
Abstract
Depression in older population is more common now. Due to increasing numbers of older patients in hospitals, nurses have more opportunities to care for these patients. Therefore, nurses should have correct knowledge of late-life depression and more favorable attitudes about depression. The study aimed to understand hospital nurses’ knowledge level of late-life depression and attitudes about depression. A cross-sectional research design was used. A convenience sample of 307 nurses from 3 hospitals in Taiwan was recruited. Nurses scored 55.15% in the Late-Life Depression Quiz. The average score of the Revised Depression Attitude Questionnaire was 71.76 (SD = 6.13). The study also found that hospital nurses had more favorable attitudes about depression when their late-life depression knowledge was higher; their interest level in providing care for older patients with depression was greater; they had ever taken care of older patients with depressive symptoms or depression; they had never received in-service training on depression in the past year; and they had ever attended lectures about depression in school. Hospital nurses’ knowledge about late-life depression was limited, and they had neutral to slightly favorable attitudes about depression in Taiwan. It is suggested to carefully examine and evaluate in-service training related to depression for nurses in hospitals. In addition, developing appropriate interventions to increase hospital nurses’ knowledge level of late-life depression and attitudes toward depression is recommended.
Depression in older population is common, but little is known about hospital nurses’ late-life depression knowledge level and attitudes about depression.
Nurses’ late-life depression knowledge in acute-care settings is inadequate, and nurses who had received in-service training on depression in recent 1 year had more negative attitudes toward depression.
Developing strategies to improve nurses’ late-life depression knowledge is recommended, and in-service training on depression should be examined and evaluated.
Introduction
Depression in older adults aged ≥65 years is a current health concern. Based on the World Health Organization1,2 (WHO)’s statistics, the prevalence rates of depression are beginning to peak during older adulthood, and it is estimated that around 7% of older people experienced depression globally. Moreover, a review article concluded that the median prevalence of depressive disorders among older persons from 74 studies with a total of 487 275 older people was 10.3% worldwide. 3 Although there are huge variations in prevalence values of depression or depressive symptoms in previous studies due to different assessment methods, assessment scales, and definitions even in the same country, this statistic suggests that depressive symptoms and depression among older populations have become a major mental health problem. Similarly, depression is also a serious issue among older adults in Taiwan. Previous studies revealed that 5.2% to 21.3% of community-dwelling older people suffer from depressive symptoms or depression.4,5
Depression is associated with older individual’s declining physical function, 6 but also affects older adults’ quality of life, 7 and is related to a higher risk of mortality. 8 The WHO 2 has identified depressive disorder as a major contributor to peoples’ disability and suicide deaths. Furthermore, previous studies also revealed that older adults’ depressive symptoms and depression were related to inpatient deaths, 9 length of hospital stay, 10 risk of hospital readmission, 11 and medication adherence in treating chronic diseases. 12 Consequently, health care costs and expenditures for depression care are remarkable. 13 Therefore, this mental disorder had better be screened, recognized, and treated at the earliest possible stage.
The number of hospital admissions among older populations is increasing, 14 so nurses who work in hospitals have more chances than before to care for patients who are aged ≥65 years. According to 2016 National Health Insurance Annual Statistics, 42% of hospitalized patients were older persons in Taiwan. 15 Most patients might be admitted to the hospital due to a disease or poor physical function, but attention should also simultaneously be paid to their psychological status by healthcare professionals. Ciro et al 16 found that 37% of hospitalized older patients had depression on admission. Even worse, the prevalence of unrecognized or untreated depression in older adults is significant. Padayachey et al 17 found that 40% of community-dwelling older adults who came to a local primary healthcare clinic were found to have depression which had previously not been identified. A longitudinal study also found that 71% of an older population (≥50 years) with depression was not prescribed antidepressant medicines or did not receive antipsychotic therapy. 18 Similarly, a study conducted in nursing homes also revealed that depression was underrecognized and undertreated. 19
Nurses are not trained well in late-life depression care. 20 One study suggested that home healthcare nurses need to have advanced training in depression care for older adults. 21 A systematic review article also concluded that nurses should receive training regarding delirium, depression, and dementia. 22 Therefore, current nurses’ knowledge levels of late-life depression should be understood first before any training. Moreover, nurses’ beliefs and values might influence what they want to do for patients in terms of their practice behavior. 23 Negative attitudes might prevent nurses from providing better quality depression care for older adults. Thus, it is also necessary to examine nurses’ attitudes toward depression. The purpose of this study was to describe hospital nurses’ knowledge level of late-life depression and attitudes toward depression, and associated factors.
Materials and Methods
This was a cross-sectional study. A self-report questionnaire was used to collect data.
