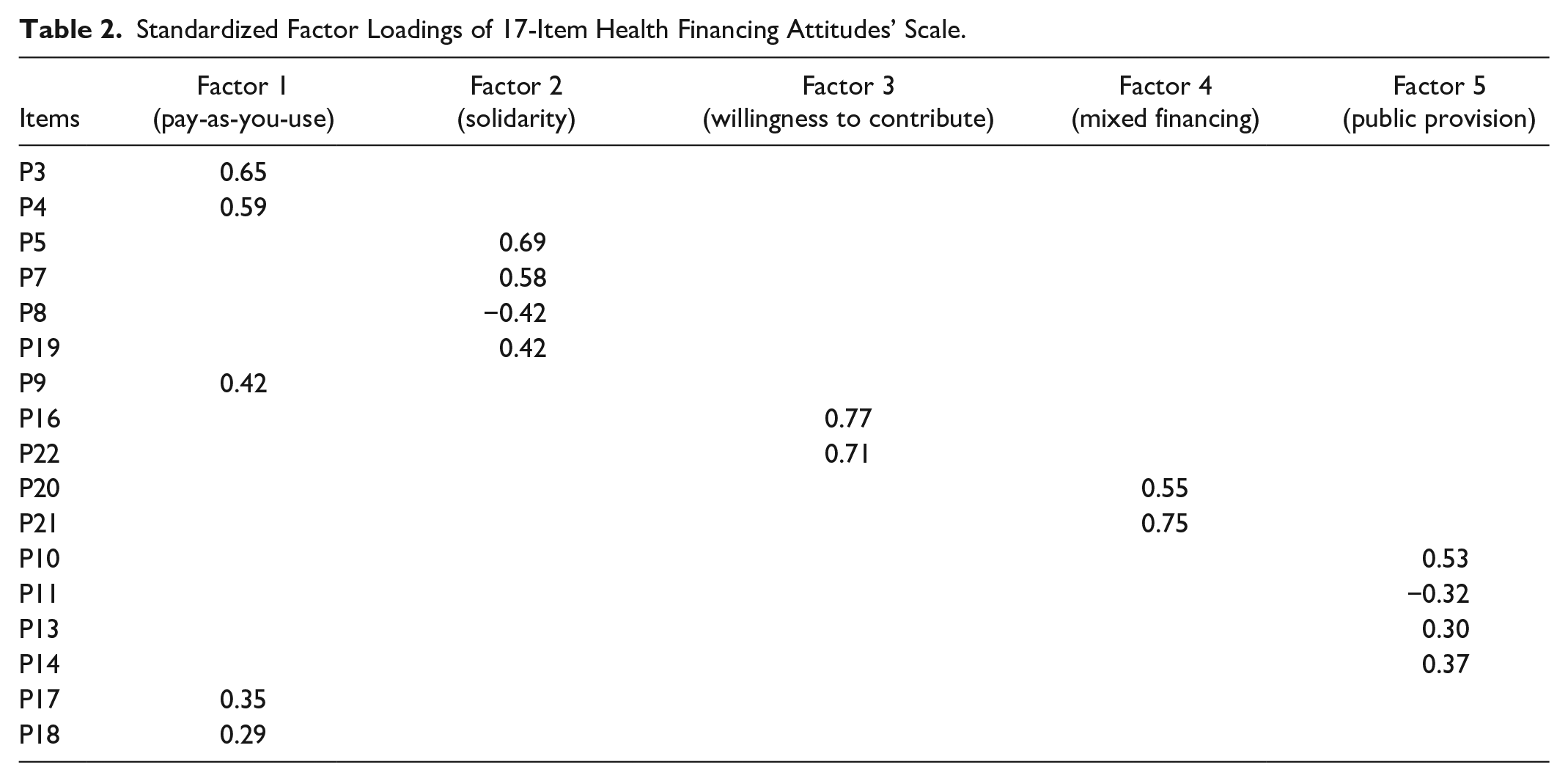
The factors arising from the 17 variables are as follows:
The first factor is formed primarily by positive loadings in 5 out of the 17 items (P3, P4, P9, P17, P18). High scores on these questions indicate support for higher payments according to risk (P3) and income (P4). It also comprises support for the following statements: Health services should be paid by mandatory deductions of 7% (actual level) exclusively (P18). The government should reimburse individuals that contribute more than what they use in health services (P9). Direct payments should replace mandatory deductions according to use (P17). This factor can be named “Pay-as-you-use.”
