
Abstract
To evaluate the preference of young adult patients and their willingness to pay for the different approaches accessible to accelerate orthodontic tooth movement. A cross-sectional survey was conducted in Jeddah, Saudi Arabia from September to December 2019. Young adult orthodontic patients from 18 to 45 years old were interviewed via online survey regarding their perception to the extent of treatment, acceptability of non-invasive (customized appliances and medications) and invasive (surgery) approaches accessible to accelerate orthodontic treatment and increase in fees they were willing to pay. Statistical analyses were performed, and gender difference was calculated at P < .05. There are 100 respondents: 70% aged between 18 to 25, 50% male, and 56% with annual income <10 000 SR. About 72% of the respondents decided that treatment takes longer period and 51% wished it would last for less than 6 months. Customized appliances were reported to be the most convenient to use (58%) and to pay (44%), followed by medications (48%). On the other hand, surgery was reported to be the most inconvenient to use (58%) and to pay for (55%). About 70% of the respondents were unwilling to pay more than 10% to 20% for all procedures assessed; considerable variation was not observed in responses between gender at 95% confidence level. Majority of the respondents believed that orthodontic treatment is taking lengthy duration. Less invasive, nonsurgical techniques and procedures were more preferred. Likewise, financial factors play vital role in the selection of their preferred approach. Most of them agrees to provide up to 20% increment of the fee for additional procedures.
Accelerated orthodontic tooth movement using different mechanical, surgical, and pharmacological approaches is gaining popularity among orthodontics. However, patients’ acceptance to such approaches is not yet deeply studied.
The current study focused on assessing the preference of young adult patients and their willingness to pay for the different accelerated tooth movement modalities. The young adult age group was chosen as the sample for this study as they represent the highest age group that can benefit from accelerated orthodontic tooth movement.
The current study showed that both invasiveness of the procedural approaches as well as the financial concerns are the most predictive factors in patients’ acceptance to accelerated orthodontic tooth movement. Such finding will have a great implication on the direction of the orthodontic practice. The orthodontists as well as the manufacturing companies need to work hard to solve the challenges between reducing orthodontic treatment time and meeting patients’ abilities and concerns.
Introduction
Modern technological advancement created a pathway in the development of the field of orthodontics, which then led to the increment in orthodontic treatments in the last decade. Yet, 2 major factors played a vital role in orthodontic treatment: (1) orthodontic treatment duration, and (2) fees associated to orthodontic treatment. Particularly, adult patients consider financial constraints as one of the barriers in seeking orthodontic treatment. The use of modern technology in orthodontic treatment also provided a means in the rise of treatment fees. Likewise, adult patients deemed shorter treatment duration as necessary since majority of them is part of the work force. In addition, prolonged treatment duration increases the risk of decalcification, gingival inflammation, root resorption, and dental caries.1-4
Tooth movement is classified into 3 phases: (1) rapid movement after application of force, (2) lag period, and (3) occurrence of gradual increment of movement. 5 Various strategies have been developed to speed the movement of teeth during orthodontic treatment as well as to shorten treatment duration, such as biological, physical, biomechanical, and surgical approaches.4-6 These strategies were mentioned to hasten orthodontic tooth movement and diminish the extent of treatment, which can minimize its potential treatment risks.2,4-9 The use of prostaglandin E and cytokines were prominent biological methods for tooth movement. 5 In addition, Collins and Sinclair studied the impact of cholecalciferol (vitamin D) on orthodontic tooth movement. The authors reported an increment in the number of activated mononuclear osteoclasts, which resulted to higher alveolar bone resorption. 10 However, majority of these studies were conducted on animals.5,6