Research Settings, Sampling, and Participants
A convenience sampling was applied in 3 hospitals in the Taipei area (northern Taiwan), including 1 medical center and 2 metropolitan hospitals. Inclusion criteria were registered nurses who were aged 20 years and older, practiced in general units in the hospital, had worked in the hospital for at least 1 month, and could read Chinese. Exclusion criteria were nurses who worked part time or who worked in the intensive care unit, pediatric unit, or psychological unit. The sample size was determined for this study by using G*power. In total, 360 questionnaires were picked up, and 353 were completed (98% response rate). Finally, 307 questionnaires were valid.
Instruments
The instruments included a demographic questionnaire, the Late-Life Depression Quiz (LLDQ), and the Revised Depression Attitude Questionnaire (R-DAQ).
The 13-item LLDQ 24 is a modified version of the original instrument developed by Pratt et al. 25 In the current study, the 13-item Chinese version of the LLDQ was used 26 to measure nurses’ knowledge level of late-life depression. The responses were “yes,” “no,” or “don’t know.” One point was given for a correct answer, and 0 points for a wrong one or “don’t know” answer. The score ranged from 0 to 13. A higher score on the LLDQ indicates that nurses had a higher knowledge level on late-life depression. The value of Kuder-Richardson Formula 20 (KR-20) was 0.74.
The 22-item Chinese version of the R-DAQ 26 was used in the current study. The R-DAQ was modified by Haddad et al 27 from the Depression Attitude Questionnaire. 28 This scale uses a 5-point Likert scale ranging from strongly agree (5) to strongly disagree (1) to measure participants’ attitudes toward depression. Some negatively worded items were recoded in reverse. A higher score (which ranges 22-110) represents more favorable attitudes about depression. The coefficient alpha of the R-DAQ was 0.84. 27
Data Collection Procedures
Researchers contacted hospitals by phone and obtained the approval from the hospitals. Then, researchers introduced the research purpose, inclusion criteria, data collection methods, and study risks and benefits to nurses during a staff meeting. This information was also included on the first page of the questionnaire. Nurses who were interested in participating in the study could pick up a questionnaire and return it to an envelope placed in the nursing station after completing it. Returning the questionnaires indicated a nurse’s agreement to participate in the study. The data were collected from January to March, 2016.
Data Analysis
Data analyses were conducted using SPSS for Windows Version 18.0 (SPSS, Chicago, Illinois) and included percentage, mean, standard deviation, t test, and Pearson’s product-moment correlation. A stepwise regression was used to examine the association of nurses’ attitudes toward depression, and their demographic information and their knowledge level of late-life depression. A p value less than .05 was considered statistically significant.
Ethical Considerations
This study was approved by the institutional review board at one university (N201512032). All participants’ rights were protected. Participation was voluntary, and participants did not need to complete or return the questionnaire if they did not want to participate in this study during the data collection period.
Results
Participants’ Demographic and Characteristics Data
The average age of nurses was 27.49 (SD = 6.19) years, and their average length of nursing experience was 5.68 (SD = 5.75) years. Most participants were women (98%) and had a bachelor degree or above (61.2%). Average scores of the level of interest in nursing, in providing care for older patients with depression, and in issues about late-life depression (these 3 variables were measured using a 5-point Likert scale) were 3.52 (SD = 0.71), 3.03 (SD = 0.8), and 3.41 (SD = 0.69), respectively.
Around two thirds of nurses did not attend any depression (66.4%) or late-life depression (72.6%) classes or courses in school. In the past 1 year, 72.6% of nurses had never attended a depression in-service training or program and 87% of nurses did not attend any late-life depression in-service training course or program. In total, 118 participants (38.4%) had ever read educational information or pamphlets regarding late-life depression. There were 62.2% of nurses who had experiences in providing care for older patients with depressive symptoms or depression (Table 1).
Demographic Data and Characteristics of Participants (N = 307).

Nurses’ Late-Life Depression Knowledge, Attitudes Toward Depression, and Associated Factors
The mean score on the late-life depression scale was 7.17 (SD = 2.10; max = 0, min = 12; full score is 13) with 55.15% correct answers among all questions. The average score of the R-DAQ was 71.76 (SD = 6.13; max = 53, min = 92).
There were no significant differences in nurses’ knowledge and demographic and characteristic variables. However, nurses’ attitudes toward depression significantly differed between those who had ever attended a depression lecture in school or not (t = −2.474, p = .014), and those who had ever read educational information or pamphlets regarding late-life depression or not (t = −2.628, p = .009).