The second factor is formed mainly by positive loadings on P5, P7, P19 and negative loading on variable P8. High values in this factor show support for a State responsibility with users of the health system, especially the most vulnerable, and health care financing exclusively through taxes. Therefore, this factor can be denominated “Solidarity.”
The third factor is related to high values of only 2 variables: P16, P22. Individuals with high values in this factor are those who are willing to pay more taxes (instead of salary deductions) or increase their salary deductions to finance a better health care system (for all). We defined this factor as “Willingness to contribute.”
The fourth factor is related primarily to high values of variables P20 and P21. Taking into account that individuals that have high values in these variables are those who are in favor of mixed financing between the public and private sector, this factor is called “Mixed financing.”
Finally, the fifth factor is related to high values in P10, P11, P13, and P14. Individuals with high values in this factor sympathize with the public sector as the sole health service provider and do not support freedom of choice. Because of this, factor 5 is named “Public provision.”
Those with positive scores in the dimension “pay-as-you-use” are keen to use mandatory contributions exclusively to finance expenditure on an individual basis and reimbursing what is not spent individually, thereby eliminating any insurance mechanism associated with such contributions. 15
People with a positive perception of the dimension “solidarity” value a government allocation of more resources to finance healthcare for the most vulnerable and subsidizing those who cannot afford to pay for their healthcare. This factor shows a commitment to the common good over individual self-interest as a motivation for supporting public health financing. 14
The idea of complete financing by the government through taxes is more prevalent among low-income people. 10 Fifty-eight percent of respondents from socioeconomic level “D” (lowest income) show a high degree of agreement with this statement compared to 41% from socioeconomic level “ABC1” (higher income), which is, nonetheless, still high.
The positive rating of the dimension “willingness to contribute” considers a higher intention to pay, which could be related to lower private consumption to obtain better healthcare services, whether as taxes or as salary deductions. 15 In Chile, only 17% of participants from socioeconomic level “D” manifest a high level of agreement with this higher deduction in comparison to 28% of the group “ABC1.”
The positive evaluation of the dimension “mixed financing” assumes that there should be more solidarity funding between FONASA and ISAPRE or between individual worker’s mandatory deductions, government payments, and employer’s support. 14 A fundamental issue about the actual structure of health financing in Chile is that many higher income groups have abandoned the public system, reducing its funding, and transferring it to private insurers.
Individuals from higher income groups remaining in FONASA contribute with their mandatory 7% to health financing of lower-income groups. On the opposite side, the ISAPRE system treats the contribution of their affiliates exclusively on individual terms and attempts to maximize profits over each individual. 24
Finally, the positive evaluation of the dimension “public provision” refers to supporting the government as the only healthcare supplier and a better perception of its service quality over private institutions. 10 Those who report high values in this factor also favor imposing restrictions over the choice of health institutions or doctors and attending health services on a territorial basis.
Typology Analysis
Cluster analysis allowed classifying respondents and finding the main characteristics of each group. The silhouette method indicates that the best option is to classify respondents into 2 clusters (Figure 2). The first group has 559 respondents (47% of the total), and the second group has 642 respondents (53%). Table 3 shows the average score of the 5 factors for each cluster.

Cluster analysis.
Classification Matrix.

Statistically significant (P < .01).
Through a mean differences t-test, we can see that, except for “solidarity,” each 1 of the other 4 factors has a statistically different mean (at P < .01) in both clusters. The “solidarity” factor would be significant at 93%.
Respondents classified in the first cluster prefer a more direct relationship between individual contributions and the use of health services (“pay-as-you-use”). They report a higher willingness to contribute through taxes instead of social security contributions. They are also willing to pay more, not inclined toward mixed financing, and support the public provision and restrictions on choice.
The second cluster comprises people with lower support of “pay-as-you-use,” and a lower willingness to contribute. They are supporters of mixed financing and not in favor of restricting choice. They are more aligned with the prevailing situation in their preference mix but are less satisfied with its quality. Accordingly, the first cluster can be named “Taxes-public” and the second “Insurance-choice.”
