
Abstract
Few researches have been focused on the treatment delay of rural-to-urban migrants in China. Our study aimed to investigate the effect of migration duration on treatment delay among rural-to-urban migrants in tertiary hospitals. A cross-sectional study was conducted based on a sample of 727 patients and surveyed factors including sociodemographics, medical costs, migration, treatment delay, and health cost-coping strategies. Totally, 727 patients were included, of which 61 delayed their treatment and 666 had no treatment delay. Statistically significant differences were found between different migration duration groups in marital status, education, insurance, family annual income, residency, payment before treatment, reported disease, and migration duration (P < .05). The results from multiple logistic regression showed that migration between 1 and 5 years (adjusted odds ratio [OR] = 7.24; 95% confidence interval [CI] = 1.59-32.87; P < .05) was considered the significant contributing risk factor for treatment delay after adjusting for age, sex, and other variables. To cope with their health expenditure, patients with treatment delay tended to use less savings and borrow more money than those without. Rural-to-urban migrants with 1 to 5 years of migration were the most vulnerable group of having treatment delay. Migrants were more likely to borrow money to cope with the health expenditure. Targeted services should be provided to meet different needs of migrants according to migration duration.
Previous studies showed that treatment delay was related mainly with sociodemographic factors, socioeconomic status, clinical variables, and psychological factors.
This study added some new knowledge to the effect of migration on treatment delay: Rural-to-urban migrants with 1 to 5 years of migration were more likely to have treatment delay.
Targeted services should be provided to meet different needs of migrants according to migration duration.
Introduction
In China, the proportion of urban population increased to 56% in 2015, and more than 30%, roughly 247 million who are living in urban areas, are migrants. 1 China is now initiating a new round of urbanization on an unprecedented scale boosted by significant reform on household registration. 2
Urbanization not only can change environment, but also people’s lifestyle, which can directly lead to various health problems. The health consequences followed by urbanization are mixed. Current studies reveal the phenomenon called “healthy migrant paradox,” that is, migrants have physical health advantages over the native-born at the initial stage of the immigration. However, the migrant health advantage diminishes significantly with increasing resident time in the host society.3-6 The huge scale of migration has generated particular difficulties for health service delivery in China. 7
In 2016, China initiated the merge of urban and rural health insurance schemes to tackle the inequity caused by separated rural and urban health care schemes which vary in funding, deductibles, and so on. 8 However, pilot experience showed that the merge varied from province to province. In many cities, pooling funds were still controlled in county level. 9 Also, whether the merge of urban and rural health insurance results in improving migrants’ health service use remains less explored.
Although the vast majority of patients have been protected by health insurance, many low-income and minority patients (many of them are migrants from rural areas) had to pay a certain amount, often the entire amount of money prior to treatment, given the fact that the profit-driven public hospital worries the potential risk of being in debt if they treat patients in advance.10,11 Many households experience financial hardship as a result of delayed necessary treatment.12,13
Most of the studies focusing on treatment delay were under the concept of patient’s delay—the length of delay between the onset/discovery/recognition of signs and symptoms and a patient’s first visit to a health care/medical provider. 14 Many studies showed that the patient’s treatment delay was related mainly with sociodemographic factors, socioeconomic status (SES), clinical variables, and psychological factors.15-18 However, few studies looked into the effect of migration on treatment delay (the delay between being told to be hospitalized/receive a major treatment and a patient’s hospitalization/getting a major treatment done). This study aims to investigate the relationship between rural-to-urban migration and treatment delay after the integration of urban and rural health insurance schemes in China.