Device-assisted therapy, which utilizes direct electric current and low-level laser, is another technique in hastening tooth movement.5,6,8 Kau used orthodontic treatment coupled with resonance vibration at a rate of 20 to 30 Hz per 20 minutes in a day to know whether root resorption was produced. The use of resonance vibration prevented root resorption and allowed healing of cementum.11-13 Another study conducted by Woodhouse and others compared the pain felt by the patient when using conventional fixed orthodontic appliances and additional vibrational devices. No significant variation was observed in pain between these approaches as well as significant reduction in treatment duration.7,8,14,15 Despite those advantages, treatment cost increment is a key issue considered when using this technique.5,6,8,14 Many studies on accelerated orthodontic tooth movement focused on surgical techniques, such as corticotomy and piezocision.5,16-20 Many clinical applications are focused on these 2, owing to its effectiveness in reducing orthodontic treatment duration and hastening tooth movement.1,5,6,16-20 However, issues on the use of this treatment arise due to its invasive nature as it needs complete mucoperiosteal flaps and extensive exclusion of alveolar cortical bone, with side effects such as post-surgical discomfort, inflammation, and hematomas.1,5-7,16-19 On the other hand, piezocision is deemed effective in reducing treatment duration without any unwanted side effects.7,20
Most adults as well as orthodontists reported higher acceptability for less invasive orthodontic treatment techniques. 4 This can be attributed to sociodemographic factors such as gender, age, level of income, treatment cost, as well as educational level.2-4,21,22 Likewise, ethnic background also played a significant role in expectation of patients on orthodontic treatment. 23 Uribe and others reported that shorter treatment duration is preferred by patients as they were willing to pay for about 20% above treatment cost for painless treatment with shorter duration. 4
This study aimed to evaluate the preference of young adult patients and their willingness to pay for the differ-ent approaches accessible to accelerate orthodontic tooth movement.
Material and Methods
This study, which utilized a cross-sectional approach, was performed in Jeddah, Saudi Arabia on a period of September to December 2019. Ethical approval was conducted by the Ethical Committee of King Abdulaziz University, Faculty of Dentistry. The questionnaire was adapted from the research conducted by Uribe and others. 4
The inclusion criteria were; young adult patients (18-45 years old) undertaking orthodontic treatment in different private and public dental sectors. Self-administering methods were conducted in the distribution of the online survey among 200 orthodontic patients and their responses were recorded. Written informed consent was provided by each respondent, and the online interview was performed in agreement with the Declaration of Helsinki.
The following variables were assessed in this study:
Sociodemographic data, such as gender, age, educational level, and annual income.
Preferred extent of orthodontic treatment duration.
Preferences to undertake supplemental approaches accessible to accelerate orthodontic tooth movement and reduce treatment duration. The assessed procedures comprised; non-invasive (customized appliances and medications) and invasive (surgery) procedures.
Willingness to pay additional fees to shorten treatment period, inclination to pay for the various approaches accessible to reduce the treatment period, and the fee increment they are keen to pay to reduce treatment duration.
Statistical Analysis
Google Forms was utilized in data collection. Descriptive statistics were computed for percentages and frequencies. Group evaluations for gender differences were conducted using Mann-Whitney test. Analyses of data was performed via Excel (Microsoft Excel 2007, Microsoft Corporation, Redmond, WA, USA) and SPSS (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp, USA). Confidence level was set at 95% confidence level.
Results
One hundred orthodontic patients (50 males, 50 females) responded out of the 200 questionnaires distributed. The response rate was 50%.
Sample Distribution
The characteristics of the sampling population, which included gender, nationality, educational level, and annual income is shown in Table 1. About 70% were at the age range of greater than or equal to 18 to 25 years old, half of the respondents were male and had college degrees, 85% were Saudi and 56% had an annual income of <10 000 SR.
Characteristics of the Participants (n = 100).

Preferred duration of treatment
The respondents’ discernments toward the extent of treatment is shown in Table 2. Nearly three-fourths of the respondents agreed that the extent of treatment is taking a longer duration and about 51% of them wished that it could last for less than 6 months. No significant differences in preferences for orthodontic treatment duration was reported between gender (P > .05).
Frequencies and Percentages of Responses to Perceptions Toward the Duration of Orthodontic Treatment (n = 100).

Inclination to Undertake Supplementary Approaches
The respondents’ predilection for supplemental approaches for a 25% to 30% discount in duration is shown in Table 3. Customized appliances were reported to be the most convenient by 58% of the participants, followed by medications by 48%. On the other hand, surgery was reported to be the most inconvenient procedure as reported by 58% of the respondents. Substantial variation in ranking was not observed among both gender (P > .05).