There was a significant positive relationship between nurses’ late-life depression knowledge and interest level in nursing (r = 0.119, p = .037). In addition, there were also positive relationships between nurses’ attitudes toward depression and a couple of variables including their interest level in nursing (r = 0.213, p < .001), their interest level in providing care for older patients with depression (r = 0.226, p < .001), their interest level in issues regarding late-life depression (r = 0.219, p < .001), and their knowledge level of late-life depression (r = 0.272, p < .001).
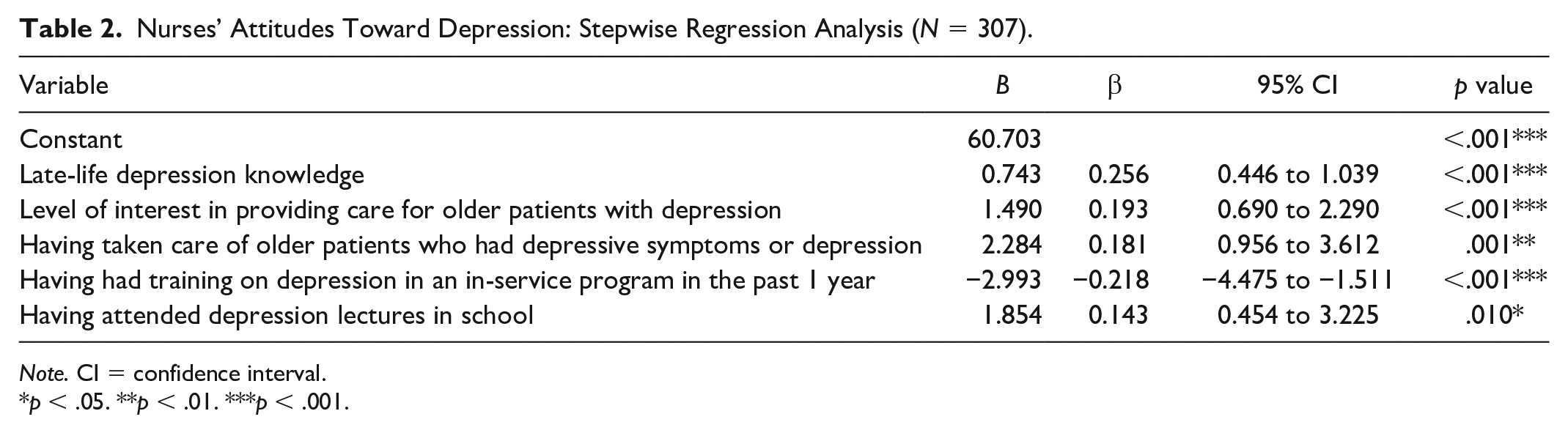
Variables entered into the stepwise regression analysis were selected based on their statistical significance found above and on the researchers’ experience. This study revealed that nurses’ attitudes toward depression were associated with their knowledge level of late-life depression (B = 0.743, p < .001), interest level in providing care for older patients with depression (B = 1.490, p < .001), ever having taken care of older patients who had depressive symptoms or depression (B = 2.284, p = .001), having received in-service training on depression (B = −2.993, p < .001), and having attended depression lectures in school (B = 1.854, p = .010). The results of regression indicated these 5 variables explained 19% of the variance (F = 14.76, p < .001; Table 2).
Nurses’ Attitudes Toward Depression: Stepwise Regression Analysis (N = 307).
Note. CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Discussion
The current study indicated that hospital nurses’ late-life depression knowledge was insufficient (55.15% correct). Pullen 29 used the same instrument (LLDQ) to examine late-life depression knowledge of staff in long-term care facilities in the United States. Similarly, this previous study found that nursing staff obtained 62% on the LLDQ and also found that staff who had a higher educational level had higher scores on the knowledge quiz. The authors also compared differences in knowledge scores between nursing staff (62% correct answers) and non-nursing staff (61.5% correct answers) and found that there was no statistical difference in these two populations. One recent study 26 using the same instrument revealed that nurses in long-term care facilities got 55.92% correct answers. Another study found that 60% nurses had insufficient knowledge to manage patients with depression. 30 However, other studies indicated that nurse practitioners in a primary care setting 31 and advanced practice nursing students 32 had better scores on knowledge about late-life depression. A study that examined the effectiveness of a training program on nurses’ knowledge of, attitudes toward, and practice changes concerning late-life depression also indicated that primary care nurses’ late-life depression knowledge improved after the training program from 8.25 (68.75% correct answers) to 10.73 (89.42% correct answers). 33 On comparison of our findings to previous studies, hospital nurses in Taiwan had poor knowledge of late-life depression. Consequently, nurses might easily neglect some important symptoms or signs of depression and have difficulty providing appropriate care. Strategies for improving nurses’ late-life depression knowledge in acute-care settings should be developed.