Methods
Conceptual Framework
The conceptual framework of this study is on the basis of the revised and expanded Behavior Model for Vulnerable Populations originated from the well-known Andersen Health Service Utilization Model.19,20 Andersen21,22 introduced the model in 1968 and had undergone several phases of updates over time. According to the model for vulnerable populations, the factors that make some populations vulnerable might also affect health services utilization and health status. We assumed that migrants, as a vulnerable population, and their use of service might be affected by 3 sequential clusters of factors: predisposing, enabling, and need factors in 2 domains (traditional and vulnerable domains) (see Figure 1). In this study, predisposing factors (predisposition to use health services) include demographic characteristics (age, sex, marital status), social structures (education, occupation), and vulnerable social structure (immigration). The enabling factors (impede the use of health services) include personal resource (insurance and income), community resource (residency), and vulnerable personal resource (payment before treatment—as an ability to negotiate). Need factors include reported diseases and vulnerable population. The outcome variable is whether the patient uses inpatient treatment in time or not.
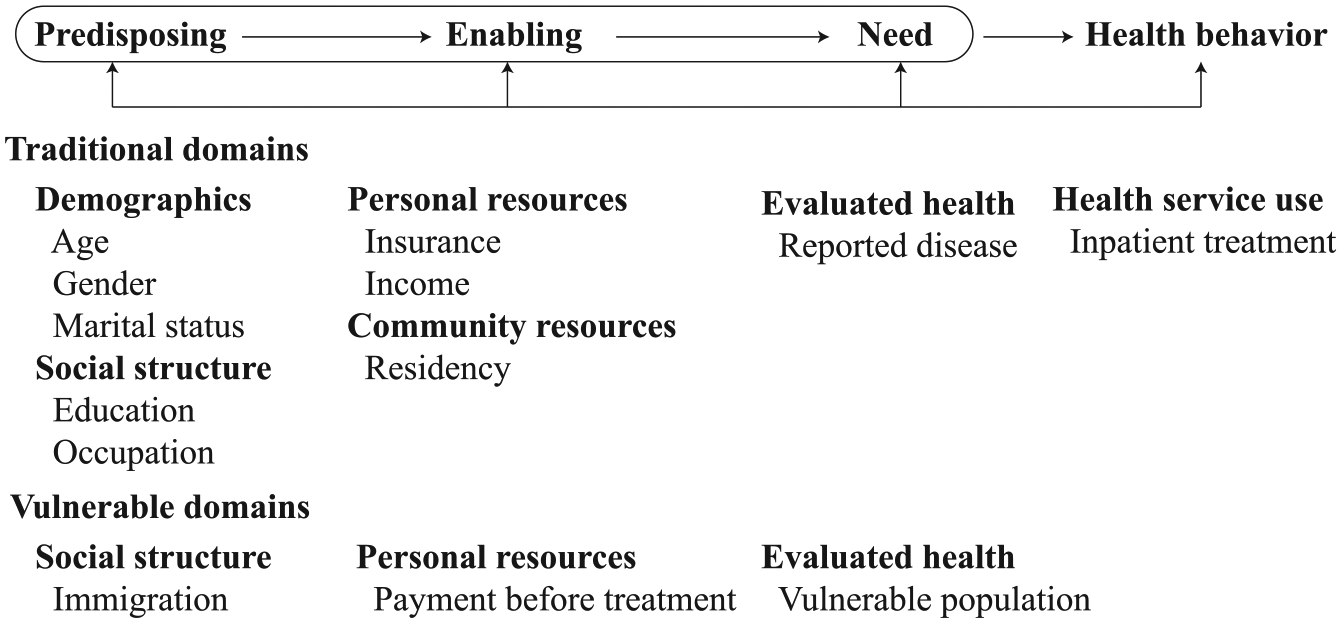
The conceptual framework based on the Andersen Health Service Utilization Model including the selected variables in this study.
Region
Recently, it is noticeable that a fast growth occurred in the midwest China, which contributed up to a 43.6% increase in migrants. 23 In Western China, migrants accounted for 19.5% of the total migrants in 2015, a 5.3% increase compared with the year of 2014. 24 So, the study was conducted at Jiujiang city in Jiangxi province of China which is located in the midwest region of China. The city was subdivided into 10 counties and had a population of 4 million. To sample patient with various diseases, we purposively chose 2 general tertiary hospitals out of a total of 6 tertiary hospitals. Both hospitals were the top hospitals with more than 1500 beds.