Frequencies, Percentages, and Group Comparison According to Gender of Responses to Ranking the Preferences for Additional Procedures for a
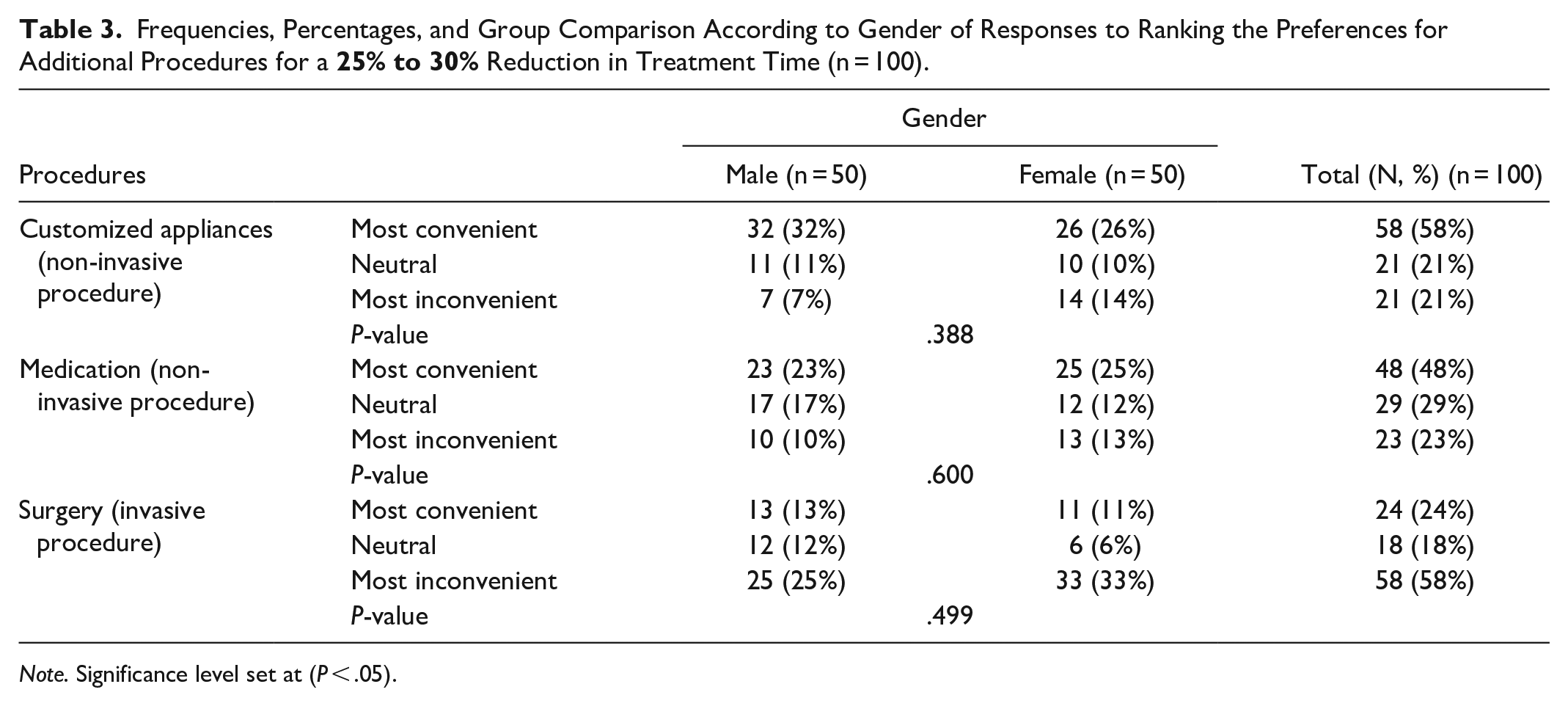
Note. Significance level set at (P < .05).
Capability and Inclination to Pay for Supplemental Approaches
Furthermore, the willingness of respondents to pay for each additional procedure is presented in Table 4. Respondents were more inclined to pay for medications (48%), which then followed by customized appliances (44%). On the other hand, 55% of the respondents were very not inclined to pay for surgery. No significant differences in willingness to pay was observed between gender (P > .05).
Frequencies, Percentages, and Group Comparison According to Gender of Responses to Willingness to Pay for Each Procedure Assessed (n = 100).