Respondents classified in cluster 1, “Taxes-public,” belong mainly (34%) to socioeconomic group ABC1 (highest level), while Cluster 2, “Insurance-choice,” has a more significant proportion of groups (28%) C2 and D (lowest level), respectively. However, the relationship of attitudes with socioeconomic status is far from perfect, and there is an important percentage of each socioeconomic group in both clusters. This limited discrimination among socioeconomic groups could be related to the high access to ambulatory medicine through low-priced private services providers that lower-income households get, effectively reducing their waiting lists for medical consultations. Most of the limitations in the access to health procedures for lower-income groups are medium to high complexity procedures involving a high out-of-pocket supplementary payment.
On the other hand, while most respondents are insured by FONASA (as expected from a national sample), a smaller proportion of those affiliated to FONASA are classified in the Taxes-public cluster. The more extensive relative representation of respondents affiliated to private institutions in the Taxes-public group seems consistent with their preferences (Table 4). A test of independence confirms that the healthcare system’s differences are statistically significant (at P < .05).
Cluster by Healthcare System.

The differences among the clusters are not statistically significant by sex and age, even though there are slightly more 25 to 34 years old and less presence of women in the “Taxes-public” group (at P = .65 and P = .18, respectively).
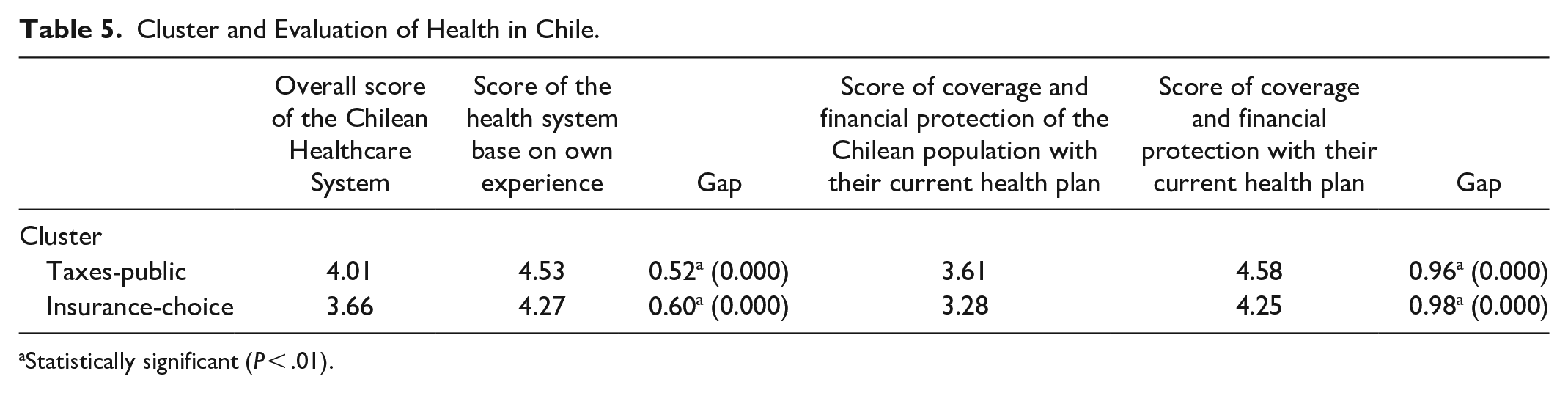
The “Taxes-public” cluster evaluates the health system better than the “Insurance-choice” cluster (Table 5): 4.05 on a scale from 1(lowest) to 7 (highest), against 3.64 respectively. Although both averages are low, the difference is statistically significant.
Cluster and Evaluation of Health in Chile.
Statistically significant (P < .01).
These ratings are higher when evaluating the health system based on their own direct or vicarious experience, although the difference between clusters holds in place: “Taxes-public” gives a higher rating (4.57) than “Insurance-choice” (4.24) to their system of affiliation.
Similarly, “Insurance-choice” evaluates coverage and financial protection of health plans with the lowest score (3.28, against Taxes-public 3.62). These ratings vary according to the individual’s health plan, confirming the evaluation gap described before: “Taxes-public” evaluates this item with 4.58, while “Insurance-choice” with a 4.26.