Data Management and Measurement
The design was a hospital-based cross-sectional study. The study population consisted of all patients with or without urban household registration who were hospitalized in the selected 2 tertiary general hospitals in Jiujiang City between January 2017 and December 2018, or their direct relatives who were willing to participate in this study with the following inclusion criteria: hospitalized ≥1 time and age ≥ 18 years, and only 1 exclusion criteria: diagnosed with mental illness.
Consecutive sampling was used. Each participant who met the inclusion criteria was included till the desired sample size is reached. Sample size calculation was based on the 5% difference in the proportion of having negative care-seeking behavior between migrants and nonmigrants with 2.5% precision at 95% confidence interval (CI) and 80% power. The calculation was completed using the “epicalc” package in R software (version 3.5.2). A total of 500 admitted cases are needed considering a 10% nonresponse rate. The details of the calculation are as follows: For testing 2 independent proportions (2-tailed test), the main outcome was the proportion of having delayed care-seeking behavior. Based on the statistics from the Mobile Population Social Integration and Mental Health Survey (MPSIMHS), the proportion for the 1- to 5-year migration group was estimated as p1 = 0.25, and the <1 year and no migration group as p2 = 0.05, ratio (r) = 10 (n2/n1), α = 0.05, Z(0.975) = 1.959964; β = 0.20, Z(0.800) = 0.841621. Sample size using a continuity correction: 1- to 5-year migration group (n1) = 25, <1 year and no migration group (n2) = 250.
The questionnaire used for the face-to-face interview consisted of 4 parts. The first part was general information on sociodemographic characteristics. The second part contained the care-seeking behavior and health care cost of the latest admission. The third part was the information on monthly and annual family income and expenditure. The fourth part contained medical record and financial bill of the latest admission information obtained from the hospital information system.
For the main independent variable—migration duration (length of residence after moving from the rural to the urban area), participants were asked a question how long they had moved from the rural to the urban area.
For the main outcome variable—treatment delay, patients who reported treatment delay were considered having a treatment delay. 25 Patients were asked a set of questions: Did you delay the hospitalization and major treatment for current inpatient admission; when were you told by your doctor that you needed to be hospitalized; and when are you told by your doctor that you need the major treatment? Then the information with the actual admission and treatment date was verified using the data extracted from the hospital information system.
Data Analysis
Both descriptive and analytical statistics were employed. Generalized linear models (GLMs) were used to test the relationship between treatment delay and migration, along with other independent variables, such as age group, sex, marital status, job type, residency, income provider (major contributors to household income), health insurance, and health expenditure. Inference was made based on the chi-square test in univariate analysis. A P value less than .05 suggests that there is a significant difference among different categories.
The best fitted multivariate model was met by stepwise variable selection based on Akaike information criterion (AIC). First, we select the possible variables based on the conclusions of previous similar studies and univariate analysis between 2 groups. Then we applied stepwise model selection to looking for a better fitted model. Last, we decided the final variables on the basis of statistical model selection based on AIC and suggestion from other studies. The 95% CI and P value were calculated in the logistic regression model. The likelihood ratio test and Wald test were used to test the statistical significance of the variable in the logistic regression model. A P value less than .05 suggests the statistical significance of a variable in the model. All statistical analyses were conducted using the R software version 3.5.2.
Ethical Consideration
This study was conducted according to the World Medical Association Declaration of Helsinki and conformed to the International Committee of Medical Journal Editors’ (ICMJE) Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals. Ethical approval was obtained from Institutional Review Ethics Committee of Prince of Songkla University (REC: 59-266-18-5***) and Ethics Committee of *** Jiujiang University (REC: JJU20160116***). Every participant’s consent was obtained with a written consent form signed by the patient or their legally authorized representatives. Great care was taken to secure the confidentiality of participants. Data from the hospital information system were disaggregated. Informed consent was obtained from all participants in hospitals. The participants had the opportunity to quit the survey at any time and to review and correct their own answers.