Nurses had slightly positive attitudes toward depression found in the current study. Consistent with 2 previous studies, Delaney and Barrere (2012) found that advanced practice nursing students had positive attitudes toward depression care, and Haddad et al 34 also found that district nursing staff had positive attitudes toward depression. Contrarily, other studies indicated that nurses have less-favorable attitudes about depression. One study revealed that more than half of the nurses expressed an unfavorable attitude toward managing patients with depression, and only 15% of nurses showed a favorable attitude about depression management. 30 Similarly, Scheerder et al 35 found that nurses had more negative attitudes toward depression than physicians and mental health professionals in 9 countries. One recent study also reported that primary health care providers including pharmacy attendants, general practitioners, social workers, and nurses had negative views regarding depression. 36 Furthermore, in addition to holding positive or negative attitudes about depression, nurses might also possess a neutral attitude toward depression. 37 Based on the previous and current studies, there is still no consistent conclusion on nurses’ attitudes about depression, so a meta-analysis study should be conducted in the near future.
Using a stepwise regression, this study found that hospital nurses had more favorable attitudes about depression when their late-life depression knowledge was higher; their interest level in providing care for older patients with depression was greater; they had ever taken care of older patients with depressive symptoms or depression; they had never received in-service training on depression in that past year; and they had ever attended lectures about depression in school.
A lot of evidence indicates that there are positive relationships between nurses’ knowledge and attitudes, regardless of their knowledge of or attitudes about depression26,30 or other variables, such as later life sexuality 38 or palliative care. 39 While nurses have more correct knowledge of disorders, symptoms, or the method of management or care, they might have more positive attitudes toward a particular variable.
Nurses who had ever taken care of older patients who had depressive symptoms or depression had more favorable attitudes toward depression. This finding shows that nurses’ practical experience gave them more opportunities to be with these adults and might help them more thoroughly understand depression. Nurses might easily empathize with or feel the same way about patients who had depressive symptoms or depression. Moreover, nurses’ past experience might help them in providing care and knowing what might happen next. Similarly, a study found that nursing students with the experience of providing care for dying patients had more positive attitudes about caring for the dying. 40
Nurses who had ever attended depression lectures in school had more favorable attitudes toward depression. This finding emphasizes that nurse faculty members at schools should arrange lectures or courses related to depression for nursing students, not only to increase their knowledge of depression but also to cultivate positive attitudes toward depression. Surprisingly, nurses who had never received in-service training on depression in the recent 1 year had more positive attitudes toward depression in hospitals. A previous study reported that a Web-based educational intervention did not improve nurses’ beliefs about depression in patients with heart failure. 41 The author suggested conducting face-to-face workshops instead of Web-based tutorials for better outcomes in the future. On the contrary, Butler and Quayle 33 found that a face-to-face training program lasting for 2 days was effective in increasing primary care nurses’ late-life depression knowledge and improving their attitudes about depression. Therefore, in-service training in hospitals mihgt need to consider not only the contents but also the delivery methods and length of the training.
Limitations
The sample was from 3 hospitals in the Taipei area, so the results cannot be generalized to all nurses in Taiwan. It is suggested that a national survey should be conducted in the future. However, to the best of our knowledge, there are few articles attempting to understand nurses’ knowledge level of late-life depression and attitudes toward depression in hospitals, so the current study can still provide valuable information for future research and clinical practice.
Conclusions
Hospital nurses’ knowledge about late-life depression was limited, and they had neutral to slightly favorable attitudes about depression. Moreover, nurses had more favorable attitudes about depression when their depression knowledge was higher; their interest level in providing depression care for older patients was greater; they had ever taken care of older patients with depression; they had never received in-service training on depression; and they had ever attended lectures about depression in school. Because the number of patients who are aged ≥65 years is increasing in hospitals, nurses, the main direct care providers, need to have correct knowledge of and positive attitudes toward depression to identify potential patients and provide appropriate care. The findings suggest that in-service training on depression should be examined and evaluated considering delivery methods and length of the training in hospitals. Moreover, further research on developing appropriate interventions to increase nurses’ knowledge level about late-life depression and attitudes toward depression in acute-care settings is recommended at the earliest possible stage.
Footnotes
Acknowledgements
The authors thank the 3 hospitals and the nurses who completed the questionnaires. Moreover, authors also thank the Ministry of Science and Technology in Taiwan for financial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology in Taiwan (grant no.: MOST 104-2815-C-038-033-B, 2015).