Discussion
As always, with exploratory work, we should interpret these results with caution. Factor analysis always involves some relatively subjective choices. For instance, the first draft of this work contained a question “All healthcare suppliers (primary care – hospitals) should only be private.” Its loading was almost equal in factors 1 and 2, around 0,30. However, the question was more related to service provision than financing (both of which have private components in Chile) and, therefore, conceptually related to factor 5. However, factor 5 includes the question “The Government should be the only healthcare provider through municipal primary health care and public hospitals.” One of the 2 questions was, in fact, redundant. In this final version, following the referee’s insights, we opted to drop the question. With this new specification, the model maintained its goodness of fit and became more parsimonious. A critique over latent model analyses using EFA or ESEM is their indeterminate nature. It means that when there is more than 1 factor, which is the case of this study, we can obtain an infinite number of factor loading combinations of equally good-fitting solutions.27,36 On the other hand, cluster analysis has resulted in 2 well-defined profiles on attitudes toward health financing and organization in Chile.
This study’s main contribution is significant on 3 levels: (1) measurement of citizens’ attitudes toward health financing, an underdeveloped area in Latin America; (2) an empirical classification of citizens based on statistical modeling. While both aspects are subject to improvement, this article advances this topic in a country where there is a private healthcare provision and a population segment that can choose. Finally, (3) it identifies the main attitudinal profiles (clusters) in Chile, comprising a distinct combination of attitudes relevant to health financing. These profiles may contribute to tailoring and targeting policy-making processes, from citizens’ view, as relevant stakeholders of the health sector. On the other hand, understanding public attitudes toward health financing is crucial to building democratically acceptable and legitimate health services.
It is important to note some limitations of this study. Firstly, the cross-sectional design of the study limits its scope. It would be interesting to explore change in attitudes on health financing over time either individually (for instance, after a significant health issue or a continuous contact with health services) 37 or collectively (assessing knowledge and the acceptability of funding reforms). 38
Second, we believe there is ample space for improving the measurement model specification (eg, number of factors, relations between factors and indicators, and relations among indicator errors), which could help facilitate the creation of short versions of the questionnaire.
Third, using scenario analysis or experimental design to assess peoples’ health financing preferences can strengthen the resulting model. We have not found extensive research on citizens’ preferences on health financing in developing countries, which could inform policy decisions.
Conclusions
Health financing is a widely discussed topic in public health policy at both national and international levels. There are profound controversies regarding the ways health services must be financed and organized. While there is no optimal technical solution, citizens’ preferences and opinions on the subject haven’t been widely studied either.
This study revealed 5 key dimensions that structure people’s attitudes toward health financing and organization in Chile using a survey conducted in the country’s 3 most populated metropolitan areas. The 5 latent factors were labeled “Pay-as-you-use,” “Solidarity,” “Willingness to contribute,” “Mixed financing,” and “Public provision.”
Chileans hold preferences, beliefs, and attitudes about how the health system should be structured and financed. One group (Insurance-choice) expresses more disagreement with the prevailing situation than the other. Moreover, both groups evaluate poorly the health system. Still, those in the insurance cluster have the worst evaluation, which may reflect their dislike of the prevailing organization and a certain skepticism regarding the possibility of achieving a positive change. It is necessary to move forward with explanatory approaches that account for the determinants of these perceptions and attitudes and whether this low rating implies apathy and carelessness or a more active stance toward the issue. Other evidence that shows low levels of agency in the Chilean population tends to favor the first possibility.39,40
However, the massive street demonstrations that started in October 2019 alluded to fundamental human rights such as health, pensions, and education provided unevenly based on market mechanisms 41 and might signal a turning point. These protests were not channeled through the political system. They expressed discontent with the Executive branch and the Congress and political parties that achieved levels of trust of 3% and 2%. Disaffection with the political system has been a gradual process since the return of democracy. 42 Caring more about people’s attitudes and beliefs and ensuring those preferences are articulated and aggregated through the political system is an essential component of any strategy to address this disenchantment.
Although the gap between citizen’s preferences and attitudes regarding health financing and actual policies is illuminating, an opinion survey is not enough basis for decision-making. More democratic policies would require a process of rational deliberation to overcome (adaptive) preferences for achieving a better understanding of the issue and the trade-offs involved. 42
Footnotes
Acknowledgements
The authors would like to thank the support of the administrative staff at the Center for Public Systems, University of Chile, the Institute of Public Health, and the PhD Program in Education Education and Society at Universidad Andres Bello. JC Oyanedel also would like to thank Uma and Cuma for their support during the preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by SCIA ANID CIE160009 and FONDECYT 1181533.