Results
Table 1 shows the comparison of sociodemographic characteristics among different migration duration groups. There were statistically significant differences between different migration groups in age, education, and residency (P < .05). And 66.67% of patients with 1 to 5 years of migration were below the age of 50.
Sociodemographic Characteristics of the Studied Participants (N = 727).

Univariate analysis was performed to explore possible factors related to treatment delay (Table 2). Totally, 727 patients were included, of which 61 delayed their treatment and 666 had no treatment delay. There were statistically significant differences between different migration groups in marital status, education, insurance, family annual income, residency, payment before treatment, reported disease, and migration duration (P < .05). Results showed that 7 (23.33%) single patients had delayed treatment; 41 (11.82%) patients with primary and lower education reported delayed treatment; 28 (11.86%) patients not covered by integrated urban and rural insurance reported delayed treatment; 45 (11.08%) patients living in rural area reported delayed treatment; 34 (11.07%) patients with 10 000 to 50 000 Yuan family annual income reported delayed treatment; 49 (10.17%) patients paid more than 75% cost before treatment delay; 8 (34.78%) patients with cancer reported delayed treatment; among 1- to 5-year migrants, 6 (22.22%) had treatment delay, whereas 51 (8.32%) reported in <1 year migrants and non-migrants.
Logistic Regression for the Factors Related to Treatment Delay.
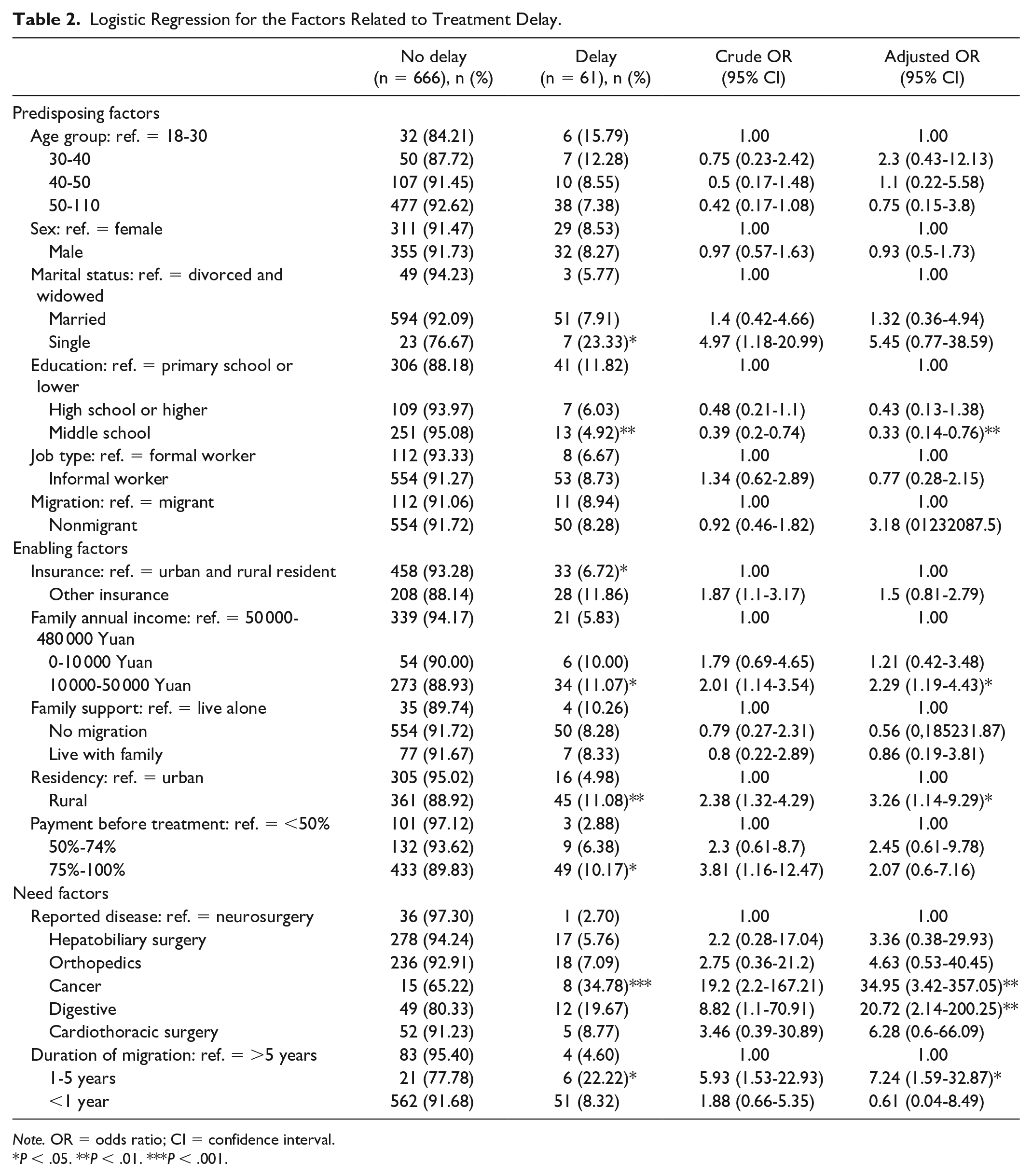
Note. OR = odds ratio; CI = confidence interval.
P < .05. **P < .01. ***P < .001.
Odds ratios (ORs) for treatment delay were adjusted for age, sex, marital status, education, job type, migration, insurance, family annual income, family support, residency, payment before treatment, reported disease, and migration duration using multiple logistic regression.