Note. Significance level set at (P < .05).
Likewise, their inclination to provide for the projected increment in fees for each supplemental approach sought to shorten treatment duration is shown in Table 5. Almost 70% of the respondents were not inclined to pay more than 20% increment for all proposed procedures (customized appliances, surgery and medication). No significant differences in willingness to pay was observed between gender (P > .05).
Frequencies, Percentages, and Group Comparison According to Gender of Responses to Willingness to Increase in Treatment Fees for Each Additional Procedure Claimed to Reduce Treatment time (n = 100).

Note. Significance level set at (P < .05).
Discussion
This study evaluated the perceptions of young adult orthodontic patients on orthodontic treatment factors such as cost, duration, and their willingness to undergo and pay for the various techniques and operations to hasten orthodontic tooth movement. In similar study conducted by Kim, about 63.2% of the adults interviewed, who were in their 20s, were interested in orthodontic treatment. Gender-wise, more female participants were interested as compared to male counterpart. However, there is no significant association between gender and positive interest in orthodontic treatment. 2 Linjawi et al, also found that females and patients aged between 18-25 years old were more interested in orthodontic treatment. 24
About 72% of the respondents agreed that the extent of orthodontic treatment is too long and about nearly half of them wished that it could last for less than 6 months. In addition, they preferred to undergo supplemental approaches for a 25% to 30% decline in duration with no significant differences between gender. Similar findings were also reported by Linjawi et al, although they had a broader age group and gender distribution. 24 Likewise, one-third of the adult patients interviewed by Uribe and others suggested that orthodontic treatment took longer duration and more than half of them wished that orthodontic treatment could last for 12 months or less. On the other hand, adolescent patients preferred shorter period of orthodontic treatment. 4
Customized appliances and medications were the most preferred procedure to be undergone by about half to 60% of the respondents, respectively. On the other hand, 58% of the patients were not willing to undergo surgery with no significant difference between gender. Likewise, many studies reported that less-invasive nonsurgical techniques and procedures were more preferred by patients.16-18,24
Results showed that 48% of the patients were more willing to pay for medications, followed by 44% were inclined to pay for customized appliances. Surgery was the least preferred orthodontic treatment technique as to which respondents were inclined to pay for. Financial concerns were deemed as an important factor considered by patients when choosing a treatment option.21,22 When asked for their inclination to provide for the projected increase in fees for each supplemental approaches sought to shorten duration, almost 70% of the respondents were not inclined to pay more than 20% additional fees for all proposed procedures (customized appliances, surgery, and medication). Uribe and others confirmed that most patients were inclined to provide for a maximum of 20% fee increment. Furthermore, the study thought that a boost in the tooth movement rate could be a potential dilemma for fee collection. 4 Results showed no significant association between gender and their willingness to pay additional charges for treatment claimed to reduce treatment duration.
Despite the differences in age groups included in all studies, findings of the current study and previous studies all confirmed that patients want to reduce orthodontic treatment time but are not welling to increase the treatment fees for more than 20% and are not welling to undergo invasive procedures.4,24 In contrary, Bindayel as well as Alansari et al surveyed a similar population for their willingness to pay additional fees for more esthetic orthodontic appliances. Both studies found that adult patients are willing to pay for more esthetic orthodontic appliances for their own but not for their children.21,25
This is a cross-sectional survey, thus, there might be a limitation of information bias. The patients might not be fully aware of the type of surgeries, medications, or customized appliances used to accelerate orthodontic tooth movement. Such lack of in-depth understanding might affect their responses. Further studies are needed to investigate the patients’ awareness with accelerated orthodontic treatment modalities.
Conclusion
The current study showed that both invasiveness of the procedural approaches as well as the financial concerns are the most predictive factors in patients’ acceptance to accelerated orthodontic tooth movement. Such finding will have a great implication on the direction of the orthodontic practice. The orthodontists as well as the manufacturing companies need to work hard to solve the challenges between reducing orthodontic treatment time and meeting patients’ abilities and concerns.
Footnotes
Ethical Statement
All procedures followed were in accordance with the ethical standards of the Ethical Committee of the Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia. Written informed consent was obtained from all patients for being included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.