Multiple logistic regression method was used to investigate the potential risk factors in the multivariable analyses (Table 2). After the model selection, the best model includes 13 independent variables (age, sex, marital status, education, job type, migration, insurance, family annual income, family support, residency, payment before treatment, reported disease, and migration duration).
Education, family annual income, residency, reported disease, and migration duration were the variables in multiple logistic regression to be significantly associated with treatment delay. Having middle school education was associated with a 67% decreased odds of treatment delay compared with having primary and lower education. Compared with patients with family annual income more than 50 000 Yuan, those with family annual income ranging from 10 000 to 50 000 Yuan had higher odds of treatment delay (adjusted OR = 2.29; 95% CI = 1.19-4.43; P < .05). In the rural setting, there was a trend toward increased treatment delay that was statistically significant (adjusted OR = 3.26; 95% CI = 1.14-9.29; P < .05). Compared with patients having neurosurgery, those with cancer (adjusted OR = 34.95; 95% CI = 3.42-357.05; P < .01) and digestive system diseases (adjusted OR = 20.72; 95% CI = 2.14-200.25; P < .01) had higher odds of treatment delay. Patients with 1 to 5 years of migration had higher odds of treatment delay (adjusted OR = 7.24; 95% CI = 1.59-32.87; P < .05) compared with those with more than 5 years of migration. Among patients who paid more than 75% cost before treatment, there was a trend toward increased treatment delay that was not statistically significant (adjusted OR = 2.07; 95% CI = 0.6-7.16; P = .25).
Age, sex, marital status, job type, migration, insurance, and family support were not associated with treatment delay in multiple logistic regression analysis.
There were 2 significant differences between patients with and without treatment delay. In total, 33 (54.1%) in the delay group used savings to cope with their health expenditure, and 458 (68.8%) in the no delay group; 46 (75.4%) in the delay group borrowed money, and 301 (45.2%) in the no delay group (Figure 2).
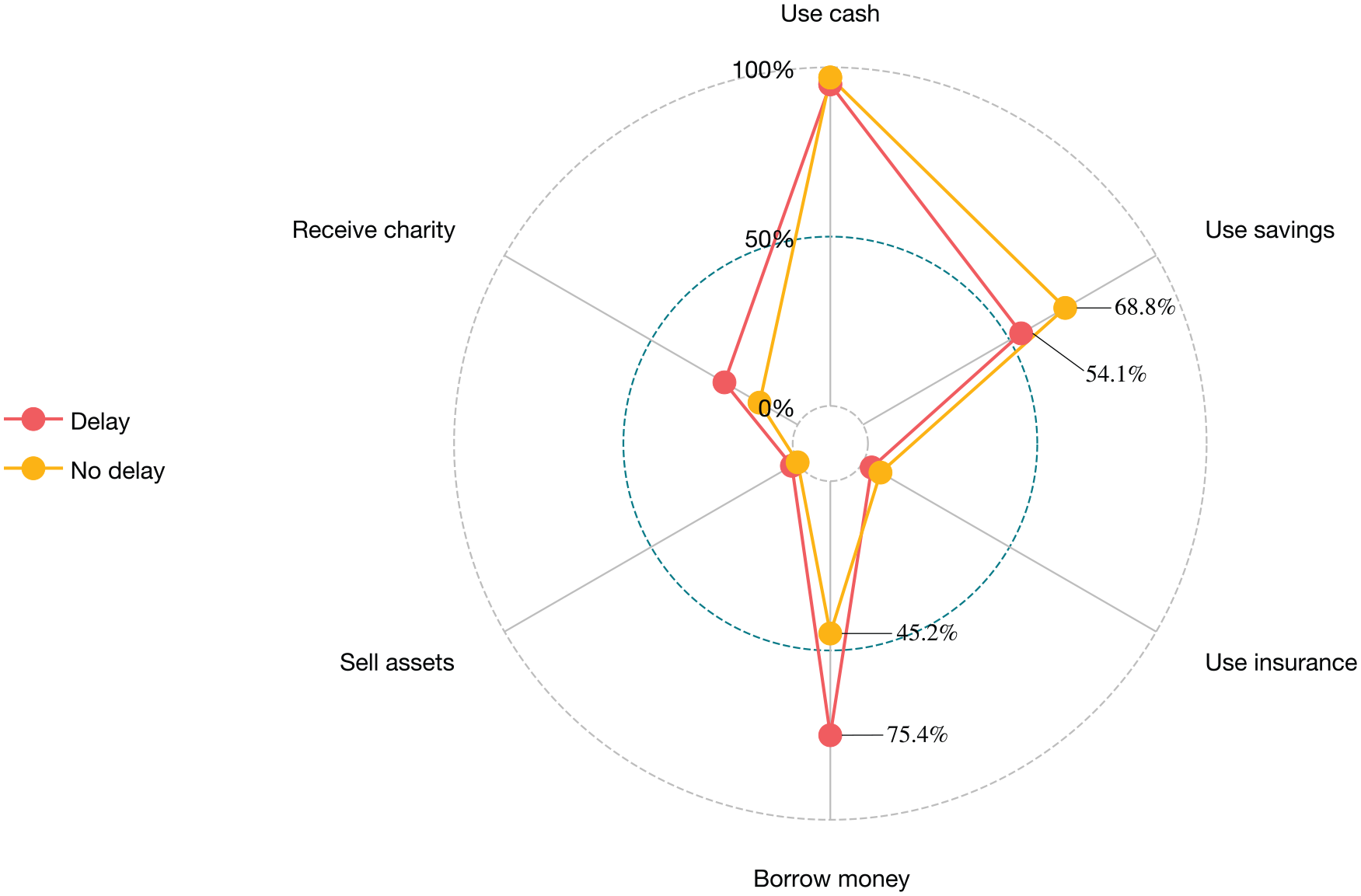
Cost-coping strategy between patients with treatment delay and no delay.
Patients with different migration durations also showed various preferences when dealing with health expenditure. Among patients with more than 5 years of migration, 48 (55.2%) used savings to cope with their health expenditure, 18 (66.7%) among patients with 1 to 5 years of migration, and 425 (69.3%) among patients with less than 1 year or no migration; 26 (29.9%) patients with more than 5 years of migration borrowed money, 12 (44.4%) among patients with 1 to 5 years of migration, and 309 (50.4%) among patients with less than 1 year or no migration (Figure 3).

Cost-coping strategy among different migration duration groups.
Discussion
After the integration of urban and rural health insurance schemes, even the rural-to-urban migrants without urban household registry were entitled to get expanded the medication and services; moreover, patients now could get the reimbursement back right before they were discharged. The result in this study presented that the probability of having treatment delay was decreased among patients covered by integrated urban and rural insurance, which might result from the expanded benefit packages and instant reimbursement policy after the integration of urban and rural insurance.
Despite the benefits provided by the integrated insurance, our study found some evidence indicating that the rural-to-urban migrants should receive special attention.
First, this study showed that most of the migrants, especially among migrants living in an urban area for 1 to 5 years, were young and middle-aged labors. The result also showed that migrants were more likely to face the risk of having treatment delay, especially those have lived in urban area for 1 to 5 years. The young and middle-aged migrants are usually the main income provider for their family, and their health-related financial risk can put an extra burden on patients and their family, who not only have to tolerate medical treatment cost but also suffer from the income loss due to absenteeism to work. 26 Under this circumstance, they will take more time to make decision whether to use inpatient care or major treatment that can lead to treatment delay. Our study also showed that with the increasing duration of migration, fewer patients used savings and borrowed money to cope with the health expenditure, which indicate that patients with longer migration are more likely to get a formal job and covered by employee health insurance. Targeted services should be provided to meet different needs of migrants according to migration duration.
It was also noticeable that there were more patients paid more than 75% cost before treatment in the delay group, and patients with treatment delay were less likely to use savings to cope with their health expenditure, most of which also needed to borrow money. For the low-income family, they may need to delay the treatment to raise money to pay for the cost. Reducing payment before treatment might serve as a vehicle to provide timely treatment for migrants. Early education about medical crowdfunding might help patients collect the money for treatment in time and prevent bankruptcy.27-29
Third, between the delay and no delay groups, there were many differences in marital status, education, insurance, family annual income, residency, payment before treatment, and reported disease, which were consistent with other studies15,30-32: being single, having less education, living in rural area, and low family annual income were more likely to have treatment delay.
Finally, this study also indicated that patients with cancer and digestive system diseases might delay their treatment. Because the disease or the treatment was not as emergency as neurosurgery, patients were more likely to delay the treatment for alternative solution.
Limitations
Our study had some limitations. First, all cases were selected from 2 tertiary hospitals in 1 city, so the conclusion might be difficult to be generalized to a larger scale. Second, socioeconomic determinants related to treatment delay were dynamic factors, which might be different over time and from country to country. The interaction between migration and other factors might react differently under changing social context. Our findings may not be generalized to all migrants in China and in other countries. Third, social capital, social support, and social integration were also proved to be related to health-seeking behavior, but we could not collect the above information due to limited time and resources. However, this is the first study to test the relationship between migration duration and treatment delay.
Conclusions
This study added some new possible factors contributing to the treatment delay. Rural-to-urban migrants in different migration groups showed different probabilities of having treatment delay, and those who have 1 to 5 years of migration were the most vulnerable group; payment before treatment may also serve as an obstacle to timely treatment. Migrants were more likely to borrow money to cope with the health expenditure. Targeted services should be provided to meet different needs of migrants according to migration duration.
Footnotes
Acknowledgements
The authors would like to thank the Jiujiang University Affiliated Hospital and Jiujiang First People’s Hospital for data collection.
Author Contributions
L.N. analyzed the results; Y.L. helped with the investigation; H.L. and J.C. provided technical support with hospital data analysis; and X.W. and H.S. reviewed the manuscript.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant nos 71864020), the Education Department of Jiangxi Province (grant no GJJ170957), and the China Medical Board (grant no 16-261).